
Abstract
The purpose of this review is to compare conventional endovascular procedures and the robotic endovascular approach in aortic aneurysm repair. Despite advantages over open surgery, conventional endovascular surgery has limitations. To develop an alternative, efforts have been focused on robotic endovascular systems. Two of the 3 studies comparing procedure times demonstrated reduced procedure time in the robotic group, by 6 times (p < 0.05). One study demonstrated that robotic procedures reduced fluoroscopic exposure time by 12 minute (p < 0.001). Three in-vitro studies showed that the number of movements required in robotic surgery was reduced up to 10 times (p < 0.05). One of 2 studies measuring robotic performance score showed a better performance score in the robotic endovascular group (p = 0.007). These results demonstrate that the robotic technique has multiple advantages over the conventional procedure, including improved catheter stability, a shorter learning curve, reduced procedure time, and better performance in cannulating tortuous vessels. However, robotic endovascular technology may be limited by the cost of the system, the size of the catheter, and the setup time required preoperatively. Further comparative studies between conventional and robotic approaches regarding cost-effectiveness, safety, and performance in cases involving complex anatomy and fenestrated stent grafts are essential. Nevertheless, this revolutionary technology is increasingly popular and may be the next milestone in endovascular surgery.
Keywords
Introduction
There have long been two common approaches to the management of vascular diseases: open surgery and endovascular surgery. More and more patients are receiving endovascular procedures worldwide because they are minimally invasive and better suited to high-risk patients. It is also possible to carry out multiple endovascular procedures in the same operation.1,2 However, the endovascular approach has many catheter-related limitations. 3 With limited shapes and sizes, there is difficulty in steering without maneuverability at the tip. More frequent catheter changes and repeated cannulation attempts would also prolong the procedure, hence increasing the risk of vessel dissection and distal embolism. Manually steerable catheters allow only unidirectional movement with limited degrees of freedom. Their fixed stiffness often hinders applications of torque. As a result, it can be very difficult to use them for interventions on arteries with complex anatomy. Their usage is also heavily skill-dependent. In view of these prominent limitations, tremendous effort has been spent on developing better alternatives to conventional endovascular surgery.
Clinical studies on the feasibility of robotic endovascular surgery
Robotic surgery has been used for more than 20 years. It was first employed in 1985 for neurosurgical biopsies. 4 Since then, it has been applied in different specialties, especially by gynecologists, urologists and colorectal surgeons operating within the confined space of the pelvis. In recent years, robotic surgery has found applications in vascular surgery, which can potentially reduce the limitations of current endovascular techniques. It was first used in vascular surgery in 2002, in robotic-assisted laparoscopic aorto-bifemoral bypass. 5 Since then, the feasibility of using robotic assistance in vascular surgery has been studied, and robotic endovascular surgery has been put into practice.
Two studies on cardiac catheter ablation were published in 2008, using the robotic steerable sheath system. Both studies demonstrated superior catheter stability and greater mobility and control of the catheter tip. Robotic catheters also provide better range and flexibility.6,7 An in-vitro study published in 2009 used a 4-vessel fenestrated stent graft to evaluate the role of robotic endovascular techniques in fenestrated graft stenting. Fifteen experienced operators were recruited to cannulate the silicon model with both conventional catheters and the robotic system. Results from the study indicated that the robotic technique enhanced target vessel cannulation, reduced instrumentation, and improved overall performance scores. 8 An interesting aspect was that fast learning curves were observed in experimental endovascular robotic therapy. This is in contrast to robotic surgery which is known to have relatively slow learning curves.
Application of robotic catheters in patients
The first experience in a real patient was aneurysm repair in a 78-year-old man with a 5.9-cm infrarenal abdominal aortic aneurysm, who had no postoperative complications on computed tomography 3 months after the surgery. 9 This was performed in St. Mary’s Hospital, London, which at the time of writing has the only functional robotic system by Hansen Medical, and 13 cases performed up to April 2012.
The system
Like most robotic surgery, the robotic endovascular system has a remotely steerable electromechanical catheter system controlled via a “master-slave” mechanism.
