
Abstract
A 62-year-old woman with Takayasu arteritis and 2 prior aortic valve replacements, was admitted with unstable angina. Computed tomographic angiography showed a newly developed right coronary artery-to-right bronchial artery fistula. Because of dense aortic calcification, catheter embolization was undertaken, which was successful. We believe the acquired coronary artery fistula developed after her uneventful second aortic valve surgery, due to inevitable trauma to the mediastinum and ascending aorta, and partly due to her underlying Takayasu arteritis.
Keywords
Introduction
A coronary artery fistula (CAF) occurs between a coronary artery and a cardiac chamber or another vascular structure. For the congenital type of CAF, the incidence is approximately 0.1%–0.2% in adult patients referred for cardiac catheterization. 1 For acquired CAF, the exact incidence is unknown, and there are only a few case reports. We describe a case of acquired coronary artery-to-bronchial artery fistula found 5 years after aortic valve surgery in a patient with Takayasu arteritis.
Case report
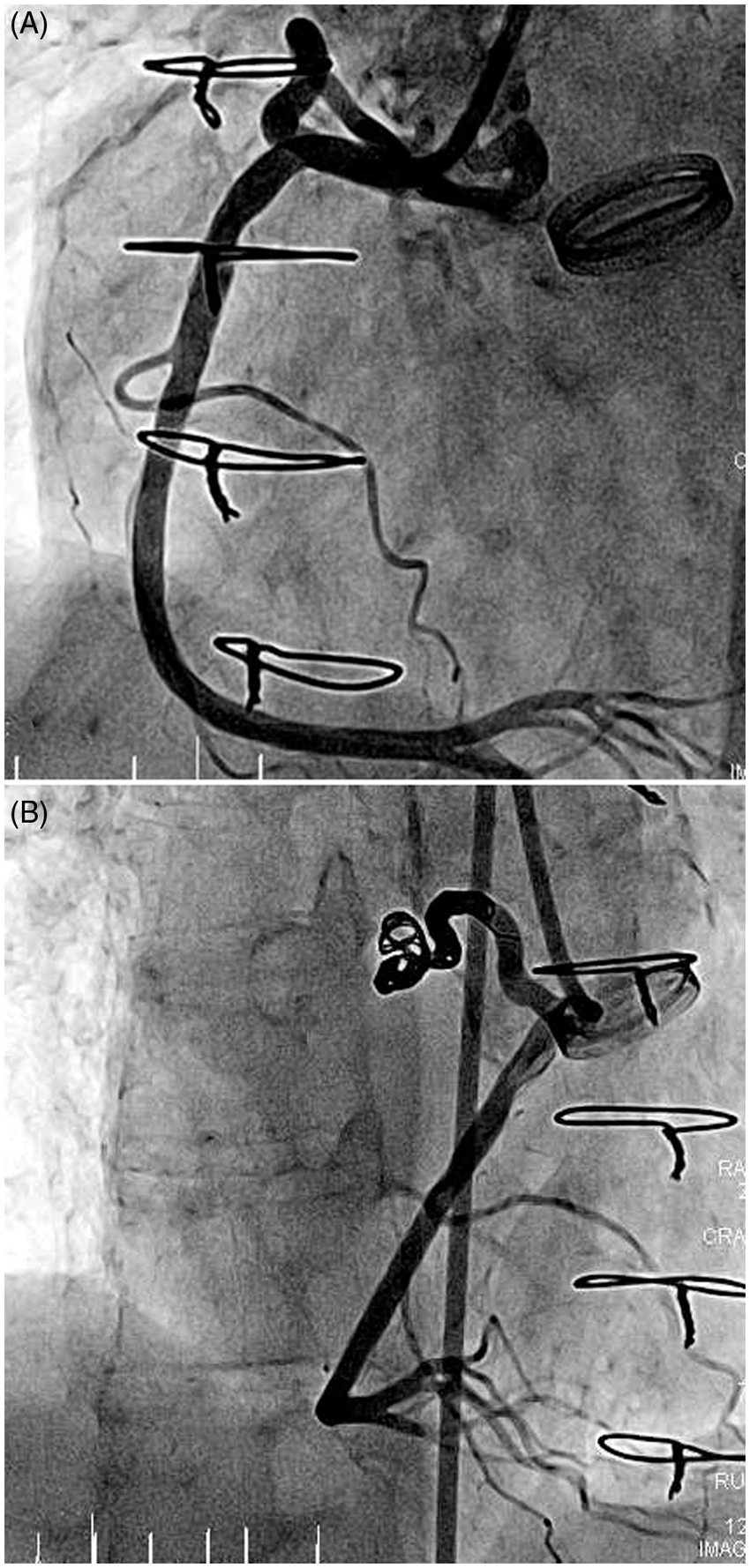
A 62-year-old woman was admitted because of exertional dyspnea and unstable angina. She had been diagnosed with hypertension 20 years earlier, and Takayasu arteritis 12 years earlier. She had undergone aortic valve replacement with a bioprosthesis 14 years earlier, and received redo aortic valve replacement with a mechanical valve (Top-Hat 19 mm) 9 years later. On admission, her physical examination, initial 12-lead electrocardiogram, and blood gas analysis were within normal limits. Chest radiography showed enlarged pulmonary arterial trunks. Coronary computed tomographic angiography showed normal native coronary arteries, but new collateral blood flow from the proximal right coronary artery to the bronchial artery was found (Figure 1). To identify the clinical implication of the collaterals, we performed cardiac single-photon emission computed tomography and found reverse redistribution in the apical inferior wall. Decreased perfusion was more prominent on rest images (Figure 1 upper row) than stress images (Figure 1 lower row). This finding was consistent with the patient's symptoms which were more severe during rest than exercise. Coronary angiography showed a right coronary artery-to-bronchial artery fistula (Figure 2). Transthoracic echocardiography showed a normal ejection fraction and valve function. Because the patient had 2 prior cardiac operations and there was extensive calcification of the ascending aorta, we decided to proceed to catheter-based embolization first, to avoid the hazards of a third-time sternotomy. After selective angiography, the coronary artery-to-bronchial artery fistula was selected with a 2.4F microcatheter and embolized with polyvinyl alcohol particles (Contour 500-700, Boston Scientific, Natick, MA, USA) and multiple microcoils (Figure 2). On completion, angiography showed no visible fistula tracks. After embolization, the symptoms resolved.
