
Abstract
Hepatocellular carcinoma is fatal and has a marked propensity for vascular invasion. However, tumor thrombi rarely occur in the right atrium. A 72-year-old man was admitted with dyspnea and disturbed consciousness. Abdominal computed tomography and echocardiography showed a huge tumor thrombus in the inferior vena cava and the right atrium. The tumor thrombus was surgically removed to treat the hemodynamic compromise. The patient underwent transcatheter arterial chemoembolization postoperatively and survived for 6 months.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is a fatal malignancy of the liver. Despite the marked propensity of HCC for vascular invasion and extension to the portal or hepatic vein, tumor thrombosis in the right atrium (RA) is rare.1,2 We report a case of RA obstruction due to cardiac extension of HCC.
Case report
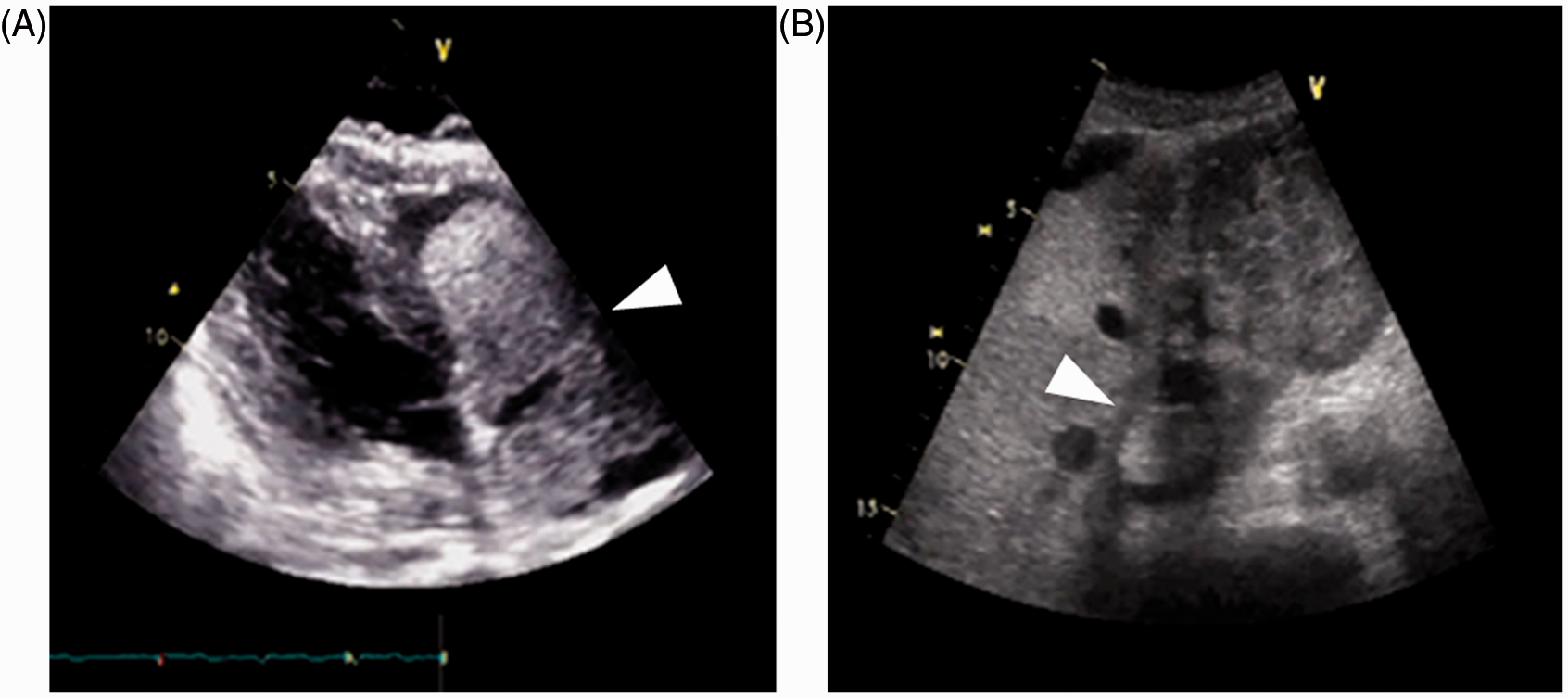
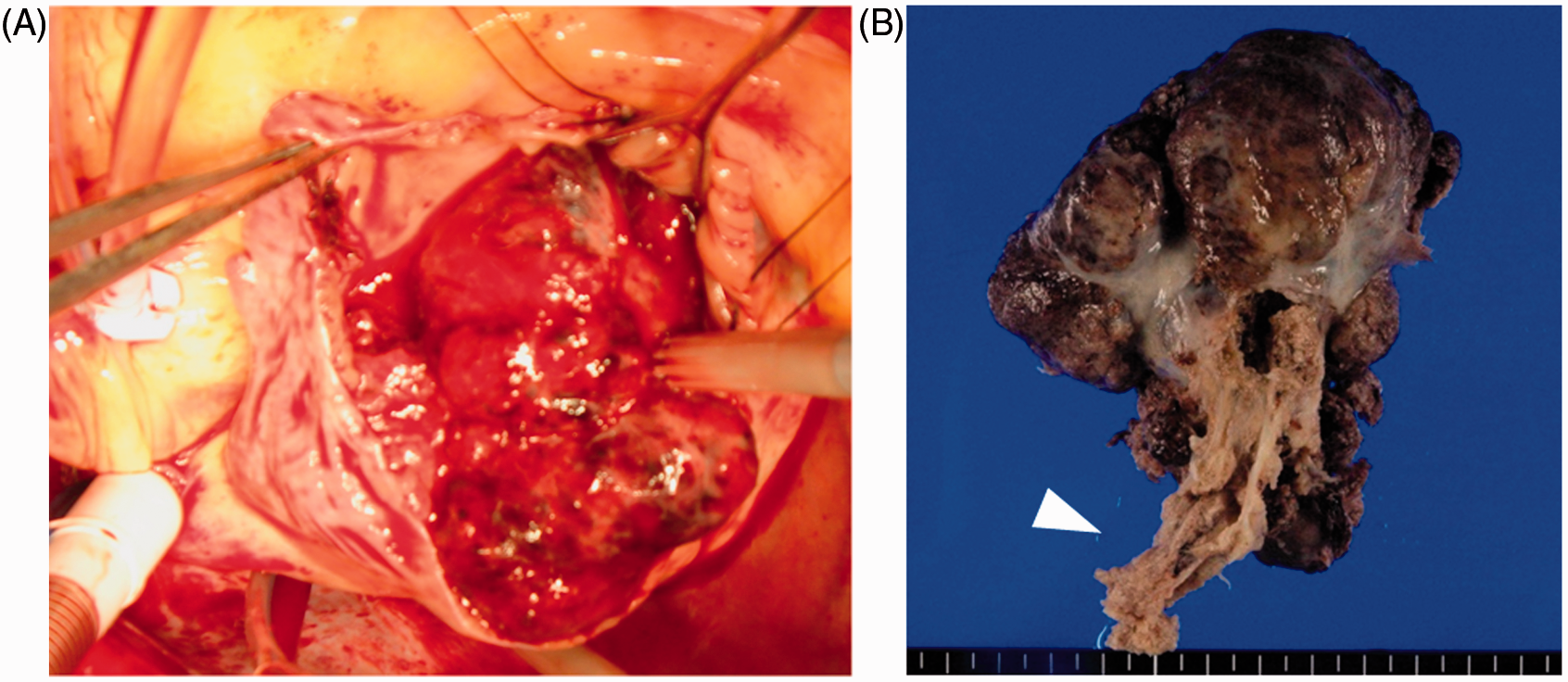
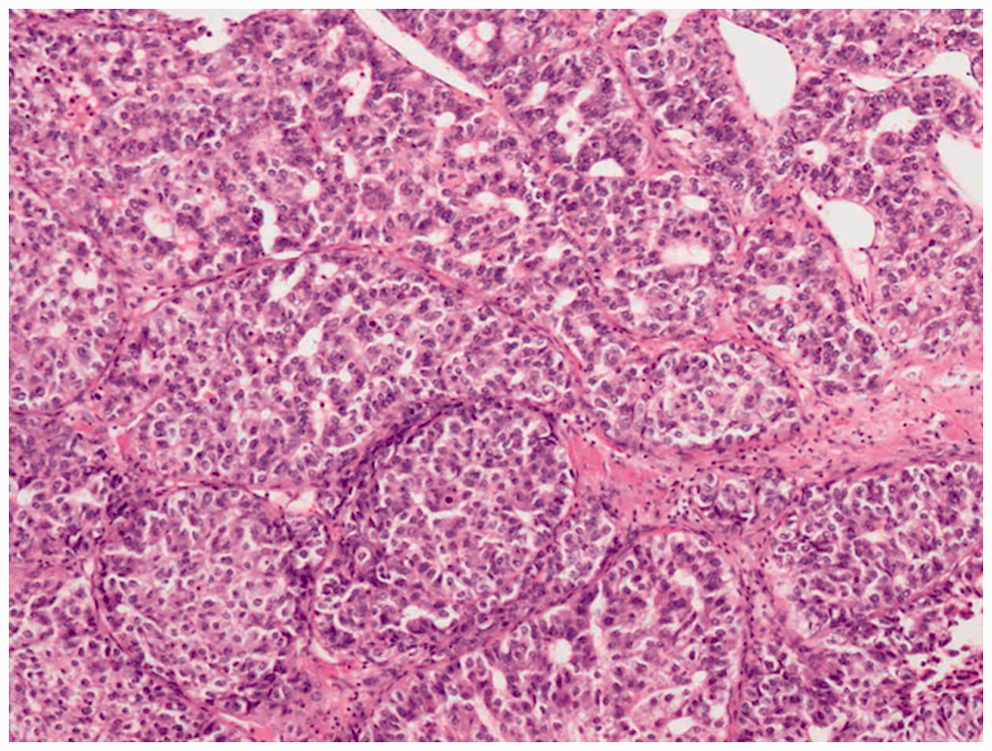
A 72-year-old man with well-controlled Lewy body disease was admitted for treatment of speech disturbance, incontinence, disturbed consciousness, and dyspnea at rest. Physical examination showed generalized cyanosis, cold sweat, tachypnea, abdominal distension, and lower extremity edema. Brain computed tomography demonstrated no new intracranial lesion. Laboratory analyses