10
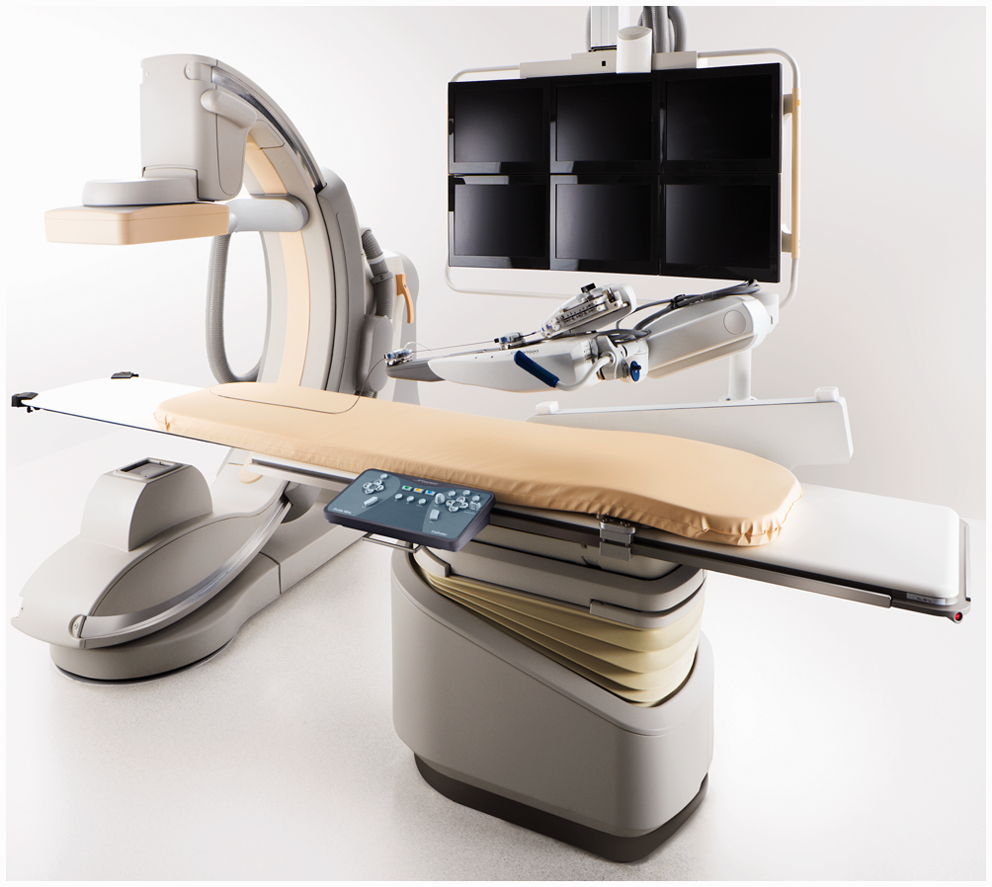
The operator steers the robotic catheter via a 3-dimensional hand-operated joystick system in the workstation, which is located outside the angiographic suite away from the radiation source (Figure 1). Robotic endovascular catheters have a flexible multidirectional inner guide with a 270-degree bend radius inside a unidirectional outer guide sheath, into which standard endovascular tools can be inserted.
11
The catheter is operated via a robotic arm on the patient’s side, and is controlled with a remote catheter manipulator (Figure 2). The robotic arm delivers the robotic endovascular catheter, according to catheter position commands received from the workstation.
The operator steers the robotic catheter via a 3-dimensional hand-operated joystick system in the workstation, which is located outside the angiographic suite away from the radiation source. The Magellan robotic endovascular system (Hansen Medical, Inc.) is a sophisticated intravascular robotic platform that integrates levels of 3-dimensional catheter control with 3-dimensional visualization, a combination that provides accuracy and stability during intravascular procedures.
Advantages of robotic endovascular surgery
Comparison of various parameters between robotic and conventional endovascular techniques.
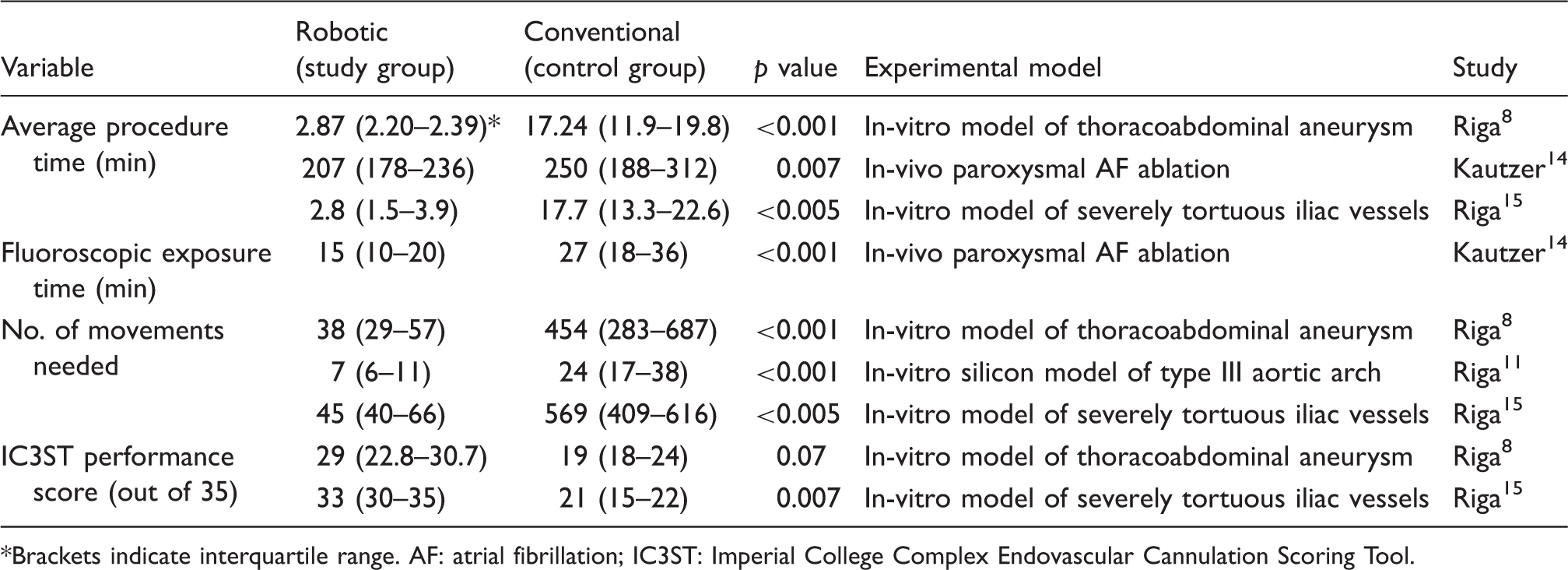
Brackets indicate interquartile range. AF: atrial fibrillation; IC3ST: Imperial College Complex Endovascular Cannulation Scoring Tool.
Average procedure time and fluoroscopic exposure time
Catheter ablation of arrhythmogenic foci is regarded as the treatment of choice for drug-refractory atrial fibrillation, but this procedure is very technically demanding, and robotic catheters have been investigated for potential improvement in performance of these ablative procedures to reduce fluoroscopic exposure time for the patient. 13 In a nonrandomized clinical study, robotic catheterization was shown to be associated with a shorter overall procedure time, by 43 minutes, with fluoroscopic exposure time halved from a mean of 27 to 15 minutes, which essentially halves the radiation exposure of the patient. 14 After this encouraging clinical result, several in-vitro studies, involving the use of computed tomography-reconstructed silicon models, have also revealed a dramatic reduction of procedure time with the use of a robotic catheter. One study showed that the median cannulation time of aortic arch vessels with normal anatomy may take only 48 seconds instead of 2.7 minutes. 11 When fenestrated graft repair was performed on a silicone model of dilated thoracoabdominal aneurysm, the average cannulation time was found to be 2.87 minutes for the robotic endovascular procedure; compared to 17 minutes taken with a conventional catheter, this is an astonishing 6-fold decrease in procedure time. 8 More importantly, technically difficult vessels, such as the left renal artery, took 0.37 minutes to cannulate instead of 7.13 minutes, representing an improvement of 19 times. 8 This shows that robotic catheters have the potential for converting anatomically difficult cannulations into swiftly achievable routines.
