
Abstract
A 26-year-old man presented with lower extremity edema and abdominal protrusion associated with dyspnea for 5 years, which had increased 7 months earlier. Echocardiography demonstrated a huge right atrium of 19.5 × 15.2 cm with a thick smoke pattern and severe tricuspid regurgitation. Magnetic resonance imaging confirmed intact pericardium. A pulmonary perfusion scan demonstrated multiple perfusion defects, suggesting recurrent small pulmonary emboli. Idiopathic enlargement of the right atrium was diagnosed. The patient declined surgery.
Case report
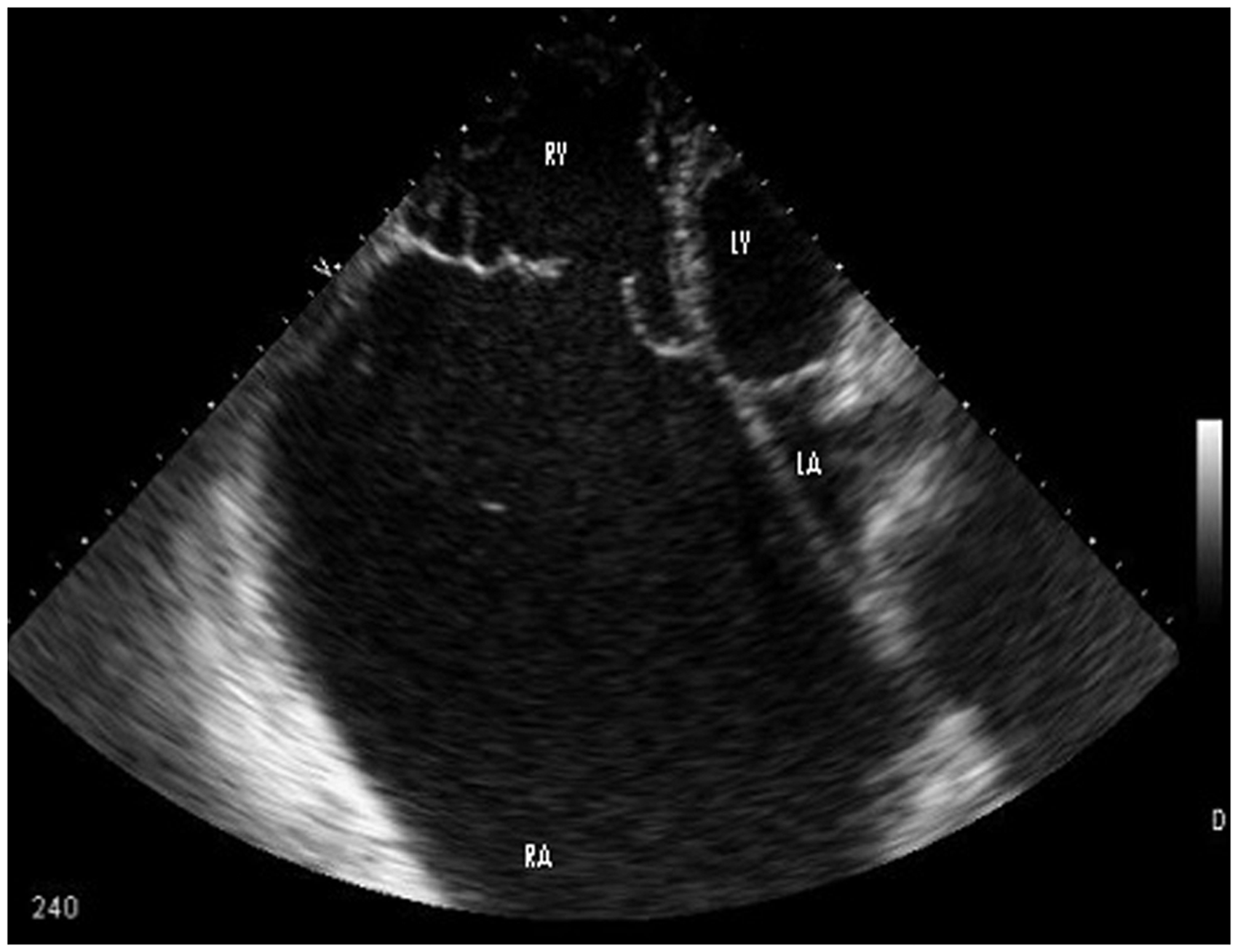
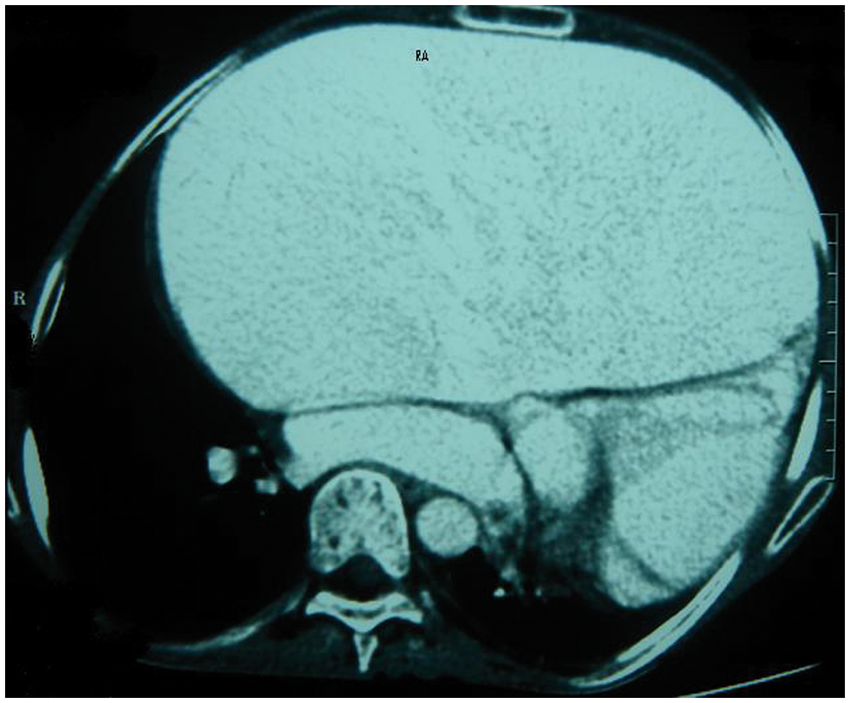
A 26-year-old man presented to emergency room with lower extremity edema and abdominal protrusion associated with dyspnea of 5-years duration, which had increased 7 months prior to admission. Echocardiography 2 years earlier, suggested atrial enlargement with mild to moderate tricuspid insufficiency and pulmonary arterial pressure of 35 mm·Hg. On admission, he was afebrile with blood pressure of 95/65 mm·Hg, a pulse rate of 50 beats·min−1, and a respiratory rate of 25 breaths·min−1. Cardiac examination showed increased heart size on percussion and a grade III/VI systolic murmur at the 5th intercostal space in the midaxillary line. The point of maximal impulse of the left ventricle was displaced from its original site in the midclavicular line at the 5th intercostal space to the left inferior scapular angle. Pulmonary auscultation revealed decreased breathing sounds in the left lower 2/3 and right lower 1/3, with no rales or wheeze. Electrocardiography showed a regular junctional escape rhythm with a rate of approximately 50 beats·min−1 associated with low voltage QRS because of posterior rotation of the left heart. Chest radiography in a standing position and with anteroposterior projection indicated cardiomegaly (Figure 1). Echocardiography demonstrated a huge right atrium of 19.5 × 15.2 cm with a thick smoke pattern and severe tricuspid regurgitation. The pulmonary arterial pressure was 65–70 mm·Hg, associated with right ventricular hypertrophy and a normal left heart with regard to size and function (Figure 2). A spiral computed tomographic scan of the chest showed a dilated right atrium with a normal but compressed lung field (Figure 3). Magnetic resonance imaging confirmed an intact pericardium, which excluded partial absence of the pericardium as a possible cause of atrial dilatation. A pulmonary perfusion scan demonstrated multiple perfusion defects, suggesting recurrent small pulmonary emboli. The patient declined any type of operation and was discharged with oral anticoagulants in junctional rhythm and New York Heart Association functional class II. Unfortunately, he did not consent to pacemaker implantation, and no calcium channel blocker was given because of junctional rhythm.
