
Abstract
We describe the case of an 82-year-old woman who had undergone aortic mechanical valve replacement for aortic stenosis with a small annulus, and coronary artery bypass grafting. Four years after the operation, she began to experience hemolysis. Prosthetic valve obstruction was observed but there was no paravalvular leakage or aortic regurgitation through the mechanical valve. We elected to perform apicoaortic bypass in this patient with severe hemolytic anemia secondary to a mechanical valve malfunction.
Keywords
Introduction
Prosthetic valve obstruction is one of the most serious complications of mechanical valves. 1 Turbulence of flow with high shear stress forces and abnormal flow jets through the left ventricular outflow tract (LVOT) can cause severe hemolytic anemia. We describe our experience of apicoaortic bypass in a patient with severe hemolytic anemia secondary to valve malfunction and LVOT obstruction.
Case report
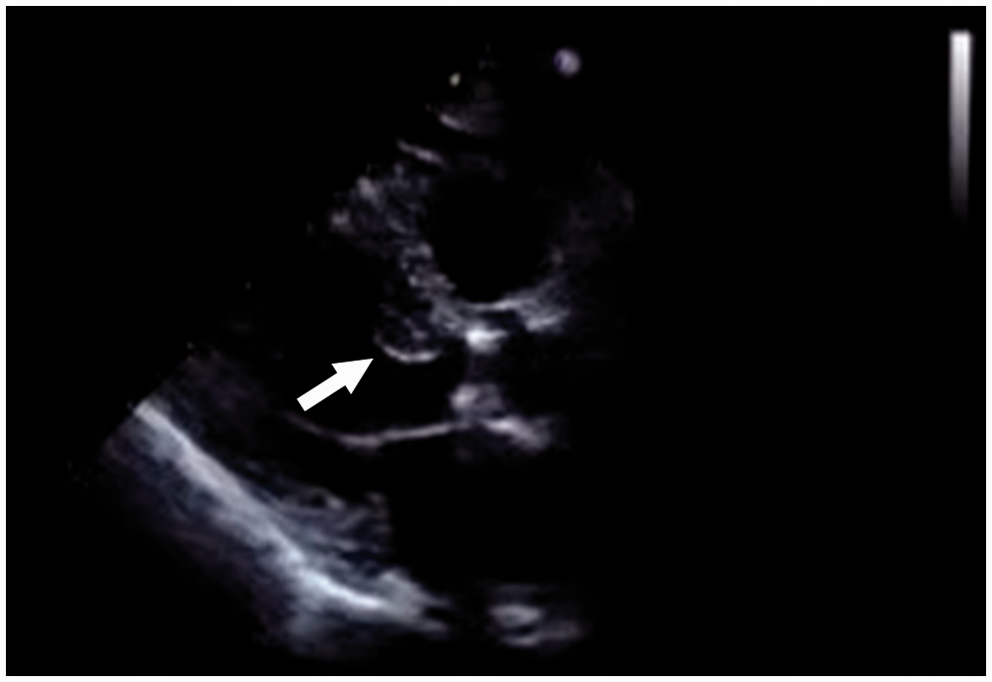
An 82-year-old woman underwent aortic valve replacement with a 17-mm SJM Regent mechanical prosthetic valve (St. Jude Medical, Inc., St. Paul, MN, USA) for aortic stenosis with a small annulus, as well as coronary artery bypass grafting to the right coronary artery. Her postoperative course was uneventful, and patient-prosthesis mismatch was not seen. However, 4 years after the operation, she began to experience hemolysis with consequent anemia which required repeated blood transfusions twice a month. Blood sample data revealed marked hemolytic anemia as indicated by the following values: hemoglobin 7.6 g dL−1; lactic dehydrogenase 1055 U L−1; serum haptoglobin < 10 mg dL−1; and reticulocytes 4.6%. Cineradiography showed restricted opening but not restricted closing of the leaflets, and an open angle limitation at 61° (Figure 1). Echocardiography showed that a sigmoid septum was also causing LVOT obstruction (Figure 2), a maximum pressure gradient of 94 mm Hg, a mean pressure gradient of 51 mm Hg, and a peak stenotic jet velocity of 4.9 m s−1. There was no paravalvular leakage or aortic regurgitation through the mechanical valve. Turbulence of flow with high shear stress forces and abnormal flow jets through the LVOT caused severe hemolytic anemia. The right coronary bypass graft was patent. Redo aortic valve replacement following coronary artery bypass is associated with high risk.