Preembolization imaging. (A) Coronary computed tomography showing the right coronary artery-to-bronchial artery fistula. (B) Cardiac single-photon emission computed tomography showing reverse redistribution of perfusion. The upper 2 sets are axial images, and lower 2 sets are sagittal images of the heart. In each set, the upper row is the resting images and the lower row is stress images. Endovascular embolization of the fistula. (A) Preembolization image showing a large fistula originating from the proximal right coronary artery and (B) After embolization, no fistulous communication is seen.
Discussion
CAFs are rare congenital or acquired abnormalities having anomalous terminations of the coronary arteries. There is no consensus in the classification of CAF, but they can be divided according to the etiology (congenital vs. acquired) or types of communication (coronary-to-systemic vs. coronary-to-pulmonary). 2 For the coronary-to-systemic type, fistulous communications may terminate directly in a cardiac chamber, the bronchial circulation, the coronary sinus or vein, or the venae cavae. 3
Among coronary-to-systemic fistulae, coronary-to-bronchial artery fistula (CBF) has been reported in 0.61% on cardiac multidetector computed tomography. 4 A CBF can present secondary to occlusive disease of the pulmonary arteries or chronic pulmonary inflammation, such as bronchiectasis or cystic fibrosis.5,6 There is little known about the possible mechanisms of postoperative acquired CAF or CBF, mainly due to the rare incidence of fistulae. In one report of acquired diagonal artery-to-pulmonary vein fistula 30 years after open mitral commissurotomy, it was suggested that CAF might be caused by blunt trauma over the anterior left ventricle during surgery or chest tube positioning. 3 In our patient, the Takayasu arteritis was well controlled and not currently active. There are two possibilities: CBF was formed by longstanding Takayasu arteritis that resulted in the pulmonary arterial disease, or by mediastinal adhesions and inflammation attributable to the 2 previous cardiac operations.
Surgical correction is indicated for a large fistula with high flow, multiple communications, very tortuous pathway, multiple terminations and/or significant aneurysmal formation. 7 In spite of developments in surgical techniques and instruments, a redo operation still has some risk to the patient, and endovascular treatment is an attractive alternative in this setting. 6 There are only a few case reports and no long-term clinical results of embolization yet, because of the low incidence of these conditions. Regarding the nature of the inflammation, special consideration should be taken in the choice of treatment. Since immunosuppressive or steroid therapy might adversely affect long-term outcomes, close observation is needed to monitor for infection, dislocation, recurrent aneurysm, or fistula development. 8
Acquired CAF after cardiac surgery is extremely rare. To our knowledge, this is the first case of an acquired coronary-to-bronchial fistula after redo aortic valve replacement in a patient with Takayasu arteritis. It can be treated successfully and safely by embolization.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.