Stable catheter tip with reduced number of movements needed
Robotics have another inherent advantage in that the tips of the catheters have inbuilt hardware and software filters to exclude the physiological tremor of the operator that would inevitably translate into catheter tip instability in conventional endovascular operations. 12 This translates clinically into much fewer movements needed to accomplish an endovascular cannulation task, as evidenced by several in-vitro studies. In cannulating 4 visceral arteries, namely, the renal arteries, superior mesenteric and celiac arteries, in a thoracoabdominal aneurysm model, robotic catheters out-performed conventional catheters with 12-times less redundant movements; 8 in particular, to cannulate the left renal artery required only 5 movements of the robotic catheter instead of 155 made by the conventional catheter, rendering the robotic procedure 30-times more efficient. In cannulation of the left common carotid artery model, robotic catheters were able to maintain such superior stability at the carotid ostium that guidewire exchange at the vessel entrance never failed in that study; whereas in the same setting with the same operators handling the task, a conventional catheter failed to access the left common carotid artery 50% of the time. 11
Superior robotic performance in tortuous angulated vessels
Catheter stability is crucial in negotiating the tight curves of anatomically variant or degenerative vessels, which are often the cause of suboptimal performance or even procedure failure in patients with highly convoluted vessel anatomy. Indeed, in-vitro studies have explicitly addressed the question of whether robotic catheters perform objectively better than the conventional type in tortuous vessels. It was found that irrespective of iliac vessel tortuosity, robotic catheters were quicker and made less redundant movements in going through tortuous vessels to cannulate the renal arteries, with the most obvious improvement in severely tortuous vessels, performing at 6-times the speed with 12-times fewer movements than conventional catheters. 15 Similarly for angulated aortic vessels, Riga and colleagues11,12 were able to assess parameters such as procedure smoothness, time for cannulation, wire manipulation, and accidental vessel wall contact, using a video-assessed scoring system: the Imperial College Complex Endovascular Cannulation Scoring Tool (IC3ST). Out of a full mark of 35, robotic catheters scored 26 compared to 20.5 in highly angulated vessels, indicating a statistically significant improvement in procedure smoothness. It is noteworthy that the IC3ST score emphasizes a reduction in vessel trauma, and hence may imply less risk of distal embolization from dislodgement of calcified plaque, and more directly, less risk of vessel dissection. 11 This could translate into potential clinical benefits for patients with heavily calcified arteries or mural thrombi in aneurysms, who would otherwise suffer a high risk of adverse events after endovascular interventions.