Chest radiograph showing massive cardiomegaly with right atrial enlargement. Two-dimensional transthoracic echocardiography in the apical position with 4-chamber view: a huge right atrium can be seen, associated with right ventricular hypertrophy and moderate right ventricular dilatation. Spiral computed tomography of the chest, with intervenous contrast, showing the dilated right atrium.
Discussion
This patient presented with a huge right atrium associated with junctional rhythm and pulmonary hypertension. This situation can be due to different etiologies: one cause is absence of pericardium, which was ruled out in this case; the most important etiology is recurrent pulmonary embolism with resultant pulmonary hypertension. In view of the fact that right atrial dilatation was present 2 years earlier in this patient, and severe tricuspid regurgitation, right ventricular hypertrophy, and pulmonary hypertension was established during these 2 years, right atrial dilatation was the primary event, with recurrent small pulmonary emboli because of blood stagnation in the right atrium as the main cause of pulmonary hypertension. Therefore, in this case, a diagnosis of idiopathic enlargement of the right atrium (IERA) was made.
IERA is a rare cardiac anomaly of unknown etiology. 1 It is defined as an increase in the right atrial long axis indexed to body surface area (men > 2.6 cm·m−2, women > 2.8 cm·m−2) in the absence of other cardiac abnormalities. In this case, this index was 12.18 cm·m−2, which greatly exceeds the threshold for diagnosis. Severe IERA is defined arbitrarily as an index ≥4 cm·m−2, which categorizes this patient as having severe IERA. This condition is not usually accompanied by primary tricuspid valve disease; valvular insufficiency is the result of IERA.2,3 The most important etiologies that should be excluded are absence of pericardium which can easily be seen in cardiac magnetic resonance imaging, and recurrent small pulmonary emboli which can be ruled out by comparing the current imaging and pressure study with a previous one. In our case, the patient had undergone echocardiography 2 years earlier, with the same huge right atrium but only mild pulmonary hypertension, which proved that IERA was the cause of his pulmonary hypertension.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.