
Abstract
The pedicled left internal thoracic artery graft is the mandatory conduit in coronary artery bypass surgery. A grossly emphysematous lung may sometimes present a significant problem for positioning of the pedicled left internal thoracic artery conduit. An inverted pedicled left internal thoracic artery graft (internal thoracic artery transected near its origin, thus supplied by retrograde flow from superior epigastric and musculophrenic arteries) might occasionally be the conduit of choice for those patients.
Keywords
Introduction
The in-situ pedicled left internal thoracic artery (LITA) conduit is generally accepted as the coronary artery bypass conduit of choice because of matchless long-term patency when it is grafted to the left anterior descending (LAD) coronary artery.1 Unfortunately, an emphysematous lung occupying the whole dome of the left pleural cavity and expanding well over the midline may occasionally produce formidable traction on the pedicled LITA graft, thus compromising blood flow or even causing avulsion of the conduit.2 Using the distal in-situ inverted LITA (LITA transected near its origin, thus supplied by retrograde flow from superior epigastric and musculophrenic arteries) as a conduit to bypass the LAD, we were able to completely avoid all complications to which the classically routed in-situ LITA conduit would be exposed in a patient with a grossly emphysematous lung.
Case report
A 66-year-old man was admitted to the hospital with progressive angina. Significant comorbidities included marked emphysematous lung disease. We planned to use pedicled LITA and additional vein grafts for coronary artery bypass, because angiography revealed severe triple-vessel disease including occlusion of the LAD in its middle part. After a median sternotomy, the LITA was harvested as a pedicled graft using diathermy and metallic clips. It was obvious that inflation of the lungs produced enormous left lung herniation through the pleura and across the midline. We concluded that the grossly emphysematous left lung would produce formidable traction on the classically routed in-situ pedicled LITA graft, or even induce its avulsion from the distal anastomosis. Therefore, we decided to use a distal in-situ inverted LITA conduit to revascularize the LAD. After full heparinization (4 mg·kg−1), the LITA was transected near its origin and reverse blood flow of 70 mL·min−1 was measured. Although the inverted LITA conduit maintained its natural course, the LITA-LAD anastomosis was constructed in the opposite direction compared to the classic one (Figure 1). Vein grafts anastomoses to the right and circumflex coronary arteries were performed before the LITA-LAD anastomosis. The distal LITA pedicle was anchored to the epicardial tissue with stay sutures, to avoid tension or kinking of the conduit or anastomosis. The aortic crossclamp time was 33 min. The heart returned spontaneously to sinus rhythm, and the patient was weaned easily from cardiopulmonary bypass. Inflation of the grossly emphysematous lung did not jeopardize conduit positioning (Figure 1). The patient was discharged on the 10th postoperative day. One month later, 64-slice multidetector row computed tomography confirmed the perfect patency of the inverted distal in-situ LITA conduit with blood supply from the superior epigastric and musculophrenic arteries (Figure 2). Three months later, the patient was free of angina with a normal stress test result.