Robotic learning curve compared to conventional catherization
One may suspect that with such superior performance, robotic endovascular surgery might be difficult to learn. On the contrary, studies have shown the opposite to be true. For in-vitro thoracoabdominal aneurysm repair, it was shown that no matter how many or how few conventional endovascular procedures an operator has performed before, the IC3ST score was always higher when the operator used robotic techniques after just a short course of basic training. 8 To further quantify the learning curve Riga and colleagues 10 recruited 10 medical students and trained them to perform cannulation of aortic arch vessels in 5 weeks. They were able to achieve 5- to 7-times less accidental wall hits, as well as a plateau of the learning curve both in terms of procedure time and catheter tip movements, as early as week 2, whereas the same students experienced a much slower learning curve with doubtful mastering of conventional catheterization skills even by week 4. This confers an additional advantage of robotic endovascular surgery as a much easier to learn alternative compared to conventional endovascular procedures, and possibly safer for the patient as it can be more standardized and mastered by even less experienced operators.
Limitations of robotic endovascular systems
Despite the advantages of the robotic endovascular system, there are still some drawbacks limiting its popular use. One major concern is the cost of the robotic system, which is more than US$ 600,000, with a maintenance fee of US$ 60,000–80,000 per year. Each disposable catheter also costs at least US$ 1500. 12 In addition, special adjustments in the operating room are required to accommodate the robotic endovascular system. Extra resources are also needed for staff training. 3 Another drawback of some robotic systems is that the operator cannot evaluate the amount of force applied to the tissues because there is no mechanical feedback when remotely controlling the robotic catheters. This may increase the chance of vascular injury and puncture.3,7 Such difficulty may be overcome by the force quantification gauge in newer robotic endovascular systems, which measures the contact force between catheter and tissue constantly. This information is displayed on the monitor of the workstation and translated into vibration of the controller, so that the operator can make the necessary adjustments.
In addition, the robotic endovascular catheter utilizes a 14F sheath, which may be too large for cannulation via a brachial approach. The 11F inner guide catheter is also not suitable for cannulating the common carotid artery. 11 Moreover, performing a 4-vessel fenestrated stent graft operation through the femoral approach requires placing four 7F guide sheaths in one common femoral artery. Gaining access to all 4 vessels at the same time can only be achieved through a combination of robotic and conventional approaches. 8 To overcome this shortcoming, small gauge sheaths are being developed.
Lastly, a setup time of 10 to 15 minutes is required before each robotic endovascular procedure. 3 However, the robotic system allows faster cannulation and more stability, which may compensate for the longer setup time and reduce the overall procedure time. Also, it is anticipated that with increased practice and experience with the system, the setup time will be further reduced. 12
Conclusion
The robotic endovascular system is an innovation that embraces advanced robotic technology with surgical finesse. Robotic endovascular technology has advantages over conventional endovascular surgery, including reduced procedure time, improved stability and precision, a shorter learning curve, and decreased radiation exposure for both the operator and the patient. It still has some limitations, but the technology provides a platform for these to be overcome. Further clinical studies assessing the cost-effectiveness of the endovascular robotic system and the safety and performance in complex clinical cases involving fenestrated stent grafting are necessary to promote the usage of this new technique.4,12 Although the only functional unit of this new system is in St. Mary’s Hospital, Paddington, London, other countries are catching up, with Germany and France due to install a unit soon, and Singapore and Sydney having purchasing plans as well. Most recently, there has been a single case report of robot-assisted fenestrated endovascular aneurysm repair using the Magellan system in a patient. 16 Therefore, the stage is set for this state-of-the-art robotic technology to transform the paradigm of endovascular surgery, and potentially unearth a new landscape of possibilities in the field in the years to come.
Presented at the Research Meeting, Department of Surgery, University of Hong Kong Medical Centre, Queen Mary Hospital, Pokfulam, Hong Kong, September 18, 2012.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared