
Abstract
Aim
To evaluate the efficacy of early video-assisted thoracoscopic debridement in patients with the fibropurulent phase of parapneumonic empyema.
Patients and methods
40 patients with parapneumonic empyema resistant to 2 weeks of antibiotic therapy, were randomly divided into 2 groups. In group 1 (20 patients), antibiotic therapy and irrigation was continued, and in group 2 (20 patients), video-assisted thoracoscopic debridement was performed. The 2 groups were compared in terms of therapeutic results.
Results
The male/female ratio was 29/11. Group 1 included 16 men and 4 women with a mean age of 54 years, and mean hospital stay was 41 days. Group 2 consisted of 14 men and 6 women with a mean age of 51 years, and mean hospital stay was 23 days.
Considering the therapeutic results, 12 patients in group 1 were cured by antibiotic therapy and irrigation, whereas 8 required decortication and pleurectomy with thoracotomy. In group 2, 18 patients were cured by video-assisted thoracoscopic debridement, and 2 underwent thoracotomy and decortication due to intraoperative bleeding. A significant difference in therapeutic results was noted between the groups (p = 0.028).
Conclusion
Video-assisted thoracoscopic debridement provides a high success rate and less invasive treatment for the early stages of empyema.
Introduction
Considering the high morbidity and mortality rates due to parapneumonic effusion (PPE), and despite aggressive usage of systemic broad-spectrum antibiotics in the early stages of empyema, PPE is still a challenging issue in developing countries.1,2 Parapneumonic effusion occurs in 20%–40% of patients admitted with pneumonia. PPE is defined as accumulation of exudative fluid in the pleural space. Progression to empyema relates directly to delayed treatment with antibiotic therapy or drainage. 3 The different stages of thoracic empyema are: stage 1: the exudative phase, identified by high lactate dehydrogenase and protein levels, and low pH; stage 2: the fibropurulent phase, recognized by loculations established in the empyema space; and stage 3: the chronic and organized phase, recognized by thick peels on the visceral pleural surface. Adequate antibiotic therapy with chest tube drainage usually cures stage 1 empyema. However, in the case of insufficient treatment, it progresses to stage 2 or 3.1,3 Continuing antibiotic therapy and irrigation, streptokinase injection, and debridement of multiloculated collections by means of video-assisted thoracoscopic surgery (VATS) most often cures the fibropurulent empyema of stage 2.1,4 In the case of inappropriate treatment of empyema and presentation of chronic thoracic empyema, thoracotomy with decortication and parietal pleurectomy is advocated for more advanced levels, and this was the accepted procedure in several reports.5,6 In fact, the aim is to prevent progression of stage 2 to stage 3 and subsequently open thoracotomy, which leads to a longer period of treatment.1,4,5 The aim of this study was to evaluate the effects of early debridement by thoracoscopy in patients with the fibropurulent phase of PPE. We also analyzed the factors affecting the success or failure of the procedure.
Patients and methods
Characteristics of patients with parapneumonic empyema treated with and without VATS.
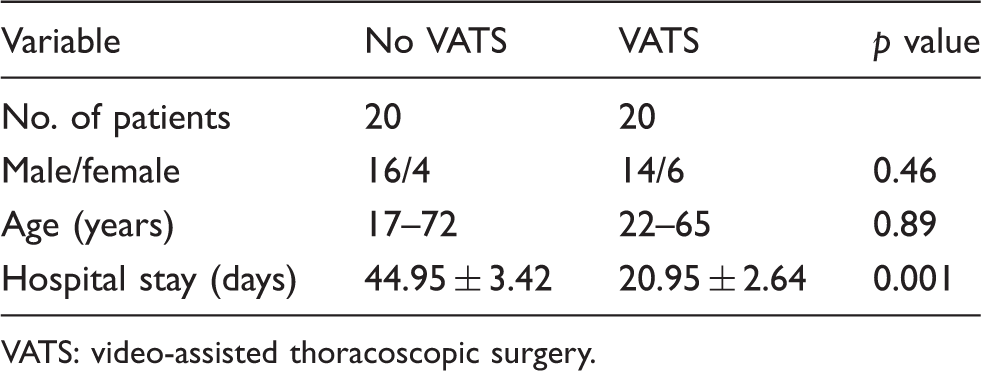
VATS: video-assisted thoracoscopic surgery.
Irrigation was performed by inserting a Nelaton catheter in the chest tube and irrigating the pleural cavity with 1000 mL of normal saline solution for 24 h continuously. All patients selected for VATS debridement underwent general anesthesia with double-lumen endotracheal intubation, and were placed in the lateral position. A thoracoscopic port was placed in the 8th intercostal space on the anterior superior iliac spine line, and 2 ports were placed in the 5th intercostal space on the middle and anterior axillary line. During surgery, all loculations were removed, and the empyema cavity was irrigated with saline. A chest tube was inserted into the pleural cavity through the port wounds. All patients were extubated and treated with antibiotics afterwards. The patients were followed-up for one year.
Data of age, sex, length of hospital stay, morbidity, and hospital mortality were collected. Treatment results were evaluated in both groups. Success was defined as no purulent discharge from the chest tube, improvement in symptoms (2 clinical criteria), and removal of multiloculated collection (radiologic criterion).
