
Abstract

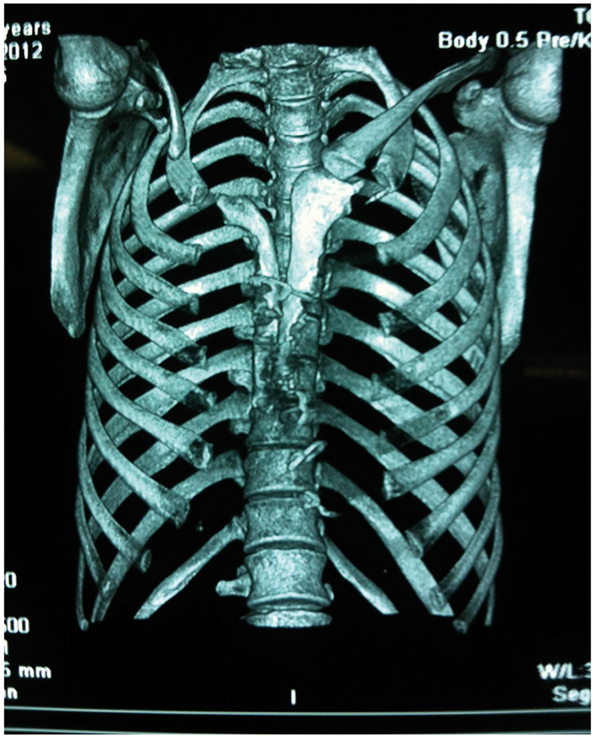
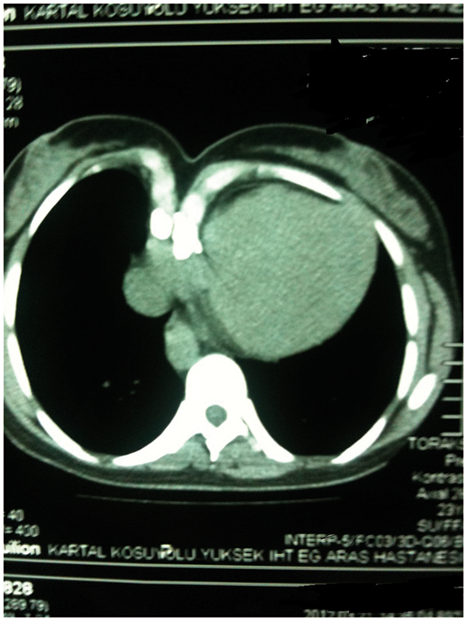
A 29-year-old woman suffered palpitation for one year. Echocardiography showed a discrete subaortic membrane. Absence of the right clavicle and a gap at the side of sternum were found during physical examination. The gap was narrow, and pulsation of the heart could not be palpated subcutaneously. The sternal cleft stayed immobile during the Valsalva maneuver, and paradoxical respiratory movement was not observed. In plain radiography, an asymmetric sternal cleft could be seen (Figure 1). The patient underwent resection of the subaortic membrane. Intraoperatively, the cleft was not located in the midline; it was displaced laterally to the right side. The pieces of the sternal cleft were not equal in size. The manubrium at the right side of the sternum was rudimentary. At the conclusion of the surgical procedure, the lower two-thirds of the sternal parts were approximated via stainless steel wires. Due to the rigidness and asymmetry of the superior parts, the upper one-third of sternum was left apart, as before. Computed tomography was performed after 10 months (Figure 2). The small-sized and asymmetrical clefts can be followed up without any surgical restoration if the patient has no complaints and the mediastinal structures are well protected by the existing bone structures (Figure 3).
Preoperative radiograph showing the sternal cleft and right clavicular agenesia. Postoperative 3-dimensional reconstructed computed tomographic scan. Cross-section of computed tomography scan showing the defect.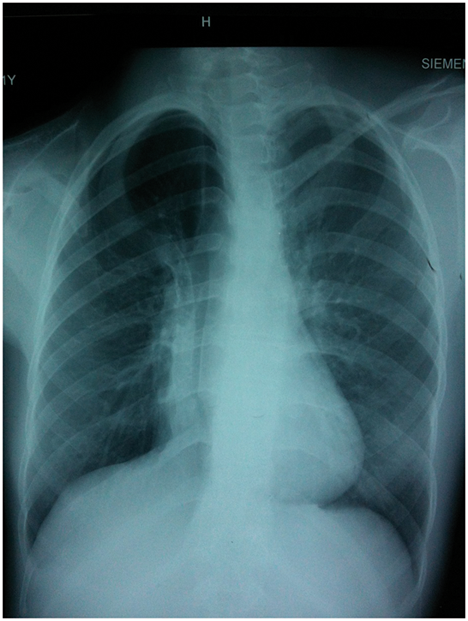
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.