
Abstract
Background
We report the results of complete video-assisted thoracoscopic surgery for treatment of primary non-small cell lung cancer, which was performed completely through the monitor in 400 consecutive patients.
Patients and methods
Between September 25, 2002 and August 25, 2011, a retrospective database of 400 consecutive patients who underwent complete video-assisted thoracoscopic surgery for treatment of primary non-small cell lung cancer was reviewed. Demographic, histopathologic, preoperative, perioperative, postoperative, and outcome variables were assessed using standard descriptive statistics and Kaplan-Meier survival analyses.
Results
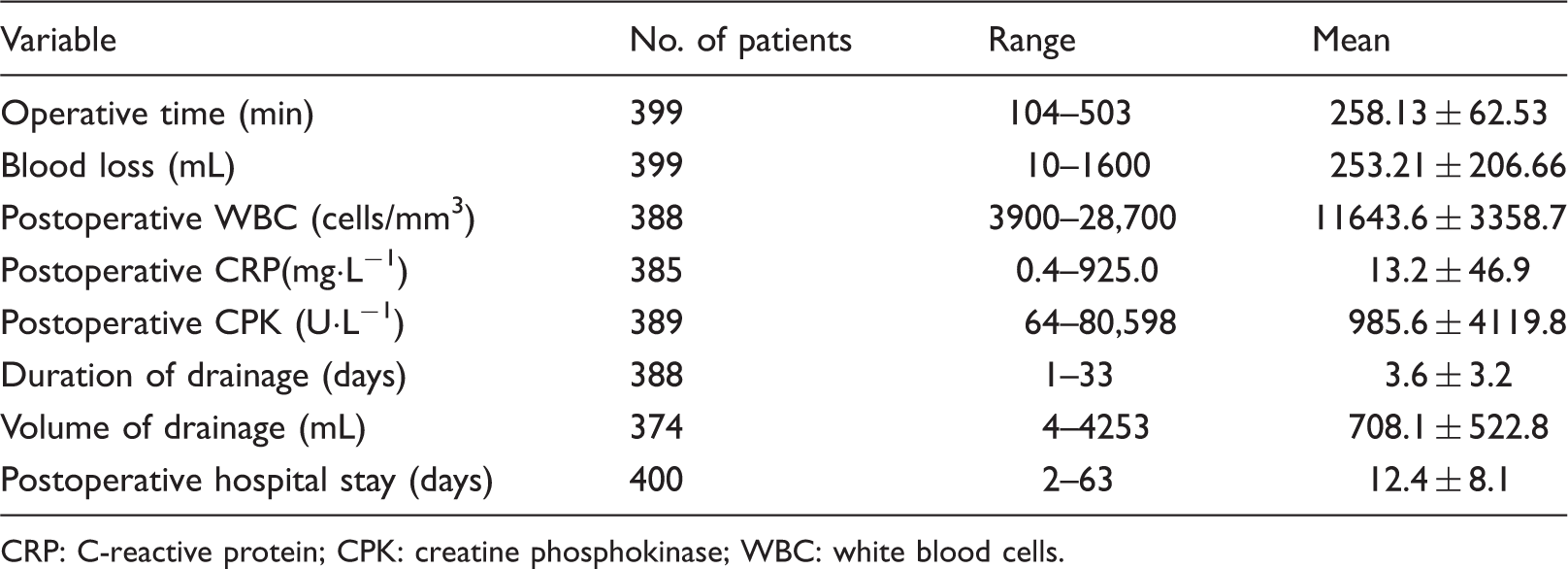
Operating time was 258.13 ± 62.53 min, volume of blood loss was 253.21 ± 206.66 mL, duration of drainage was 3.6 ± 3.2 days, volume of drainage was 708.1 ± 522.8 mL, the postoperative respiratory complication rate was 14.8%, the reoperation rate was 1.3%, and operative mortality was 1.0%. The 5-year postsurgical survival rates for pathologic stages I, II, and III were 93.9%, 62.0%, and 61.6%, respectively; the 3-year postsurgical survival rate for pathologic stage IV was 40.0%
Conclusions
Complete video-assisted thoracoscopic surgery for treatment of primary non-small cell lung cancer is associated with safety and acceptable postoperative complication rates, operative mortality rates, and survival rates.
Keywords
Introduction
The role of thoracoscopic surgery for treatment of primary non-small cell lung cancer has become increasingly accepted. Surgeons are still aware of intraoperative safety and long-term oncologic concerns. 1 Many believe that thoracoscopic surgery might leave unrecognized tumor tissue within lymph node drainage areas, fissure staple lines, and at the bronchial margins; and furthermore, that it might cause pleural tumor seeding from lung manipulation and fail to identify second primary cancers because of the lack of bimanual lung palpation. 2 Therefore, we undertook this study to review our experience of complete video-assisted thoracoscopic surgery (VATS) for the treatment of primary non-small cell lung cancer.
Patients and methods
Between September 25, 2002 and August 25, 2011, 413 patients with clinical stage I primary non-small cell lung cancer were referred for surgical treatment at the Division of Thoracic Surgery, Department of Surgery, Nippon Medical School. Complete VATS was advised. The primary treatment in all patients included in this study was surgical resection by segmentectomy or lobectomy combined with mediastinal lymph node dissection. We converted to a minithoracotomy in 13 patients because of bleeding from the pulmonary artery and/or vein in 11 cases (blood loss in these 11 cases was 350–3900 mL, mean 1334.82 ± 1102.82 mL). The reason for the maximal 3900 mL blood loss was stapling trouble due to pulmonary vein injury. One case was converted to a minithoracotomy due to difficulty in finding the interlobar pulmonary artery in the left upper lobe, and another due to difficulty in making pleural space in a small patient (height 149 cm, weight 54 kg). The database of 400 consecutive patients who had complete VATS was analyzed retrospectively.
