
Abstract
Surgical excision of the left atrial appendage is an essential key in the Cox maze IV procedure. Management of very thin, friable, and delicate tissue in the base of the left atrial appendage can be difficult. We have designed a simple method to expose adequately without handling the base of the left atrial appendage. With this technique, the risk of bleeding due to excessive traction or manipulation of the heart is dramatically reduced.
Introduction
Nowadays, atrial fibrillation (AF) is considered a lethal disease because of the incidence of stroke and its devastating consequences. 1 Over 90% of the atrial clots in AF are formed in the left atrial appendage (LAA). 2 Indeed, the LAA has been called “our most lethal and disabling attachment”. 3 The Cox maze procedure has been designed for the surgical treatment of AF. 4 The high success rate of this technique has been attributed not only to eliminating AF but also to the fact that the LAA is excised during this procedure. 5 The controversy over which technique is best to exclude the LAA is in favor of cut-and-sew external excision.6,7 In addition, the electrical isolation of the LAA required in the Cox maze IV with bipolar radiofrequency (RF) cannot be safely achieved by simple ligation or an encircling suture. Therefore, excision of the LAA is a crucial part of the Cox maze procedure. Luxation of the heart is necessary to obtain good visibility of the LAA. One of the biggest challenges has always been management of the very thin friable tissue frequently found in the base of the LAA. We have designed a simple and easy method to expose the base of the LAA without manipulating the heart.
Technique
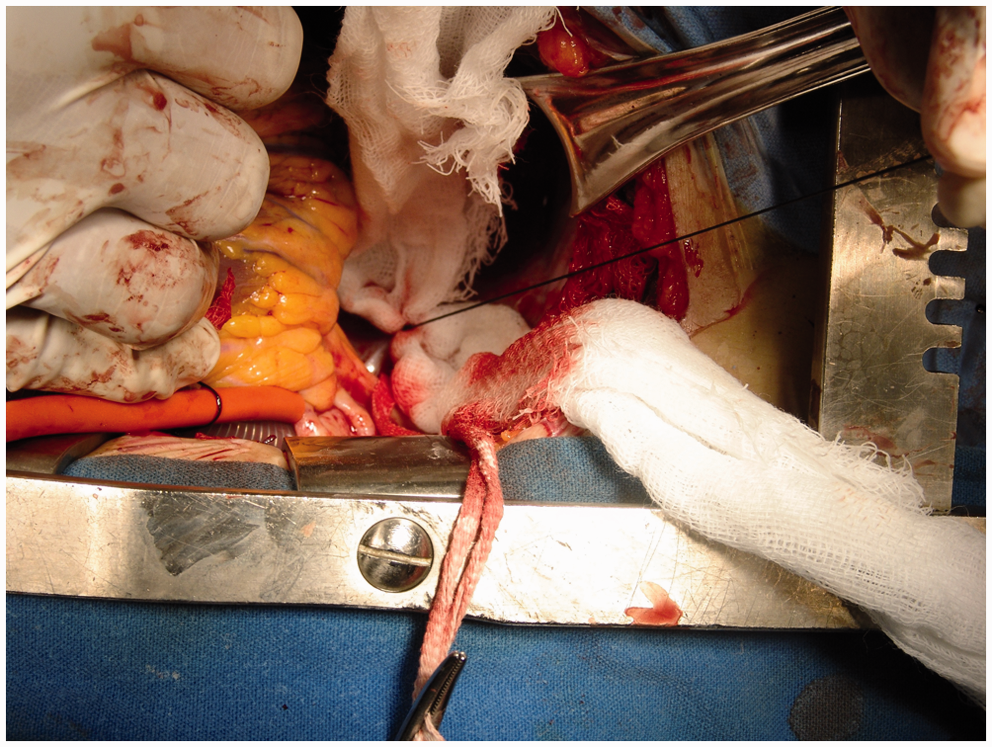
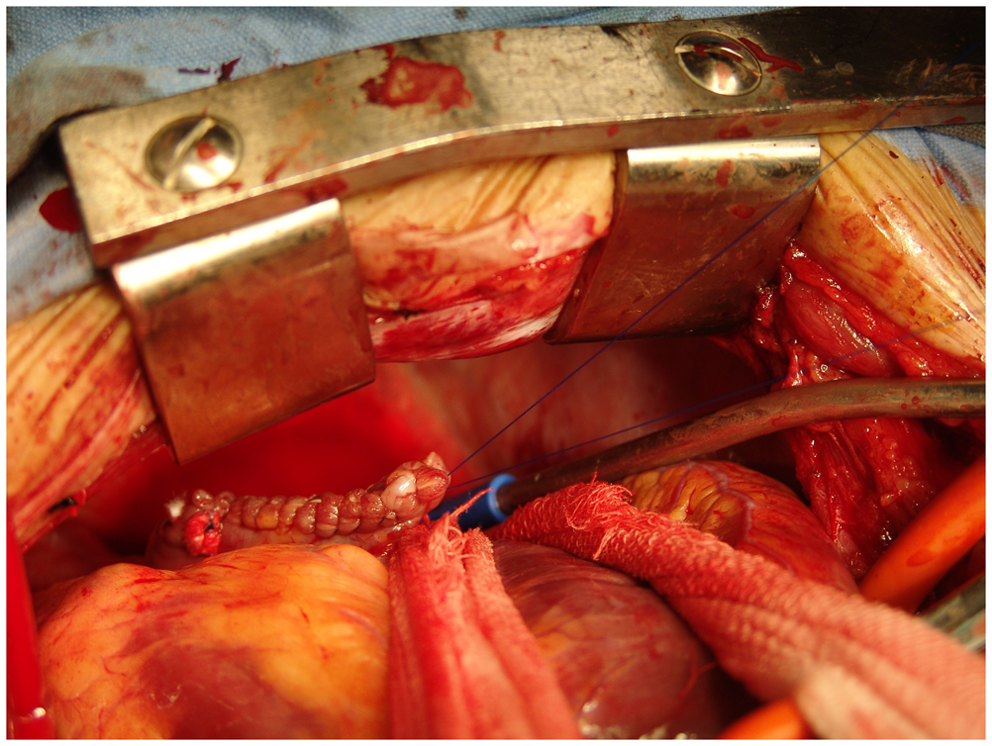
The operation is performed through a median sternotomy. Cardiopulmonary bypass is established with bicaval and ascending aorta cannulation. Once the pulmonary veins have been isolated, the heart is arrested by cold cardioplegia, the left atrium is opened, and the box-lesion set is achieved. To expose the posterior aspect of the pericardium, the heart is completely lifted upwards. A single stitch of 0 silk is placed in the middle portion of the pericardium, between the left inferior pulmonary vein and the inferior vena cava. Care is taken, keeping in mind the structures behind the posterior pericardium (Figure 1). A strip of 5 cm in width is cut from a surgical pad. The middle point of the strip is tied with the above suture (Figure 2). The heart