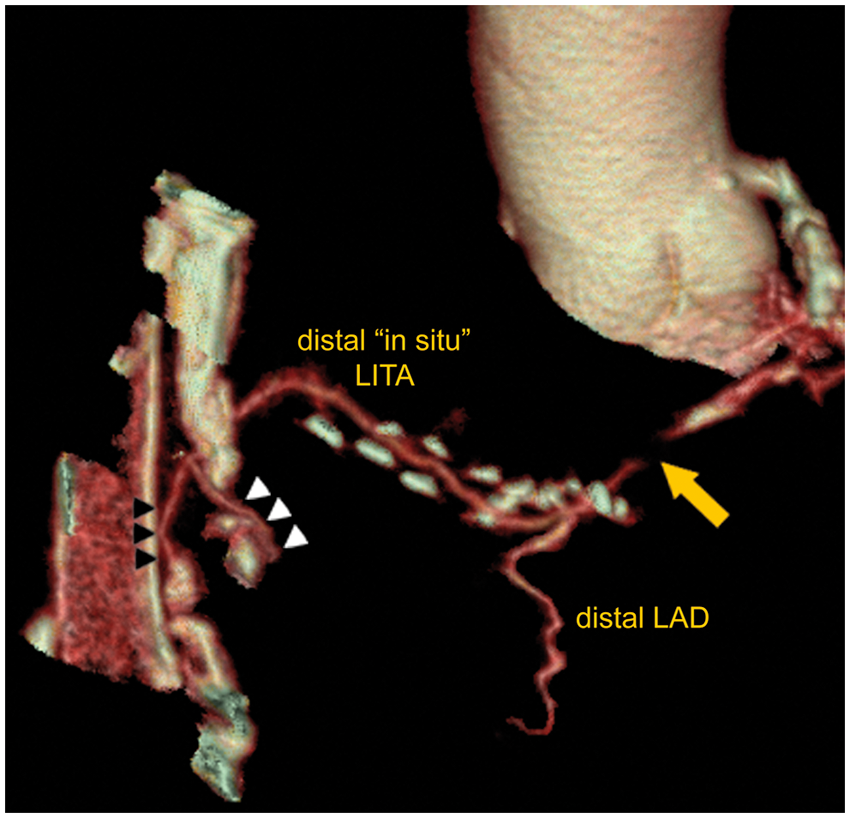
Schematic drawing showing the surgical strategy for grafting of the LAD in a patient with a grossly emphysematous lung (GEL), using an inverted distal in-situ LITA conduit (black arrow) with retrograde blood supply from the superior epigastric (SEA) and musculophrenic (MPHA) arteries. The LITA-LAD anastomosis is constructed in the opposite direction compared to the classic one (dotted black arrow). Black arrowheads: coronary artery lesions. Three-dimensional volume-rendered image with multisegment reconstruction depicts the patent superior epigastric artery (white arrowheads) and musculophrenic artery (black arrowheads) with reversed blood flow that supplies the distal in-situ LITA remnant and subsequently the LAD. Yellow arrow: the site of the proximal LAD occlusion.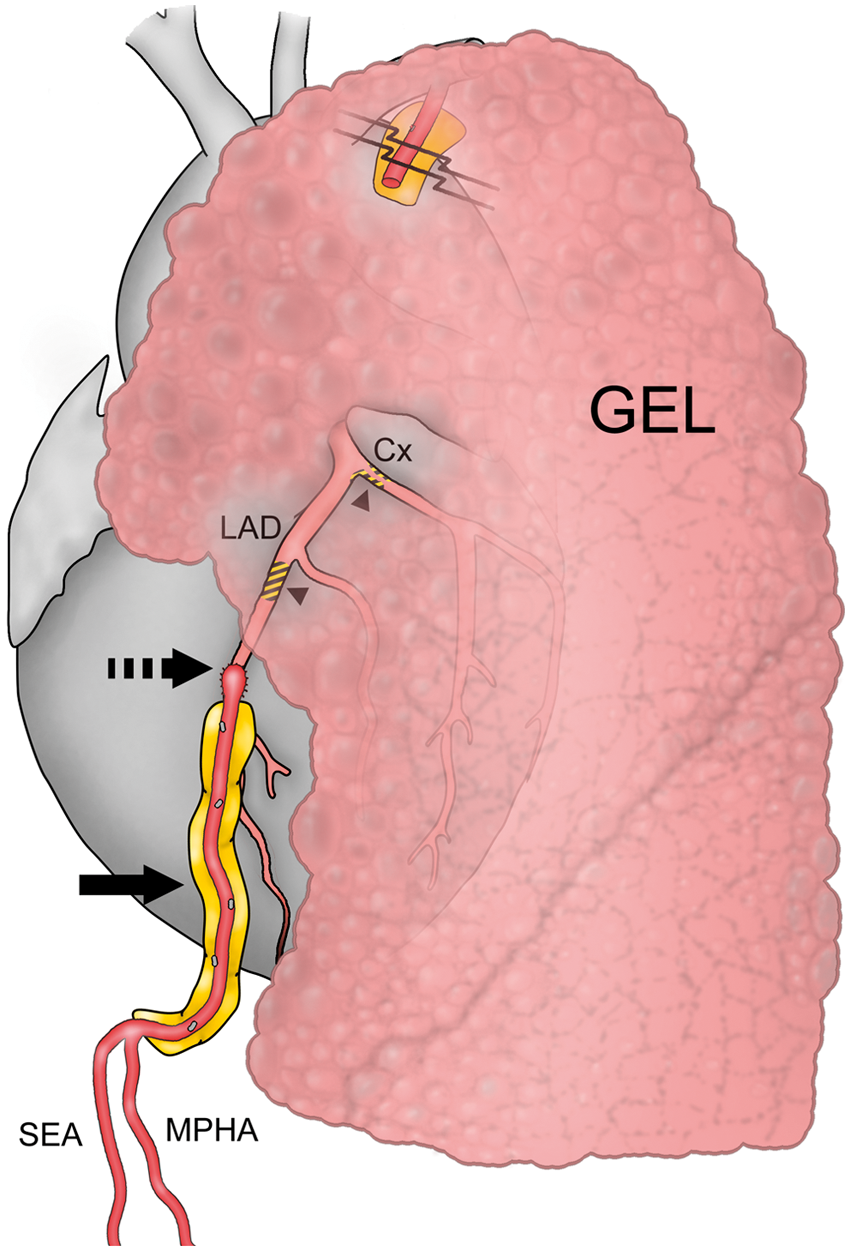
Discussion
The pedicled LITA graft is the mandatory conduit in coronary artery bypass surgery, with its superiority being a direct result of its high resistance to atherosclerosis. 1 However, an emphysematous lung occupying the entire dome of the left pleural cavity and expanding well over the midline can sometimes present a surgical challenge in positioning of the LITA conduit. The basic problem is traction of the most proximal part of the LITA graft, due to pressure on the conduit from the apical segment of the emphysematous lung. It can hardly be avoided, even with the use of a pericardial incision-slit, pericardial flap techniques, or a crisscross incision on the fascia over the LITA. 3 Additional traumatization of the emphysematous lung (e.g. creation of a slit in the apical segment of the left lung upper lobe), 4 can sometimes cause a serious problem such as massive air leakage. We speculated that LITA as a free graft would not be able to reach the LAD without using its most distal part (often small in diameter and prone to spasm). 5
Kolesov and Petukhov 6 were the first to use an inverted-reversed LITA conduit, and Kolesov even protected his author’s right (patent no. 388738-13.04.1973) on reversed LITA-LAD anastomosis.
We recently reported excellent early results using the inverted LITA conduit to revascularize the LAD in the carefully selected patients.1,7 Therefore, we believe that the use of the inverted distal in-situ LITA conduit might sometimes be an acceptable option for patients with grossly emphysematous lungs, provided that adequate retrograde blood flow (above 60 mL·min−1) from the superior epigastric and musculophrenic arteries is obtained, and that targeted coronary artery stenosis is severe (high-grade stenosis or occlusion), thus minimizing concurrent flow through the native coronary artery and the possibility of graft failure later on. 8
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.