indicated severe organ damage and a blood coagulation abnormality: glutamic-oxalacetic transaminase 593 IU L−1, glutamic-pyruvic transaminase 397 IU L−1, lactate dehydrogenase 1015 IU L−1, blood urea nitrogen 109 mg dL−1, creatine 2.49 mg dL−1, international normalized ratio 2.03, activated partial thromboplastin time 50.4 s, fibrinogen 292 mg dL−1, D-dimer 10.2 µg mL−1, and fibrin degradation products 15 µg mL−1. Hepatitis B surface antigen and hepatitis C virus antibody were both negative. The alpha-fetoprotein level was as high as 85,492 ng mL−1 (normal range l–10 ng mL−1). Abdominal computed tomography revealed dilatation of the RA and inferior vena cava (IVC; Figure 1A, 1B) and enlargement of the left lobe of the liver with reduced density and obscuration of the vasculature, indicating the presence of a liver tumor (Figure 1C). There was a thrombus-like mass with a high-density area in the left renal vein and IVC (Figure 1D). Echocardiography showed a huge mass occupying the dilated RA (Figure 2A). The mass in the RA was continuous with the mass that occupied the IVC. Abdominal echo showed a well-defined heterogeneous hypoechoic mass in the left lobe of the liver and a solid mass floating in the IVC (Figure 2B). The diagnosis of RA extension of advanced HCC was considered highly probable. Extirpation was undertaken urgently to prevent sudden