2
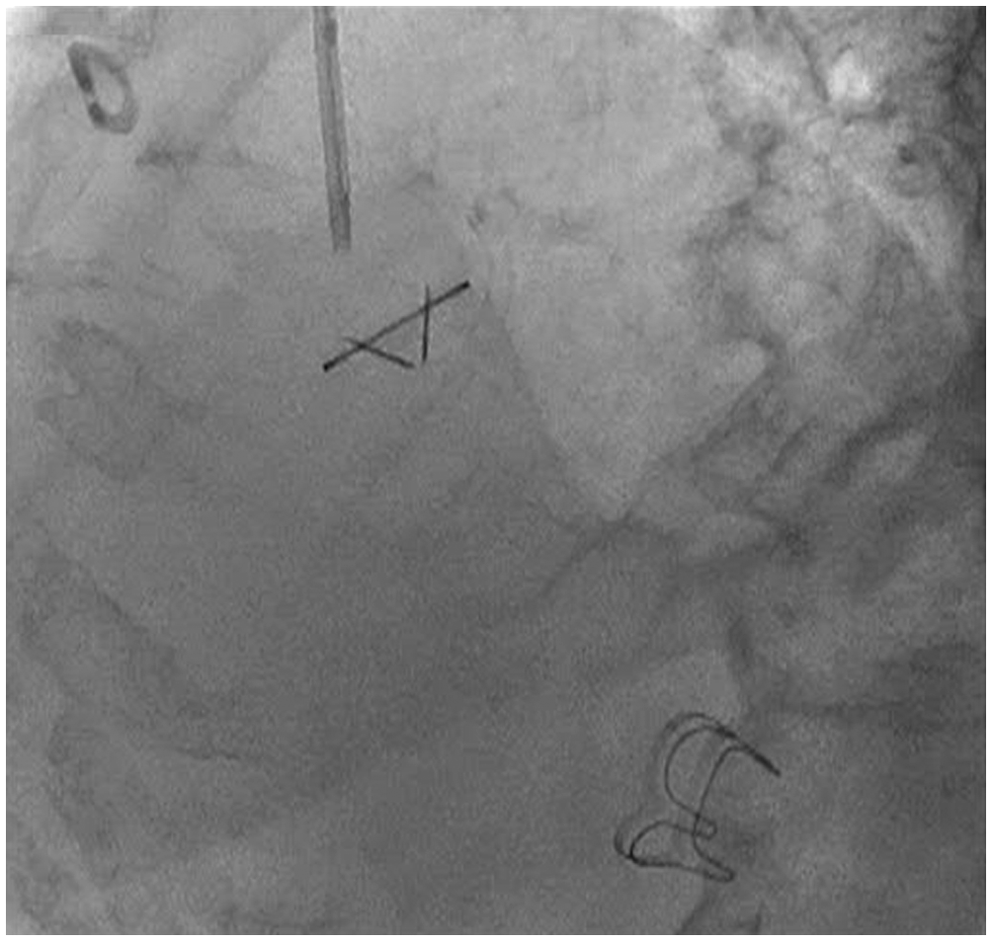
Our patient had a small aortic annulus and previous aortocoronary bypass. Her logistic EuroSCORE was 25.59; therefore, we elected to perform apicoaortic bypass. The chest was opened through a left lateral thoracotomy in the 5th intercostal space. Using a descending thoracic aorta occluding clamp after partial cardiopulmonary bypass, a 22-mm vascular prosthesis (J Graft Shield Neo; Japan Lifeline Co., Ltd., Shinagawa, Tokyo, Japan) was sewn in an end-to-side fashion. Thereafter, total cardiopulmonary bypass was established. Under ventricular fibrillation, the left ventricular apex was excised and a 30-mm-diameter hole was cut into the ventricular cavity. A valved graft using a 19-mm Carpentier-Edwards Perimount Magna bioprosthesis (Edwards Lifesciences LLC, Irvine, CA, USA) and a 22-mm J Graft Shield Neo was inserted. The two grafts were then sewn together. After the operation, biochemical tests were normal. Postoperative echocardiography at 30 days confirmed a maximum pressure gradient of 27 mm Hg, a mean pressure gradient of 13 mm Hg, and peak velocity of the stenotic jet of 2.6 m s−1 at the aortic mechanical valve; the hemodynamic calculations revealed a stroke volume of 78 mL per beat (64 mL per beat through the conduit valve and 14 mL per beat through the mechanical aortic valve). Cineradiography showed an open angle limitation at 71° (Figure 3).
