
Abstract
Background:
Post-infarction ventricular septal defects require surgical closure. Only a few studies have been conducted in Asian populations. This study reports the current outcomes and determinants affecting survival.
Methods:
Between January 1995 and January 2012, 40 patients underwent surgery for post-infarction ventricular septal defect. We analyzed demographics, clinical, angiographic, and echocardiographic parameters, operative data, postoperative morbidity, and survival. Mean follow-up was 5.2 ± 5.3 years. Univariate and multivariate analyses were used to determine the factors affecting 30-day mortality and long-term survival.
Results:
There was no intraoperative death. Our 30-day mortality was 20%. Single-vessel disease was found on coronary angiography in 63% of patients. Eight patients had concomitant coronary artery bypass grafting. Overall survival at 1, 5, and 10 years was 68%, 55%, and 42%, respectively. Event-free survival from subsequent angina, myocardial infarction, congestive heart failure, or percutaneous interventions at 1, 5, and 10 years was 66%, 43%, and 25%, respectively. Preoperative oliguria and postoperative sepsis were independent predictors of 30-days mortality on multivariate analysis (p = 0.02). Preoperative left ventricular function was associated with long-term survival (p = 0.048).
Conclusion:
We had good results of current postinfarction ventricular septal defect repair. Selected patients had concomitant coronary artery bypass grafting. Preoperative oliguria and postoperative sepsis were independent predictors of 30-day mortality, while left ventricular function was related to long-term survival.
Keywords
Introduction
Ventricular septal rupture complicates less than 1% of all cases of acute myocardial infarction, but is nonetheless a serious and fatal complication. 1 Nonoperative treatments for post-infarction ventricular septal defect (VSD) have poor results. Historical reviews have shown that 50% of patients died within 1 week, 80% within 4 weeks, and less than 10% survived beyond 1 year. 2 Surgical repair of post-infarction VSD is the definitive treatment of choice. 3 Several small series have been described in Asian populations.4–8 Prognostic factors for post-infarction VSD repair have been studied in Western publications.9–12 Nevertheless, such determinants may not apply to Asian populations because the disease pattern may differ between Asian and Western populations. This study aims to report the latest outcomes and determinants of survival in patients who underwent post-infarction VSD repair surgery.
Patients and methods
Demographics, clinical features, and preoperative data of 40 patients with post-infarction ventricular septal defect.
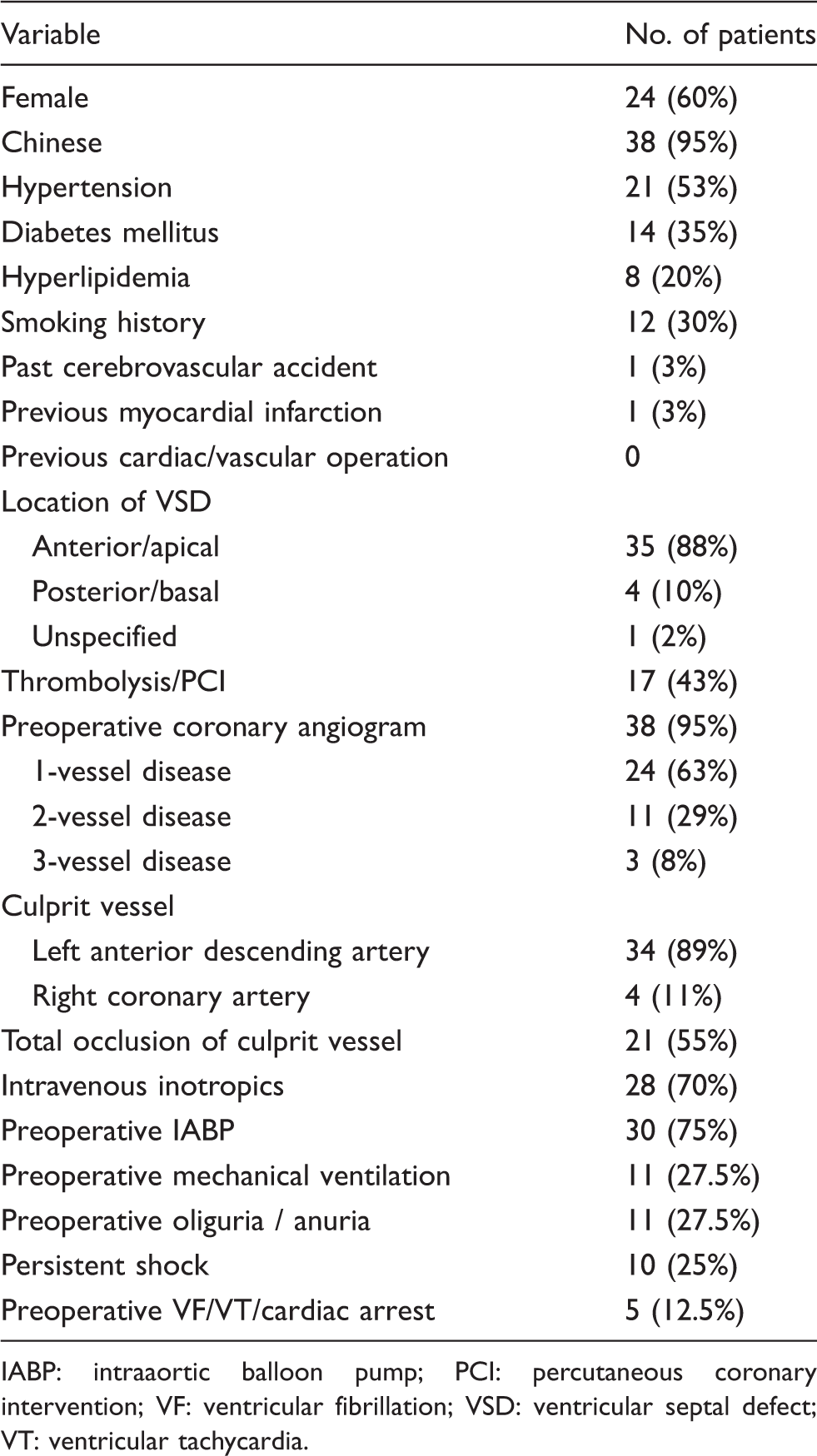
IABP: intraaortic balloon pump; PCI: percutaneous coronary intervention; VF: ventricular fibrillation; VSD: ventricular septal defect; VT: ventricular tachycardia.
Perioperative data were retrieved retrospectively from hospital records. The diagnosis of post-infarction VSD was made a median of 2 days (range, 0–9 days) after the diagnosis of acute myocardial infarction. The VSD were located in the anterior or apical septum in 35 (88%) cases and the posterior septum in 4 (10%). Seventeen (42.5%) patients were treated with primary percutaneous coronary interventions or thrombolytic therapy prior to surgery. Preoperative coronary angiograms were performed in 38 (95%) patients. The coronary artery disease pattern is shown in Table 1. Mean left ventricular ejection fraction (LVEF) on preoperative echocardiography was 56%. Preoperative inotropic support was required in 28 (70%) patients. An intraaortic balloon pump (IABP) was used in 30 (75%) patients. Eleven (28%) patients were intubated for mechanical ventilation before surgery. Five (13%) patients suffered cardiac arrest or ventricular arrhythmias before the operation. Despite hemodynamic support, 11 (28%) patients had oliguria or anuria, and 11 (28%) had persistent shock (systolic blood pressure ≤90 mm Hg) preoperatively.
Emergency operations (on admission) were carried out in 17 (43%) cases, and urgent operations (next day) in 11 (28%). Nine (23%) patients had a period of stabilization before surgery (semiurgent operations). Two patients in our cohort had chronic postinfarction VSD. They were discharged home with medical therapy and readmitted for operations 3 and 8 months later. In the acute cases, mean time from VSD diagnosis to repair was 3 days (median, 1 day; range, 0–19 days). All procedures were performed under cardiopulmonary bypass with myocardial protection by cardioplegia and hypothermia of 28 ℃ to 32 ℃. Distal anastomoses were undertaken first if coronary artery bypass grafting (CABG) was carried out, before ventriculotomy. After adequate debridement, pledgetted sutures were inserted around the VSD with 3/0 or 4/0 Prolene, and Dacron or Teflon patches were used for VSD closure. Sandwich closure of the ventriculotomy was carried out, including the free edge of the VSD patch and 2 Teflon strips for reinforcement on both sides of the incisions, using 3/0 or 2/0 Prolene sutures. Proximal vein graft anastomoses were completed afterwards. Routine de-airing, rewarming, decannulation, and primary sternal closure were accomplished. Seven consultant surgeons performed the operations. Mean aortic crossclamp time was 87 ± 35 min, and mean bypass time was 117 ± 44 min. Concomitant procedures included CABG in 8 (20%) patients (1 vein graft per patient) and tricuspid valve repairs in 2.
Early surgical mortality was defined as 30-day mortality, and long-term survival and freedom from cardiac events was defined as no admission for angina or myocardial infarction, congestive heart failure, or percutaneous closure of residual septal defects. Incidences are presented as number and percentage, and quantitative data are presented as mean ± SD or median and range. Logrank tests were used for statistical comparisons. In addition, individual analyses of preoperative variables and their associations with early or later deaths were performed, and their odds ratios (OR) are quoted. In situations where the contingency table contained frequencies less than 5, Fisher’s exact test was employed instead of the chi-squared test. Univariate analyses of long-term survival and event-free survival were carried out using the Kaplan-Meier method (SPSS for Windows; SPSS, Inc., Chicago, IL, USA). Values of p < 0.05 were considered statistically significant.
Results
Predictors of early (30-day) mortality after post-infarction ventricular septal defect repair.
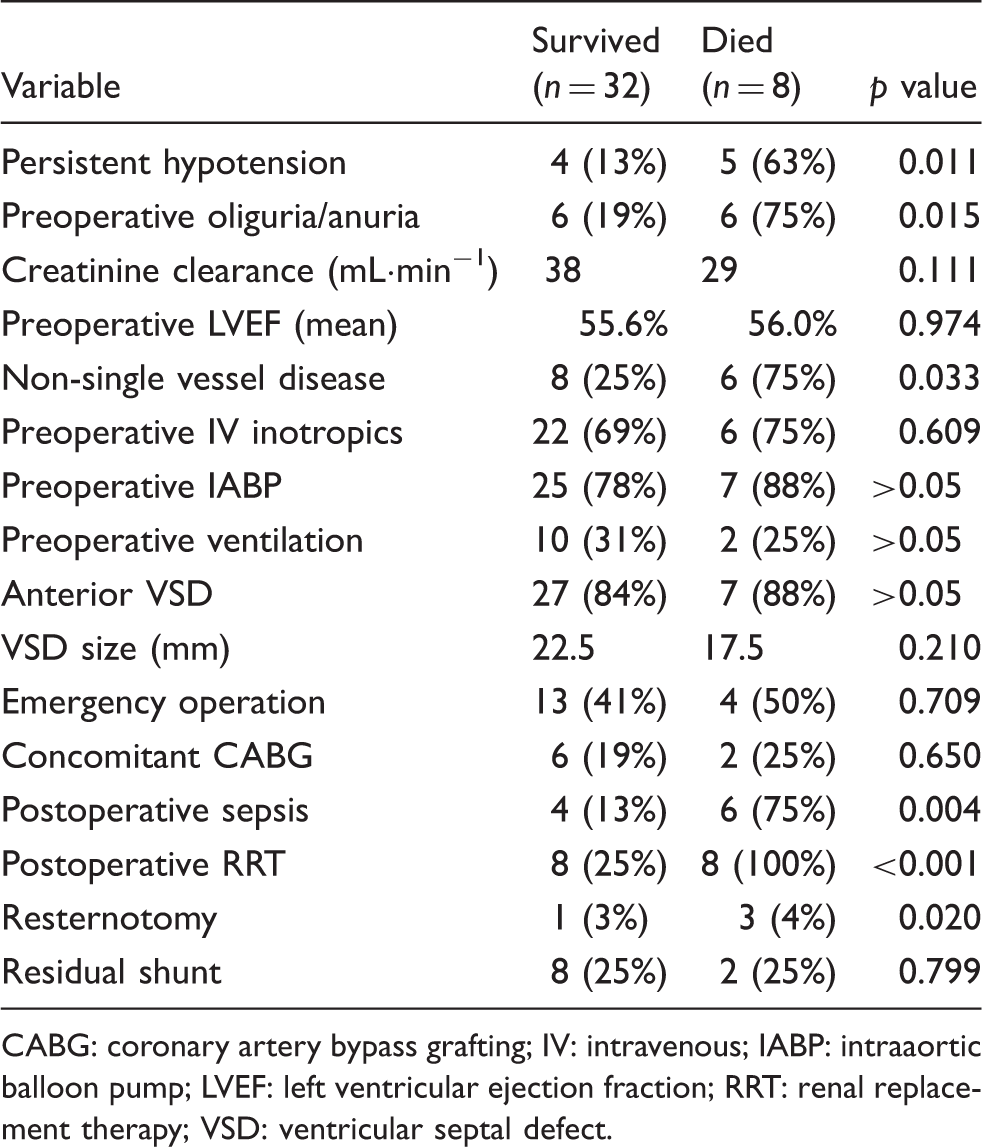
CABG: coronary artery bypass grafting; IV: intravenous; IABP: intraaortic balloon pump; LVEF: left ventricular ejection fraction; RRT: renal replacement therapy; VSD: ventricular septal defect.
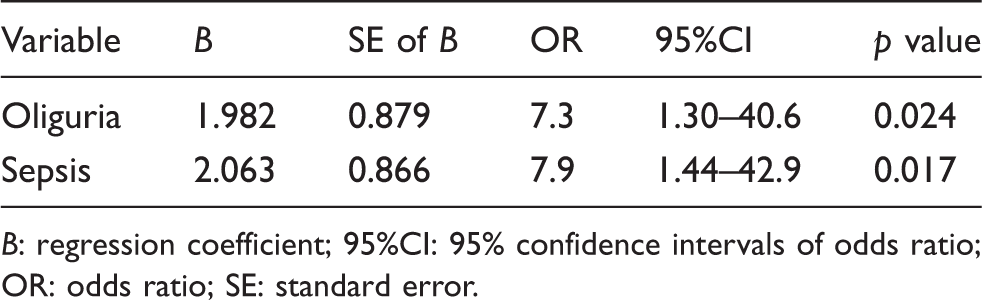
Three preoperative and 3 postoperative factors associating with early mortality, with p values less than 0.05 in univariate analyses were entered into multivariate analyses. Multivariate Cox regression analyses showed that preoperative oliguria (OR 7.3, p = 0.044) and postoperative sepsis (OR 7.9, p = 0.049) were the only variables that correlated with early postoperative death (Table 3). Performing CABG in addition to VSD repair was not associated with an increase in early mortality or complications (p = 0.65). However, we were not able to demonstrate an improvement in overall survival by performing concomitant CABG in our patients (p = 0.334; Figure 1). Furthermore, a subgroup analysis of patients with multivessel disease (n = 14) showed no significant difference in survival between the CABG group (n = 7) and the non-CABG group (n = 7).
Difference in event-free survival in patients with or without coronary artery bypass grafting (CABG). Independent predictors of 30-day mortality by Cox regression multivariate analysis. B: regression coefficient; 95%CI: 95% confidence intervals of odds ratio; OR: odds ratio; SE: standard error.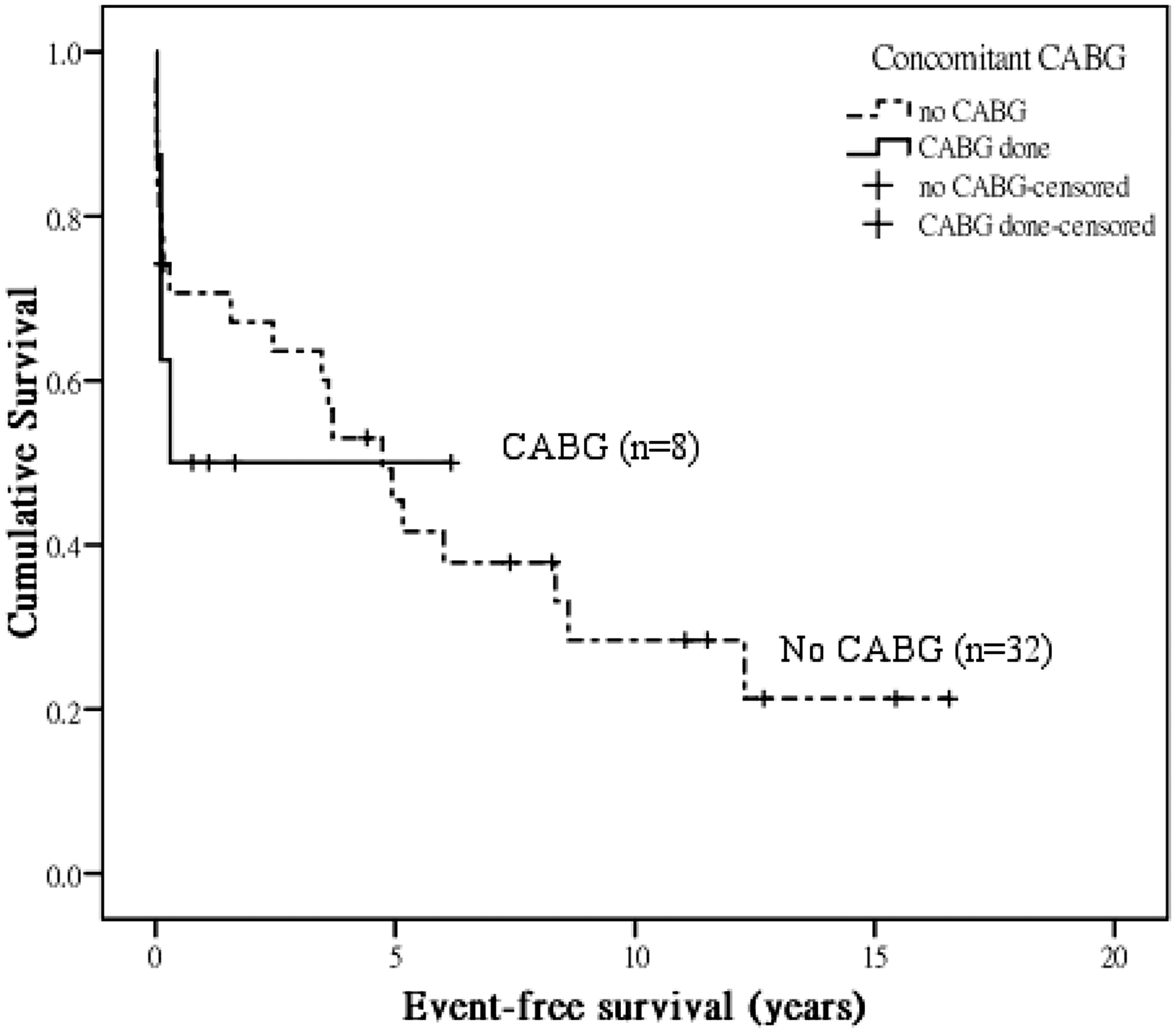
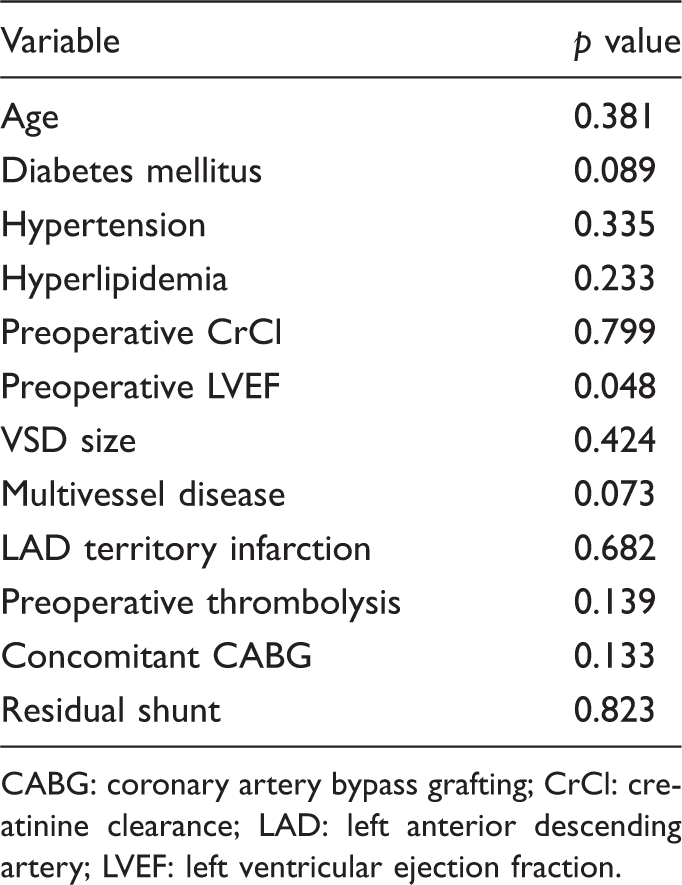
All patients had long-term follow-up with a cardiologist and/or cardiac surgeons, with one exception only. Mean follow-up duration was 5.2 ± 5.3 years. Among the late survivors, age, sex, pre-morbid cardiovascular risk factors, or having CABG during the initial operation were not significant predictors of long-term survival. The preoperative LVEF was the only significant determinant of long-term survival in this study (p = 0.048; Table 4). The size of the repaired VSD and the presence of a residual shunt did not predict long-term survival. Overall survival at 1, 5, and 10 years was 68%, 55%, and 42%, respectively. Event-free survival from subsequent angina, myocardial infarction, congestive heart failure, or percutaneous interventions at 1, 5, and 10 years was 66%, 43%, and 25%, respectively (Figure 2).
Kaplan-Meier survival curves for total survival and event-free survival. Perioperative predictors of long-term survival. CABG: coronary artery bypass grafting; CrCl: creatinine clearance; LAD: left anterior descending artery; LVEF: left ventricular ejection fraction.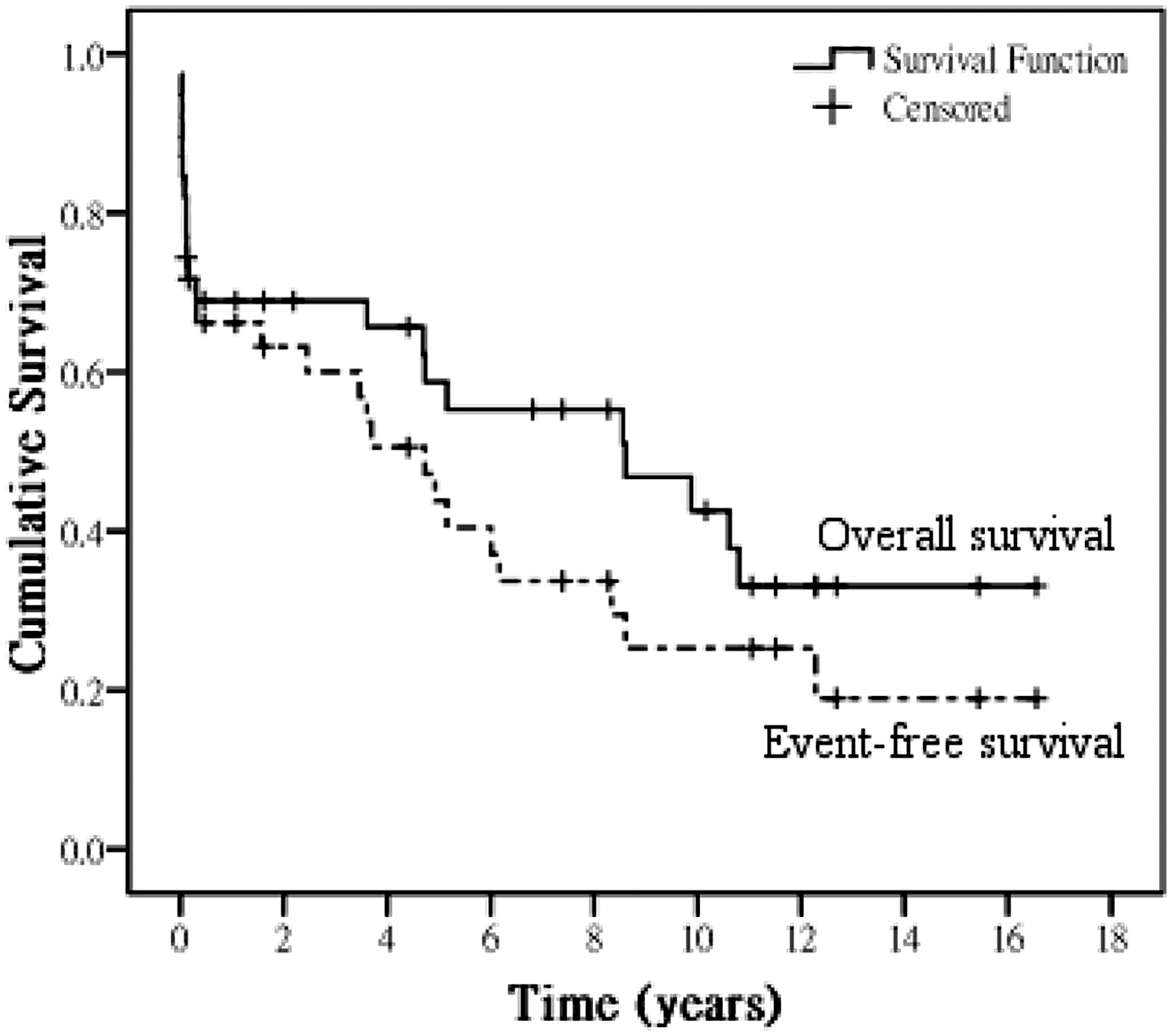
Discussion
