
Abstract
Spontaneous haemothorax due to vasculopathy in patients with neurofibromatosis type 1 is rare but life-threatening. A 56-year-old lady with neurofibromatosis type 1 presented with right-sided chest pain, dyspnoea, and collapse. Computed tomography showed a right-sided hemothorax. Urgent angiography showed contrast leakage from a right subclavian artery pseudoaneurysm. A Gore Viabahn endovascular stent graft was deployed. Completion angiography revealed satisfactory haemostasis. She underwent video-assisted thoracoscopic evacuation of the hemothorax, with good results. This case highlights a novel approach to managing a rare emergency, using combined procedures.
Introduction
Neurofibromatosis type 1 (NF-1) is an autosomal-dominant condition characterized by multiple cutaneous neurofibromas and café-au-lait spots.1,2 It was reported that 3.6% of patients with NF-1 have associated vasculopathy which includes stenoses, aneurysms, and arteriovenous malformations. 1 Spontaneous rupture of these vessels is rare but life-threatening. Only 70 cases have been reported in the literature over the past 40 years. 3 Various treatment strategies have been described, including conservative measures such as intercostal drainage, 4 thoracotomy,5,6 interventional radiological procedures such as coil embolization,2,5 and stent graft placement. 3 We describe a case of spontaneous right-sided haemothorax from a pseudoaneurysm of the right subclavian artery in a 56-year-old lady with known NF-1.
Case report
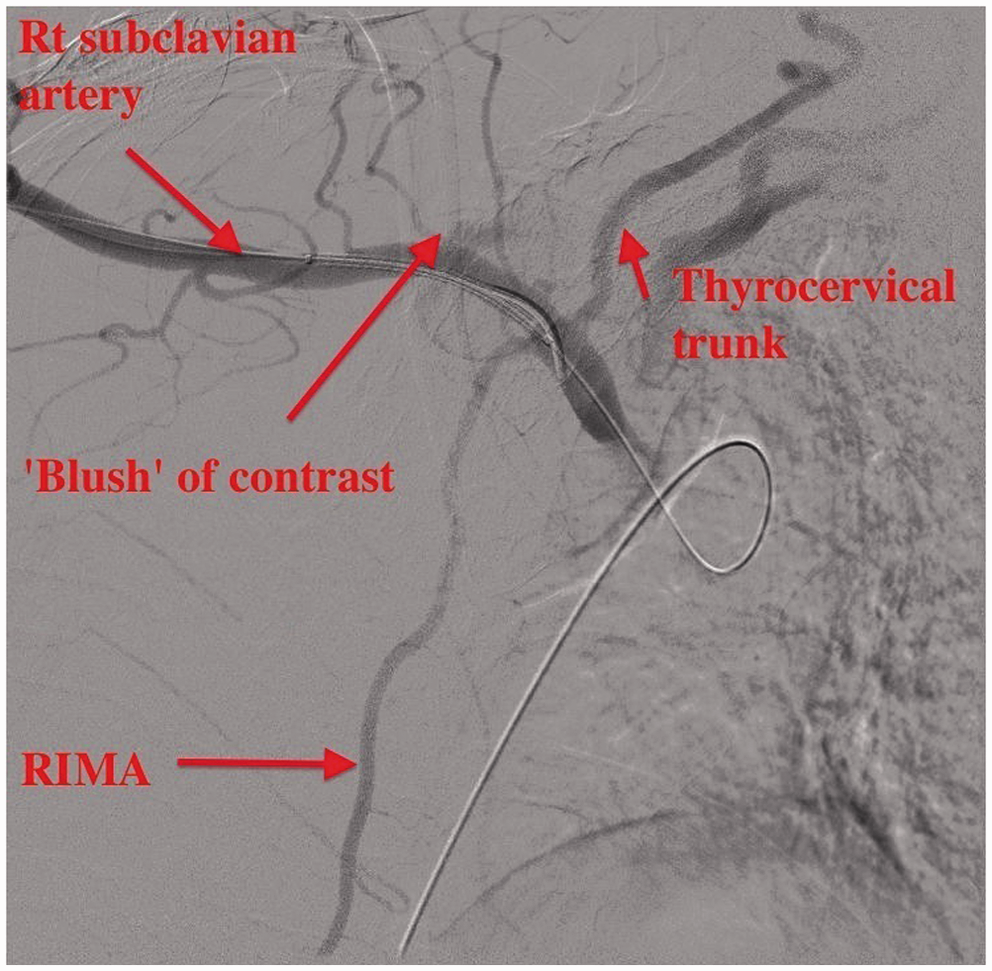
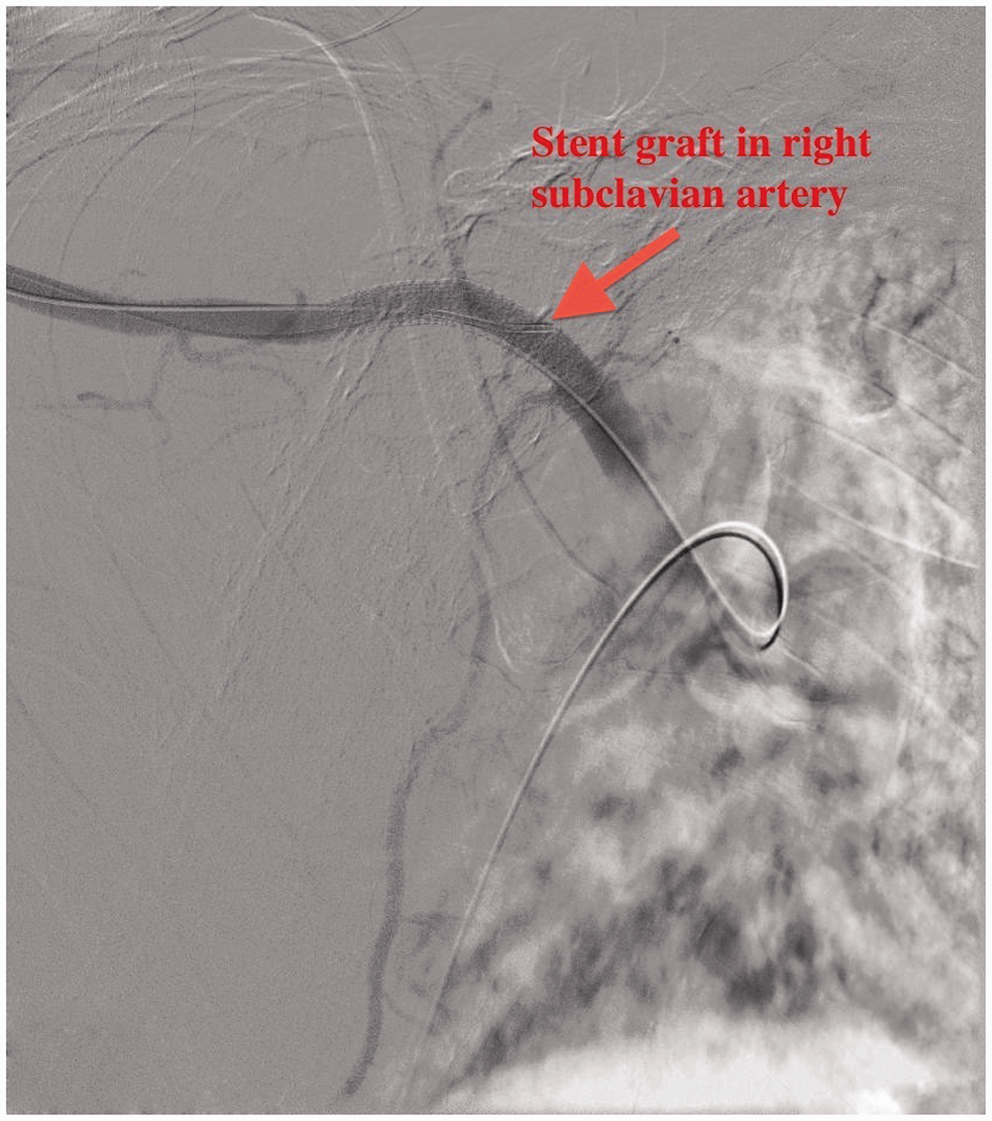