Preoperative cineradiography. (A) Restricted opening of the leaflets and reduced valve orifice area were observed, with an open angle limitation at 61°. (B) Restricted closing of the leaflets was not observed. Transthoracic echocardiography showing that a sigmoid septum caused left ventricular outflow tract obstruction (arrow). Postoperative cineradiography showing an open angle limitation at 71°.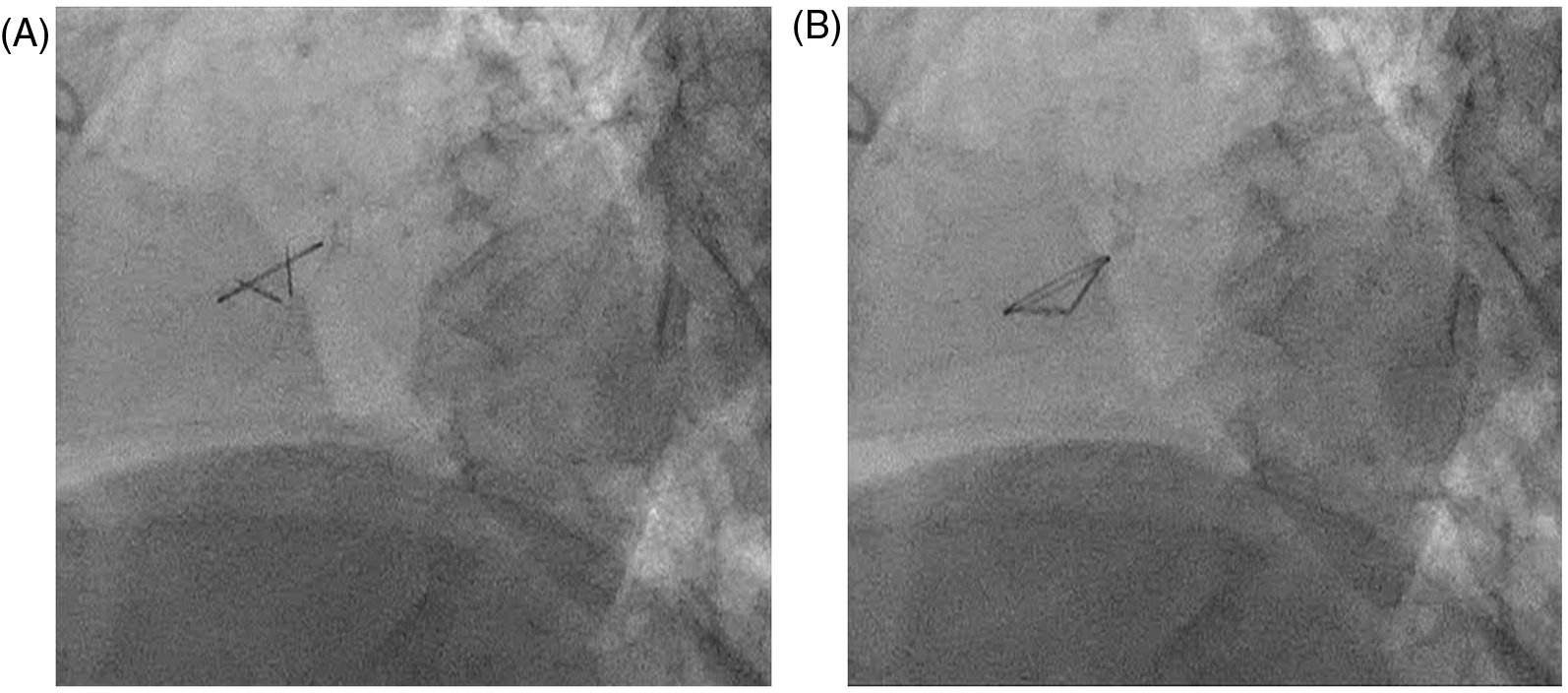
Discussion
Chronic intravascular hemolysis following aortic valve replacement in patients with a mechanical prosthesis is well documented. 3 Severe hemolysis is often associated with valve malfunction or paravalvular leakage. 4 In such cases, repeat replacement of the aortic valve is needed. On the other hand, it is rare to elect apicoaortic bypass because aortic valve regurgitation, like paravalvular leakage and mechanical valve sticking, is contraindicated in the procedure. Skrabal and colleagues 5 described a patient who had undergone 3 previous aortic valve replacements and developed hemolytic anemia due to patient-prosthesis mismatch. Apicoaortic bypass was performed and the patient recovered and remained well after the operation. In our case, the hemolysis was thought to be secondary to aortic prosthetic valve malfunction compounded by subvalvular stenosis. If a new prosthetic valve was to be implanted in the aortic position, resection of the old mechanical valve and also of the subvalvular stenosis would be needed. Furthermore, the patient would be at risk of injury to the right coronary bypass graft. Therefore, we elected to perform apicoaortic bypass. Cooley and colleagues 6 reported creation of double-outlet left ventricles in a number of patients with severe LVOT obstruction. The left lateral transthoracic approach gave direct access to the descending aorta and made the operation less complex in our case. The hemolytic anemia and all hematological alterations improved after the operation. The gradient and the peak velocity over the aortic mechanical valve returned to near-normal values.
In conclusion, using apicoaortic bypass, we successfully treated severe hemolytic anemia resulting from mechanical valve malfunction and subvalvular stenosis. The etiology of the mechanical valve malfunction was unknown. However, apicoaortic bypass can be considered as a valuable treatment in select patients with complex stenosis of the LVOT.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.