It is a common notation that post-infarction VSD occurs in patients in their 60 s who suffer their first episode of anterior myocardial infarction. 2 It has been estimated to occur in 1%–2% of all myocardial infarctions. Since the introduction of reperfusion strategies, there has been a reduction of the incidence to 0.2% on thrombolytic treatment. 1 A similar trend has also been demonstrated in patients with primary angioplasty. 13 The occurrence of an acute left-to-right shunt in a heart with recent infarction carries extremely high mortality. In the GUSTO-I study, the 30-day mortality of medically treated patients was 94% compared to 47% in the surgical repair group. The success of the David and Armstrong 14 infarct exclusion technique further reduced the operative mortality of this high-risk operation. Most studies within this decade across the world have reported 23% to 38% early mortality (30-day or hospital mortality).6–8,15,16 We accept emergency cardiac surgical referrals from the whole territory, and overall 30-day mortality in our current series was 20%. However, no attempt at a direct comparison was made because the differences in outcomes among centers and different time periods probably reflect the differences in referral patterns and recruitment for surgical intervention.
We observed a similar age group and a slight female preponderance among our patients, as in the GUSTO-I study. Although advanced age, female sex, and anterior infarction have been shown to relate to the occurrence of post-infarction VSD; age and female sex were not found to be predictors of worse survival. Approximately 90% of our VSD were related to anterior infarction due to left anterior descending artery occlusion, hence no difference between anterior and posterior infarctions could