death from RA obstruction due to cardiac extension of HCC. Cardiopulmonary bypass was established by cannulating the superior vena cava, femoral vein, and ascending aorta. After cardioplegic cardiac arrest, the RA was incised longitudinally. A solid tumor occupied the dilated RA. The tricuspid valve and the atrial wall were free of the tumor (Figure 3A). The tumor extended into the IVC and was removed en bloc (Figure 3B) under intermittent hypothermic circulatory arrest. Pathological examination revealed malignant cells with the pseudo-glandular and trabecular architectural patterns of HCC (Figure 4), confirming RA metastasis from the HCC. The postoperative course was uneventful. Postoperative computed tomography demonstrated that the tumor in the RA and IVC had disappeared (Figure 5). The patient was discharged from our hospital after subsequent transcatheter arterial chemoembolization using miriplatin hydrate for the primary hepatic tumor, and he ultimately died of tumor extension 6 months after the operation.
Abdominal computed tomography scan showing: (A) dilatation of the right atrium. (B) Dilatation of the inferior vena cava in the thorax. (C) Enlargement of the left lobe of the liver with ill-defined vasculature, and marked dilatation of the left lobe of the portal vein, suggesting tumor thrombus. (D) Dilatation of the inferior vena cava and left renal vein with a high-density area that suggested venous stasis and a blood clot. (A) Transthoracic echocardiogram in long-axis view: the right atrium was dilated and occupied by a multilocular tumor (arrow). (B) Transverse scan of the liver, showing a well-defined heterogeneous low-echoic mass in the left lobe of the liver and a solid mass floating in the inferior vena cava. (A) Right atrial tumor with clot. (B) The tumor extended to the inferior vena cava (arrow). Histologic photomicrograph: the tumor cells were arranged in pseudo-glandular and trabecular architectural patterns of hepatocellular carcinoma. Hematoxylin-eosin stain, original magnification ×40. Computed tomography on postoperative day 3. The thrombus in the inferior vena cava was removed completely.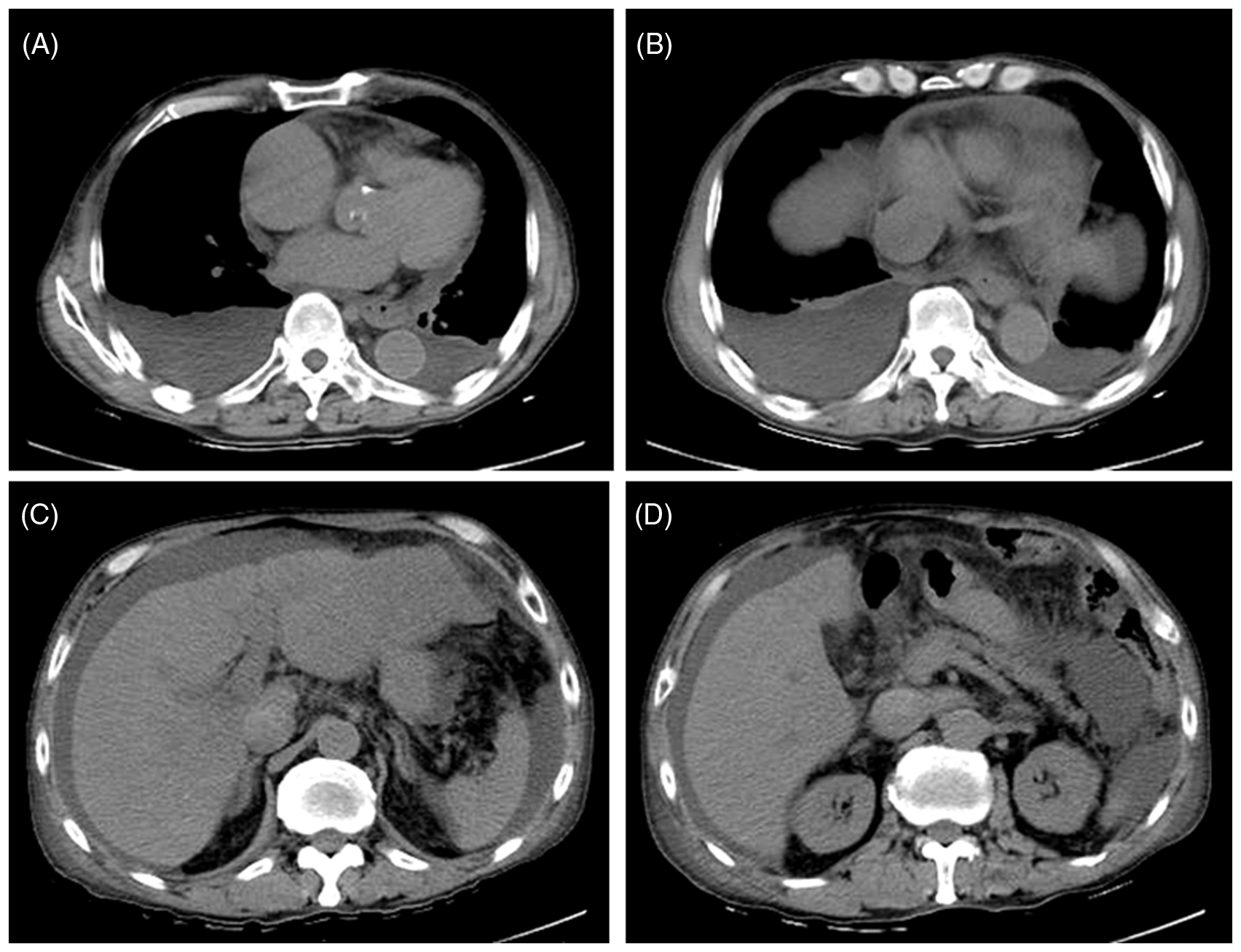

Discussion
HCC is known to have a marked propensity for vascular invasion and extension. 2 While approximately 70% of patients with HCC exhibit hepatic vein and portal vein invasion, tumor encroachment into a cardiac cavity is very rare.2,3 The incidence of tumor thrombus in the RA is as low as 0.5%–7.0%. 4 In the case of a mobile mass formation in the cardiac cavities, ball valve thrombus syndrome presenting with cardiac murmurs, respiratory distress, syncope, and/or shock causing sudden cardiac death may occur. 1
Several cases of aggressive surgical resection of tumor thrombus in the IVC and the RA with advanced HCC have been reported since the 1980s.4–8 While in some cases, curative resection of the primary tumor can prolong the survival period, early recurrence in the remaining liver or lung metastasis continues to be a problem after aggressive radical surgery.4–6,8 Yokoi and colleagues 4 reviewed 15 reports of 18 cases of surgical resection of HCC with tumor thrombus in the RA. Five patients in whom thrombectomy in the RA alone was performed, died within 8 months due to liver failure, lung metastasis, or recurrence of tumor thrombus. Among the 13 patients who underwent primary tumor resection and thrombectomy in the RA, 3 survived for more than 2 years. The mean survival period of all patients was 11 months. 4
In our case, tumor thrombus in the IVC and the RA was almost completely removed via the RA under extracorporeal circulation and intermittent hypothermic circulatory arrest. The primary HCC lesion was treated with adjuvant transcatheter arterial chemoembolization. Ultimately, the patient survived for 6 months after the cardiac tumor resection. In this case of RA obstruction due to cardiac extension of HCC, surgical resection of the tumor in the IVC and the RA was effective in treating the hemodynamic compromise.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.