For statistical analysis, the chi-square test was used. Incessant variables were analyzed using the 2-tailed Student’s t test. Data are expressed as mean ± standard deviation. Results were considered significant if p < 0.05.
Results
In group 1, 12 (60%) cases responded to the treatment (according to the definition of success), and in 8 (40%) cases, irrigation and systemic antibiotic therapy failed, for which open decortication and pleurectomy with posterolateral thoracotomy was performed. In group 2, 18 (90%) cases were successfully cured, and in the other 2 patients, the VATS procedure failed and was converted to open surgery (decortication and pleurectomy) due to intraoperative bleeding. A significant difference was noted in the therapeutic success rate between groups (p = 0.028). Hospital stay (from the day that empyema was diagnosed) in the irrigation group was 44.95 ± 11 days, and 20.95 ± 9 days in the VATS group. There was a significant difference between these 2 groups (p < 0.05). Postoperative complications occurred in 2 patients. One had postoperative atelectasis (in group 1), and the other (in group 2) had a wound infection. They were cured by medical treatment. There was no significant difference in postoperative complications between the 2 groups, and no hospital death was reported.
Discussion
PPE is one of the most common problems in thoracic surgery, which increases morbidity and mortality in patients with pneumonia. The management and treatment of empyema differs according to the surgeon’s preference.6,7 Selecting the appropriate treatment depends on whether a complicated or uncomplicated effusion exists.7,8 Early drainage by means of a chest tube or limited thoracotomy is the traditional way to treat complicated effusion or empyema. When the lung does not expand well despite aggressive antibiotic therapy or chest tube drainage, surgical intervention is needed.1,9 The exudative phase of empyema has a low cellular content and acceptable fluidity, therefore, thoracentesis or tube drainage is usually sufficient for lung reexpansion.
However, patients with PPE are mostly admitted when they are in the fibropurulent phase with a denser pleural effusion. 10 Drainage alone is insufficient in this phase. Other recommended therapies include applying streptokinase, irrigation, or early VATS.1,6 A study by Luh and colleagues 3 in 2008 demonstrated that there is still controversy between applying VATS or fibrinolytic therapy for patients with PPE, especially in the fibrinopurulent phase (stage 2). They recommended that more studies should be carried out to obtain a definitive conclusion. In a trial by Yamaguchi and colleagues, 1 applying VATS in the fibropurulent phase was recommended as the optimum procedure owing to appropriate therapeutic results and less invasiveness, which avoided conversion to the chronic phase and subsequent complications. Bilgin and colleagues 10 revealed that using VATS in the fibropurulent phase allows early recovery and prevents further complications. Kim and colleagues 9 found that administrating VATS with endo-shave is a simple and effective procedure for treatment of the fibropurulent phase. In study by Luh and colleagues 7 on 234 patients with parapneumonic empyema, early VATS resulted in good outcomes. Potaris and colleagues 11 highlighted that VATS debridement is a safe and effective technique with less morbidity and no mortality in the fibropurulent phase of thoracic empyema. Various studies have implied that thoracotomy and open surgery is an acceptable treatment in patients with stage 3 empyema, due to increased technical failure of VATS.1,5,11 However, the results of VATS in this phase have also been reported. Studies comparing VATS to open surgery in patients with chronic empyema (stage 3) found less postoperative chest drainage, shorter hospital stay, less pain after the operation, and earlier mobilization after VATS.5,6 Chan and colleagues 12 noted that optimal results can be achieved regardless of the stage of empyema, and they strongly advised open thoracotomy, although VATS could be performed by experienced hands.
Several studies have evaluated VATS as a therapeutic modality in children with empyema. In 2008, a large retrospective study assessed the efficacy of VATS in 114 children with empyema; 91% had full resolution of their symptoms. This study demonstrated that excellent results can be achieved in children with empyema if performed with expertise. 4 Yamaguchi and colleagues 1 assessed complications and failures in 151 children with empyema who underwent VATS; 82.6% were treated successfully. In addition to the shorter length of stay, other advantages include full evacuation of empyema fluid, which decreases the need for open surgery and decortication. Bilgin and colleagues 10 recommended VATS as the treatment of choice in well-equipped centers. Waller and Rengarajan 5 studied 48 patients with multiloculated PPE who underwent visceral pleural decortication. They concluded that VATS has many perioperative advantages over open surgery; VATS shortened general anesthesia, postoperative stay, and the immobilization period. Different treatment strategies are recommended in children, and most reports have preferred VATS as the early treatment. A study by Meier and colleagues 2 on complicated forms of empyema showed that early VATS leads to satisfactory results with minimum complications. Chibuk and colleagues 13 concluded that the choice of treatment should be based on the surgeon’s experience and preference, and that early VATS brought about favorable results with minimum complications.
We concluded that the treatment of empyema varies according to the different stages. Open surgery (thoracotomy and decortication) is performed in late-stage empyema (organized and chronic), which is associated with more morbidity and longer hospitalization. In addition, effective and safe treatment with minimal invasiveness (VATS, decortication) is advised in the fibropurulent stage of parapneumonic effusion.
Footnotes
Acknowledgement
This paper is the result of a residency thesis by Dr Kamran Adhami Moghadam which was supported by the Deputy of Research, Mashhad University of Medical Sciences. The authors wish to thank the Vice Chancellor for Education and the research committee of the university for their support.
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.