be detected in this study. Only one patient had prior history of myocardial infarction, and 63% had single-vessel disease only. These findings confirm reports that post-infarction VSD tends to occur in hearts with less well-formed collateral vessels.17,18
Preoperative shock and organ hypoperfusion (reflected in preoperative oliguria or anuria) strongly predicted 30-day mortality (OR 9.6 and 9.2, respectively). We used a strict definition of shock: hypotension was defined as systolic blood pressure ≤90 mm Hg, and oliguria as less than 0.5 mL·kg−1·h−1 of urine production. But if the patient survived the early period, preoperative shock and oliguria did not influence long-term survival, suggesting that these hemodynamic factors had no persistent biological effect beyond the perioperative state. Several studies showed similar findings or shared the same conclusion.9,16 Most of these patients were given intravenous inotropics and frusemide. We advocate placement of an IABP after the diagnosis of VSD. An IABP reduces the afterload of the failing heart and improves the forward systemic cardiac output and coronary flow. Theoretically, the shunt across the VSD and thereby right heart overload would also be reduced. Although we were not able to demonstrate a survival benefit by its use, we believe that IABP support provided patients adequate stabilization for operation arrangements or transfer to our institution. A quarter of our patients were intubated preoperatively due to our relatively liberal use of mechanical ventilation, mainly for management of congested lung fields, and this did not necessarily represent worse hemodynamics.