The surgical techniques for complete VATS segmentectomy were the same as those for complete VATS lobectomy. The procedures were performed under general anesthesia with one-lung ventilation by a double-lumen endotracheal tube. The patient was placed in the lateral decubitus position with flexion of the operating table at the level of the mid-chest, which allowed splaying of the ribs to improve exposure. The surgeon always stood on the right side of the patient. For right-sided procedures, the first port was at the 7th or 8th intercostal space in a mid-axillary line which was 1.5 cm long. This port was for placement of the 30-degree thoracoscope. The second port was a minithoracotomy 3–5-cm long at the 5th intercostal space between the anterior to mid-axillary line. The third port was 1.5-cm long at the mid-axillary line to the front edge of the lower angle of the scapular at the 6th intercostal space. The fourth port was 1.5-cm long at the 3rd intercostal space between the anterior to mid axillary line. For left-sided procedures, the first port was 1.5-cm long at the 7th or 8th intercostal space in the mid-axillary line. This port was for placement of the 30-degree thoracoscope. The second port was a minithoracotomy of 3–5-cm long at the 4th or 5th intercostal space between the anterior to mid-axillary line. The third port was 1.5-cm long at the 5th intercostal space in the anterior axillary line. The fourth port was 1.5-cm long at the front edge of the lower angle of the scapula of the 3rd intercostal space.
The following procedures were performed completely under the monitor. Hilar structures were dissected. Pulmonary veins and arteries were cut with an automatic stapling device or by ligation using a knot-pusher, according to anatomical circumstances. The bronchus was cut by the stapling device. The segmental border (in the case of segmentectomy) or the lobation (in the case of lobectomy) were completely divided using the stapling device. The lung specimen was placed in a plastic bag and removed through the second port.
Mediastinal lymph node dissection was performed at the upper mediastinal level and the hilar level. For right mediastinal lymph node dissections, a 30-degree thoracoscope was inserted through the fourth trocar port. The mediastinal pleura was opened along the azygos vein and the superior vena cava. The right subclavian artery, innominate vein, vagus nerve, and the branch of the recurrent nerve were exposed. Lymph nodes were dissected with adipose tissue distally from the upper mediastinum. The azygos vein was exposed and lymph node dissection was carried out caudally from the upper mediastinum to the tracheobronchial area. Dissected lymph nodes were connected to the bronchial lymph nodes by passing below the azygos vein toward the tracheal side. The region between the pulmonary artery and the bronchus and the ventral side of the pulmonary artery was dissected. Subsequently, the mediastinal pleura was opened around the pericardium, esophagus, and the intermediate bronchus at the caudal side of the azygos vein. Dissection was continued to between the pericardium and esophagus toward the carina associated with the upper mediastinum. The bifurcation of the trachea was retracted to facilitate subcarinal lymphadenectomy. For left mediastinal lymph node dissection, a 30-degree thoracoscope inserted via the fourth port offers an excellent operative view. The mediastinal pleura was opened. The vagus nerve was dissected and exposed. In these procedures, the paraaortic lymph nodes were dissected. The #5 lymph nodes at the Botallo ligament and around the recurrent nerve were dissected. Bronchial lymph nodes #10 behind the left main bronchus were dissected towards the bifurcation of the upper and lower lobe bronchus. Subsequently, lymphadenectomy was continued along the esophagus towards the foot side until the back of the carina was reached. Lymphadenectomy behind the carina was performed and continued towards the ventral side. Finally, bleeding and air leakage were checked. A pleural drainage tube was placed via the first port with another catheter drain.
All statistical analyses were performed with IBM SPSS version 19 (IBM SPSS Statistics, IBM Corp., Armonk, NY, USA). The data are shown as mean ± standard deviation. The data of both groups were compared using unpaired t tests or the chi-square test. Survival rates were calculated by Kaplan-Meier estimated survival curves, and the significance of the difference was analyzed by the logrank test. A p value < 0.05 was considered significant.
Results
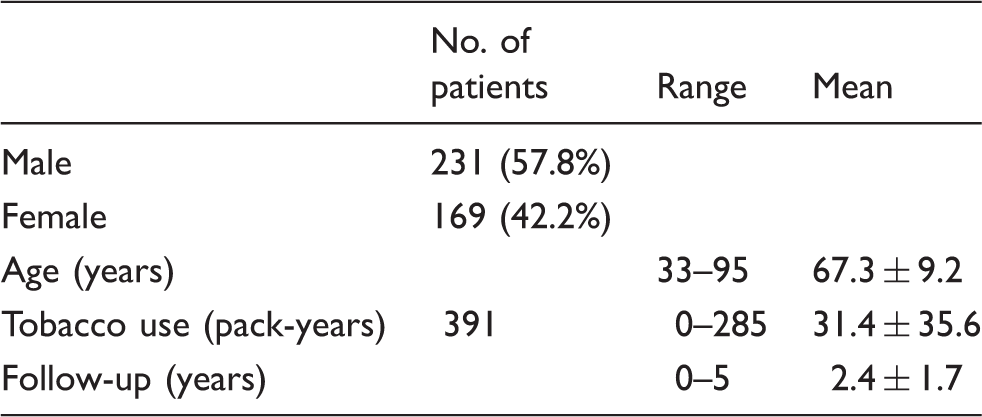
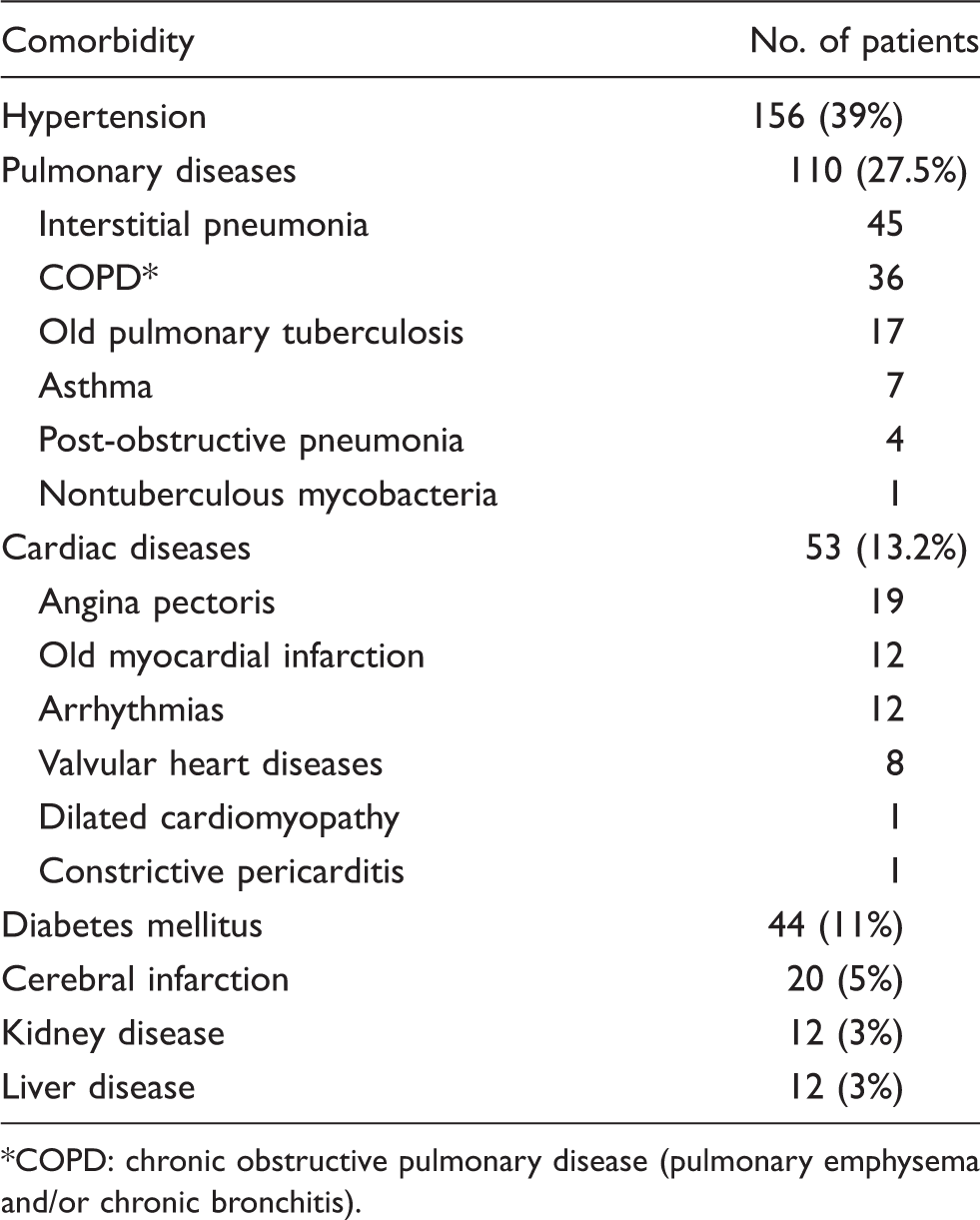
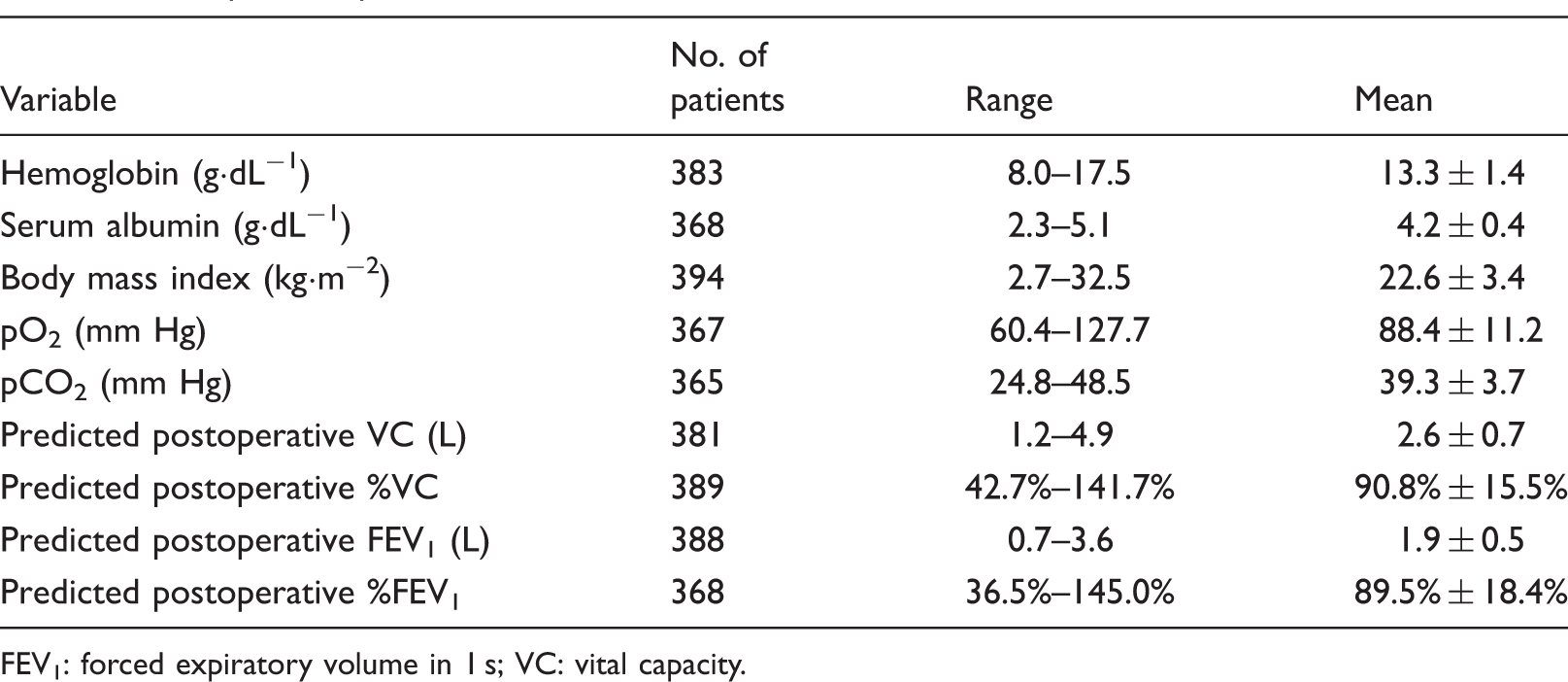
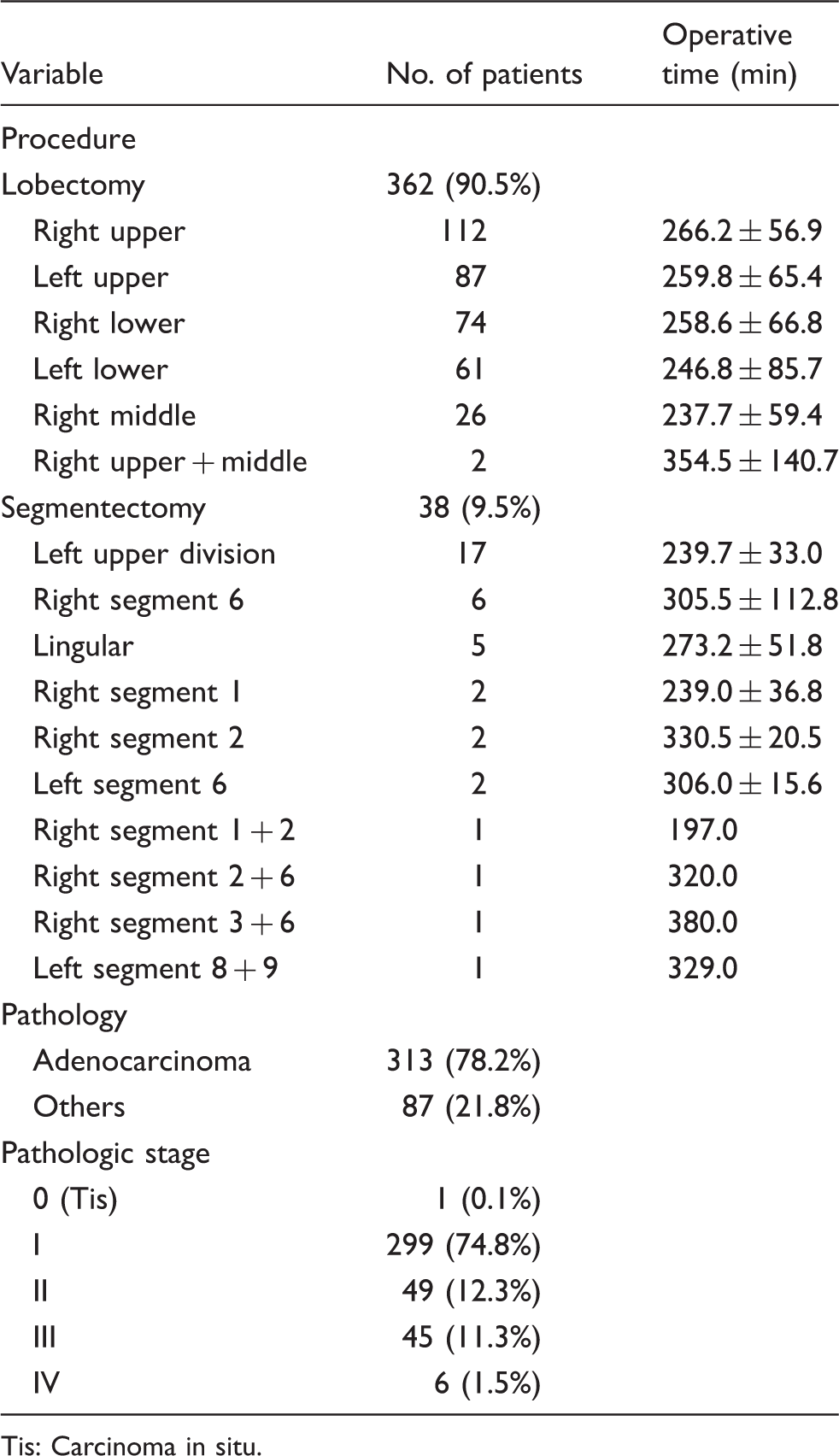
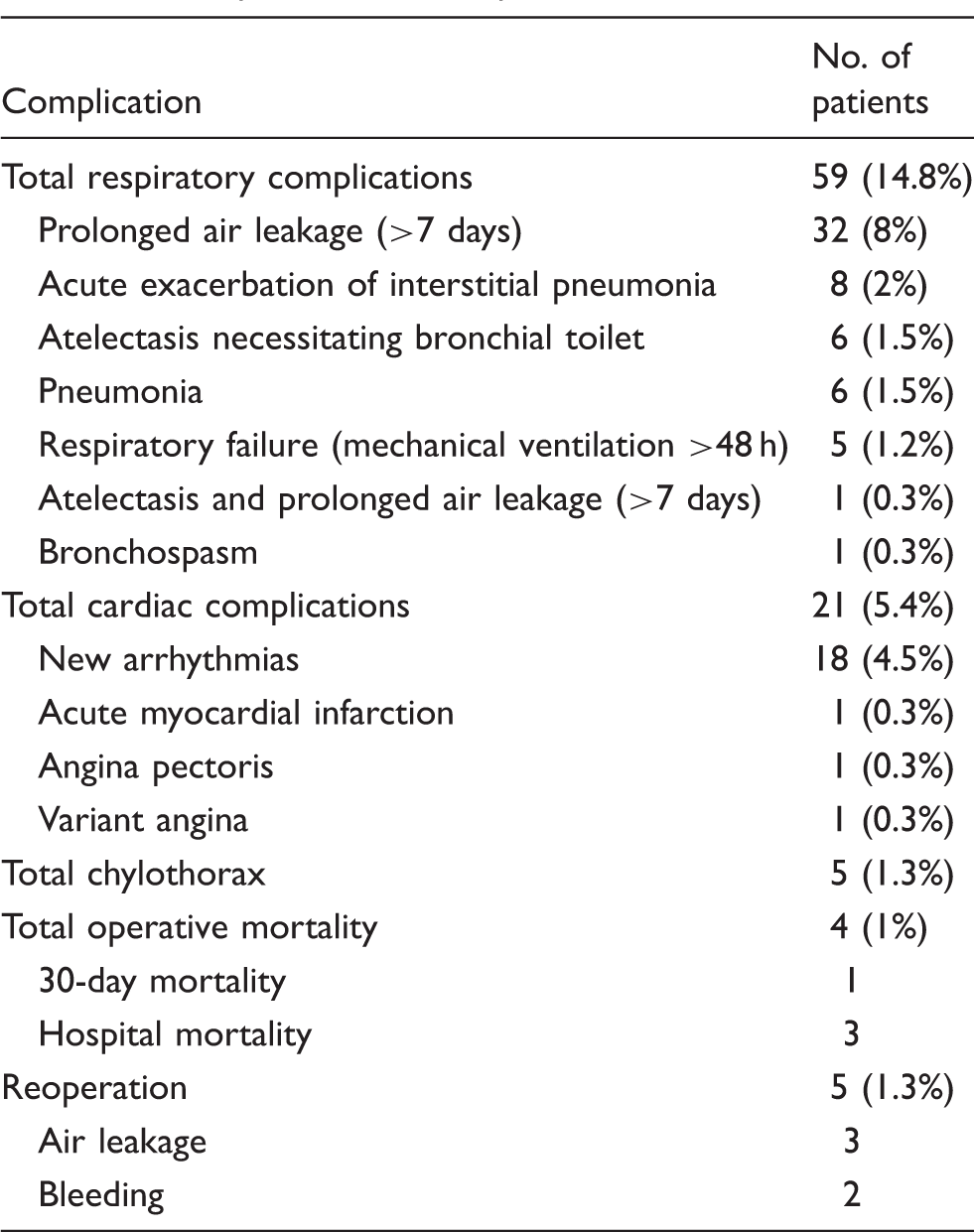
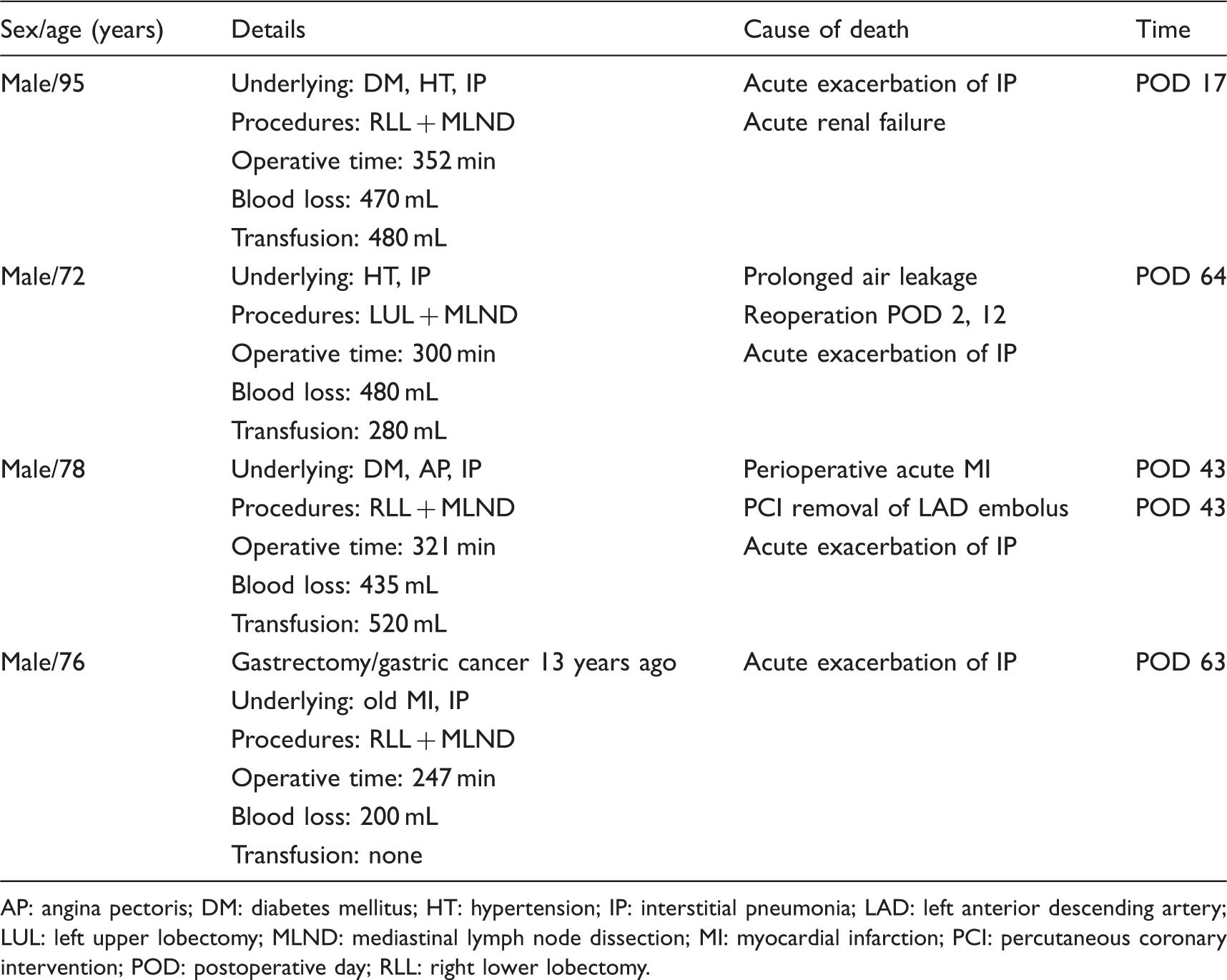
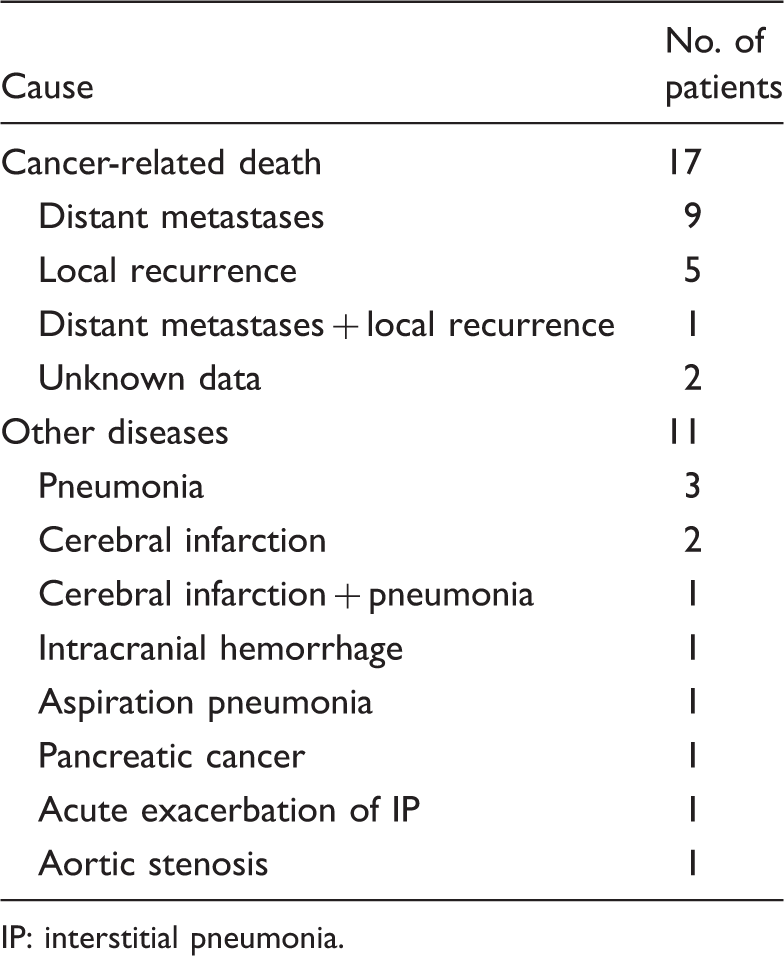
There were 231 men and 169 women with a mean age of 67.3 ± 9.2 years included in our study. Mean follow-up was 2.4 ± 1.7 years (Table 1). Hypertension, pulmonary diseases, cardiac diseases, and diabetes mellitus were among the most common comorbidities (Table 2). Mean body mass index was 22.6 ± 3.4 kg·m−2. Mean pO2 was 88.4 ± 11.2 