is released and both arms of the strip are passed through the left side of the heart. Tension is placed on the strip toward the right side. Thus a V-shaped band is obtained, allowing excellent exposure of the LAA (Figure 3). The LAA is removed with scissors. An RF burn line is created between the base of the LAA and the left pulmonary veins. The LAA is closed with a 3/0 polypropylene running double layer. The pericardial stitch and the strip are removed. The rest of the operation is performed in the usual way.
A single suture is placed in the posterior pericardium. The strip is tied in the middle of the pericardium. Both ends of the strip are passed to the left side of the heart and pulled up toward the right side. This maneuver exposes the left atrial appendage and left pulmonary veins, without directly manipulating the heart.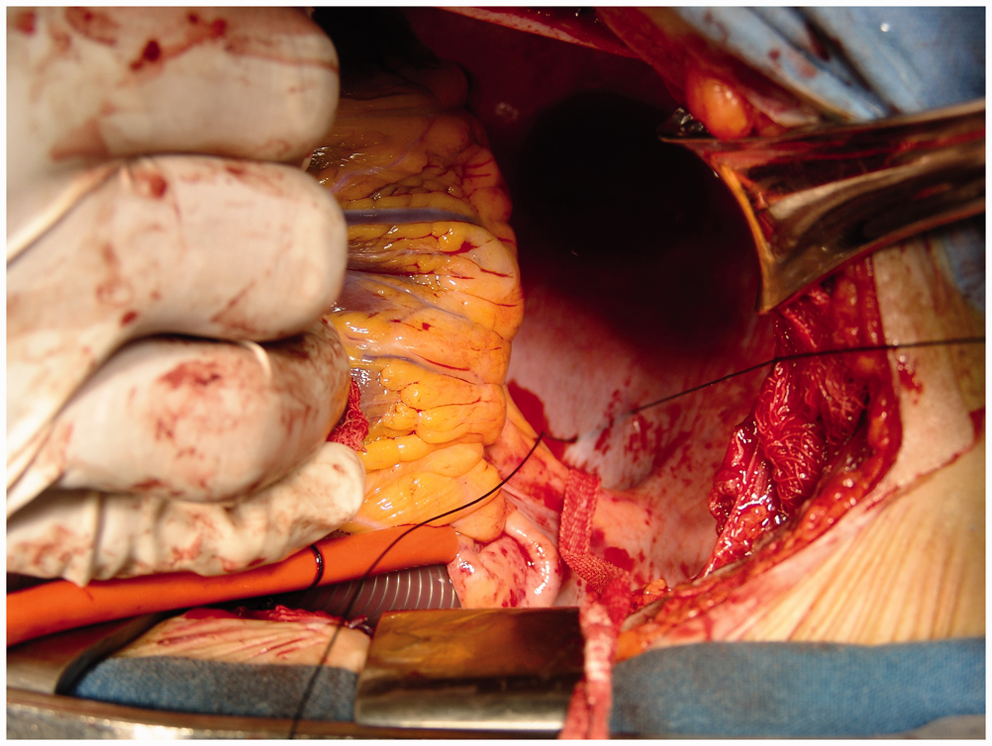
Discussion
Bipolar RF ablation appears more reliable than monopolar RF ablation for creating transmural lesions. 8 Because of its simplicity, the Cox maze IV is preferred by most surgeons. However, exposure of the LAA and left pulmonary veins is a challenge in this technique. This is due to the fact that both the LAA and the left pulmonary veins are addressed from outside the heart. There is a thin fat pad covering the base of the LAA and the adjacent aspect of the left ventricle. Handling of this area of the heart can cause lethal bleeding tears. Exposure of the LAA may be difficult, especially when cardiomegaly is observed. This is particularly true in the case of chronic AF with concomitant mitral valve disease. In such a case, we recommend our technique based on a hands-free method. Specifically, it avoids any additional risk resulting from excessive traction by the hand of the surgical assistant. It is important to close all the incisions very meticulously in this area because it becomes almost inaccessible once the heart is full and beating. We have successfully employed this technique in more than 100 cases, with excellent outcomes. No bleeding of the worked area has been observed.
In conclusion, it is important to emphasize the need to work without handling the heart in this type of surgical procedure. Special care must be taken because of the very friable, delicate, and thin tissue in this area. Excessive traction or manipulation of the heart can result in inaccessible lethal bleeding. Our hands-free technique offers a good alternative for this purpose.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.