The role of concomitant CABG remains controversial. Intuitively, one would surmise that CABG would be necessary in selected patients to reduce future ischemic events. All except one CABG operations were performed on a noninfarct-related artery in our patients with 2- or 3-vessel disease. Many studies have reported improved early and late outcomes with revascularization, whereas a number of others have shown no benefits.9,15,16,19,20 In our experience, patients who had CABG performed as well as those without CABG, with no added morbidity or mortality. The subgroup analysis of patients with multivessel disease did not show a difference in long-term survival or event-free survival. Our population had a high rate of single-vessel disease (63%), hence it would seem that the majority of our patients would not require extra revascularization. Similar patterns were also noticed in other smaller Asian series.5–8
In our cohort, postoperative renal failure requiring peritoneal dialysis or hemodialysis was the most common complication and it was predictive of 30-day mortality, and this was also statistically related to preoperative renal failure. As in other cardiac surgery, preoperative renal failure predicted increased operative mortality. Postoperative sepsis was another complication associated with increased 30-day mortality. Causes of the sepsis included pneumonia, wound infection and mediastinitis, and persistent high fever without any positive bacterial culture. In our multivariate analysis, both preoperative oliguria or anuria and postoperative sepsis were associated with a nearly 8-fold increase in 30-day mortality. Nonetheless, sepsis was not related to long-term survival. This would suggest that if a patient has been treated and survived the early postoperative period, sepsis had no persistent effect on the long-term prognosis. One-quarter of our patients had Doppler evidence of a residual shunt. Our high proportion of residual shunts could be attributed to the very careful scanning during the early postoperative period by our cardiologists. However, only 2 patients required reoperations. Furthermore, we observed a trend for more residual shunts after emergency operations rather than urgent or semiurgent operations. We could postulate that when the sicker patient (who may have had a more extensive infarct and hence intractable heart failure) requires an emergency operation, the surgeons would need to operate on freshly infarcted tissue that was more fragile and prone to cut-through by sutures, a reflection of the fact that chronic defects are easier to repair. 2 Nonetheless, there was no significant difference in long-term survival associated with the presence of a residual shunt, suggesting that many were indeed clinically insignificant findings.
Although the patients who died within 30 days and those who survived had similar LVEF (55% vs. 56%, p = 0.97), those with better LVEF tended to have better long-term survival. It seems that while early survival is more dependent on the severity of illness preoperatively and the immediate complications, the long-term survival is relatively independent of these factors and more related to the overall cardiac fitness, using LVEF as a surrogate marker. A major shortcoming of this study is the lack of uniform follow-up measurements of the postoperative LVEF, due to a difference in practice among various cardiology centers in the territory. Hence, we were unable to demonstrate any potential improvement in cardiac function after surgery. Secondly, apart from IABP, we did not have any experience with the latest developments in mechanical support such as extracorporeal membrane oxygenators or ventricular-assist devices in this condition. Last but not least, it would be beyond the scope of this retrospective study to draw any conclusion regarding the best timing for surgery, due to the relatively small number of patients in each subgroup (emergency, urgent, or semiurgent operations).
From our experience, we concluded that preoperative evidence of renal hypoperfusion and postoperative septic complications give rise to significantly higher surgical mortality. If the patient is unstable before surgery and requires addition mechanical support, we would still recommend early insertion of an IABP, and coronary angiography may be carried out if feasible, to allow selected patients to undergo concomitant CABG during VSD repair.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.
Presented at the 20th Annual Scientific Congress, Hong Kong College of Cardiology, Hong Kong, May 4, 2012.