mmHg, and mean pCO2 was 39.3 ± 3.7 mmHg. The mean predicted postoperative percentage of forced expiratory volume in 1 s (%FEV1) was 89.5% ± 18.4%, with a range of 36.5% to 145% (Table 3). There were 362 lobectomies and 38 segmentectomies (Table 4), mean operative time was 258.13 ± 62.53 min. There were 75 (18.8%) cases in which the recorded operative time included the 40-min waiting time for a frozen section procedure. The most common pathology was adenocarcinoma in 78.2%, and the percentage of patients in pathologic stages 0–IV are given in Table 4. Perioperative and postoperative data are given in Table 5. Respiratory complications were the most common complications, found in 59 patients (Table 6). Among these, prolonged air leakage (>7 days) was the most frequent complication. Predicted postoperative FEV1 (p = 0.013) and predicted postoperative %FEV1 (p = 0.003) were risk factors for postoperative respiratory complications. Heart disease was also a risk factor for postoperative respiratory complications (p = 0.027), but we do not have data about the relationship between cardiac function and postoperative respiratory complications. New cardiac arrhythmias were the most common cardiac complications, and were mostly atrial fibrillation and paroxysmal supra-ventricular tachycardia. Chylothorax was found in 5 patients and all were healed conservatively (Table 6). Reoperation was required in 5 patients due to continuous air leakage and postoperative bleeding. Operative death occurred in 4 patients (Table 7). After primary resection, 17 (4.3%) patients were diagnosed with a local recurrence and/or distant metastases. The 5-year postsurgical survival rates for pathologic stages I, II, and III were 93.9%, 62.0%, and 61.6%, respectively (Figure 1). The 3-year postsurgical survival rate for pathologic stage IV was 40.0%. Overall causes of death are listed in Table 8.
Kaplan-Meier analysis of survival after complete video-assisted thoracic surgical resection. Characteristics of 400 patents. Comorbidities in 400 patents. COPD: chronic obstructive pulmonary disease (pulmonary emphysema and/or chronic bronchitis). Preoperative profile. FEV1: forced expiratory volume in 1 s; VC: vital capacity. Procedures, pathology, pathologic stage, and operative time. Tis: Carcinoma in situ. Perioperative and postoperative profile. CRP: C-reactive protein; CPK: creatine phosphokinase; WBC: white blood cells. Complications in 400 patients. Details of 4 hospital deaths. AP: angina pectoris; DM: diabetes mellitus; HT: hypertension; IP: interstitial pneumonia; LAD: left anterior descending artery; LUL: left upper lobectomy; MLND: mediastinal lymph node dissection; MI: myocardial infarction; PCI: percutaneous coronary intervention; POD: postoperative day; RLL: right lower lobectomy. Causes of death. IP: interstitial pneumonia.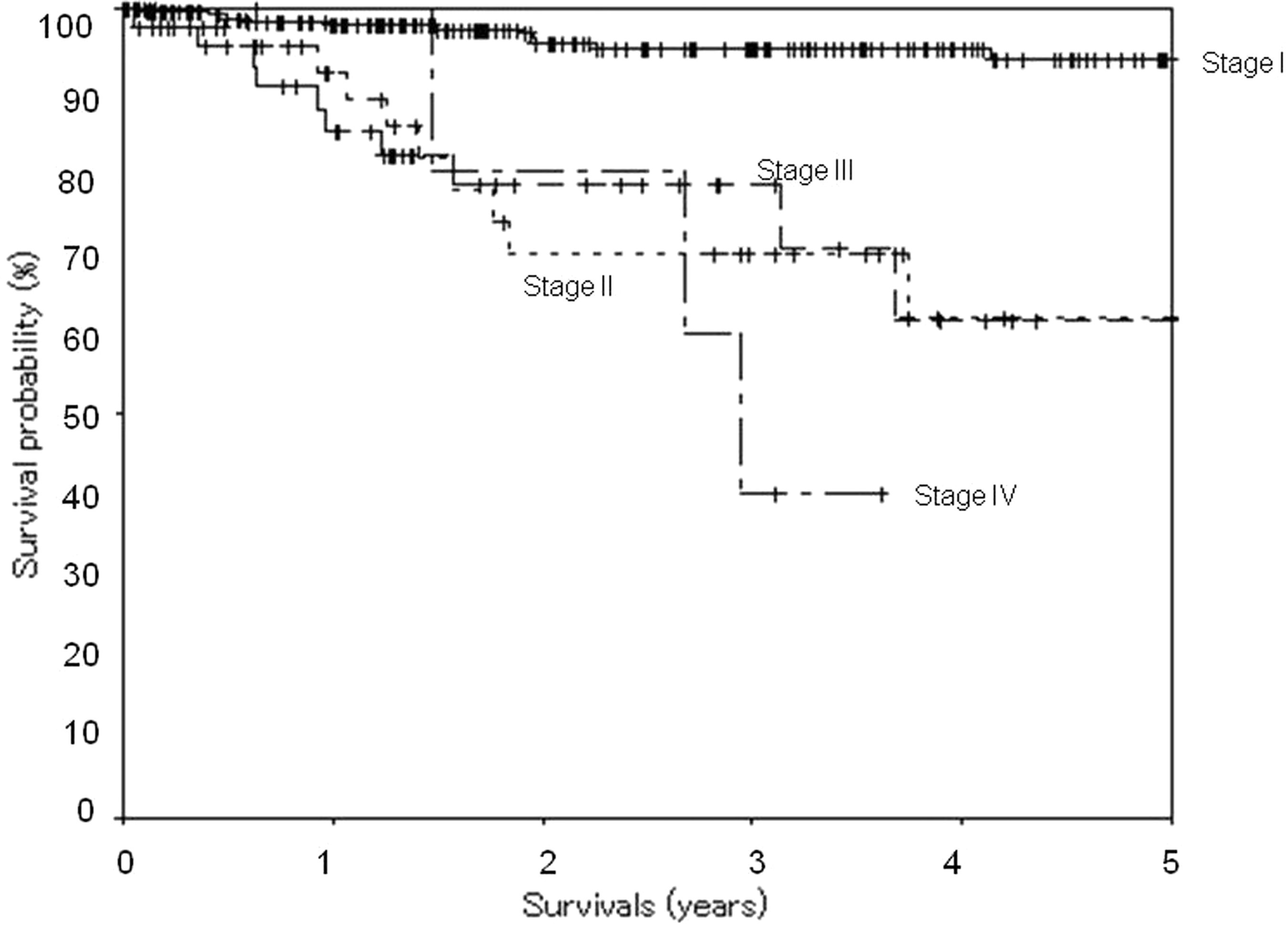
Discussion
Nowadays, a thoracoscopic approach is an acceptable alternative to an open operation for lobectomy, pneumonectomy, segmentectomy, and wedge resection of non-small cell lung cancer. 3 While immune function is an important factor in controlling tumor growth and recurrence, much literature suggests that the immune response is better preserved after thoracoscopic surgery than thoracotomy.4–7 This supports the thoracoscopic approach, but the greatest concerns are about safety, oncologic efficacy, and long-term survival when comparing it to the conventional open approach. 8 Morbidity and mortality are no greater in thoracoscopic resections than in an open approach. 9 The postoperative mortality rate after thoracoscopic resection for lung cancer is low.10–12 Our experience demonstrates that the morbidity and mortality rate was acceptably low. All deaths were related to postoperative acute exacerbation of interstitial pneumonia which is triggered by perioperative stress. 13 Longer operative time may probably be a risk factor for acute exacerbation of interstitial pneumonia. Careful preoperative evaluation of patients with a history of interstitial pneumonia will help to reduce mortality. Since we cannot conclude that thoracoscopic surgery is better than thoracotomy for patients with lung cancer and interstitial pneumonia, 14 a muscle-sparing thoracotomy could be an alternative to reduce operative time hence reduce the risk of acute exacerbation of interstitial pneumonia. In our series, we demonstrated high postoperative levels of C-reactive protein and creatine phosphokinase in a few patients. Because C-reactive protein and creatine phosphokinase relate to inflammation and tissue damage, we could not find any relationship with their postoperative incidence. Respiratory complications were the most common complication after thoracoscopic procedures in our experience. Careful preoperative pulmonary evaluation and intensive postoperative pulmonary care will reduce pulmonary complications.
The reoperation rate of 1.3% was due to bleeding and air leakage. Careful intraoperative inspection for air leakage by a water-seal test along the staple line and bronchial stump is of great importance. Reinforcement suturing with pledgets and/or a polyglycol acid sheet with fibrin glue coverage along the staple line will cease or prevent air leakage. While thoracoscopic procedures have been taught and practiced widely, the morbidity, mortality, reoperation rates, and operative time should be reduced. The most serious and dangerous event during the procedure is heavy bleeding from a pulmonary vessel.15,16 Attempted hemostasis by immediately applying pressure for control of the bleeding should be undertaken before any other procedures. 16 Uncontrolled bleeding from a pulmonary vessel along with difficulty in making the lobation and/or difficulty in hilar dissection from dense fibrous adhesion caused us to convert to minithoracotomy without rib resection in 14 of 414 patients or 3.4%. In our experience in the present series, there was no conversion to a conventional open thoracotomy. According to Asamura and colleagues 17 in 2008, the 5-year postsurgical survival rates for pathologic stages IA, IB, IIA, IIB, IIIA were 83.9%, 66.3%, 61%, 47.4%, and 32.8% respectively. Recently Sawabata and colleagues 18 reported that the 5-year postsurgical survival rates for the same stages were 86.8%, 73.9%, 61.6%, 49.8%, and 40.9% respectively. They also conclude that the overall 5-year survival rate for surgical cases was 69.6%. Thoracoscopic lobectomy and conventional open lobectomy demonstrate similar 5-year survival rates, while thoracoscopic lobectomy is associated with fewer complications.12,19,20 In our study, the 5-year postsurgical survival rates in pathologic stage I, II, and III were 93.9%, 62.0%, and 61.6%, respectively. The 3-year postsurgical survival rates in pathologic stage IV was 40.0%. Recurrence was documented in 15 cases. Because the mean follow-up period was 2.4 ± 1.7 years, we need a longer period of time before a conclusion about survival rates can be made. We totally agree with Congregado and colleagues 15 that if thoracoscopic surgery is properly performed and meets oncological criteria for lung cancer surgery, long-term survival should not be affected. For oncologic efficacy, careful preoperative evaluation, accurate clinical staging, suitable operative manipulation, and complete mediastinal lymph node dissection should be achieved. 21 Nodal dissection via a VATS approach is comparable to nodal dissection through a thoracotomy. 22 We saw 5 cases of postoperative chylothorax, all of which healed conservatively. Many reports suggest that thorough lymph node dissection may improve disease-free survival compared to only sampling. 23 For this reason, we continue to perform lymph node dissections in all lung cancer cases.
Because of the visualization, the thoracoscope indeed helps the thoracic surgeon, even in an open thoracotomy. For non-small cell lung cancer, we recommend complete VATS in clinical stage 1, peripheral nodules, good lobation, and no hilar lymph node swelling. If hilar nodes are swollen but inflammation is not present, we would continue with complete VATS because it is easier to dissect them from the pulmonary artery, and thus more safely. If pneumonectomy has to be carried out, or there is a hilar tumor, peripheral tumor >5 cm in diameter, poor lobation, lymph node adhesion to the pulmonary artery which is difficult to dissect, an N1 case, or previous radiation to the hilar or mediastinal area, it is reasonable to proceed with a conventional open thoracotomy. From the point of view of pulmonary function and cardiovascular status, the general perception is that VATS had less effect compared to thoracotomy; 24 thus we would recommend complete VATS in a low performance status patient. Patients with Eastern Cooperative Oncology Group performance status 2 or more and low predicted postoperative FEV1 of approximately 1000 mL, are often contraindicated for open surgery. From our previous work, patients with an operative time >297 min in VATS lobectomy for lung cancer developed significant postoperative respiratory complications; 25 thus we routinely attempt to complete the lobectomy stage within 3 h. If we cannot not finish on time, we convert to an open thoracotomy to complete the procedures within 5 h. In this study, the operative times of complete VATS are longer than those of conventional open surgery. However, we think that VATS training and improvement of team work are most important and will eventually overcome these difficulties. This study demonstrates that complete VATS is a feasible approach to the management of primary non-small-cell lung cancer, with safety and acceptable low morbidity and mortality rates.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.