A 56-year-old lady with known history of NF-1 and no significant comorbidities, presented within 12 h of sudden-onset right-sided chest pain, an episode of collapse, and dyspnoea. On arrival, she was found to be anaemic with a hemoglobin level of 5.5 g·dL−1. A chest radiograph showed complete whiteout of her right chest. She was transfused with 2 units of packed red cells and remained haemodynamically stable on 2 L·min−1 of oxygen via nasal cannulae. Right-sided pleural aspiration revealed frank blood. Urgent computed tomography of her chest showed a right-sided haemothorax with almost complete collapse of her right lung. A possible pseudoaneurysm of the right subclavian artery was seen (Figure 1). She was transferred to our department for consideration of emergency surgery. She was haemodynamically stable on arrival, with a pulse rate of 90 beats·min−1 (sinus rhythm), blood pressure of 130/70 mm Hg, and oxygen saturation of 94% on a fraction of inspired oxygen (FiO2) of 0.28. We elected not to perform intercostal chest drainage because we felt that the haemotoma was tamponading any bleeding. A repeat computed tomography scan suggested direct filling of the pseudoaneurysm from the subclavian artery, and an ultrasound scan confirmed arterial phase blood entering the sac. Our interventional radiology team therefore organized urgent angiography with a view to either coil embolization or stent graft placement. The right brachial artery was cannulated using a 4F sheath under ultrasound guidance, while the right common femoral artery was punctured with a 5F sheath. An arch aortogram and selective angiography from the brachial sheath demonstrated a small blush of contrast in the right subclavian artery distal to the origin of the vertebral artery (Figure 2). The 5F sheath in the femoral artery was exchanged for a 9F sheath. Using a Simmons Sidewinder 2 catheter, the right subclavian artery was catheterised, and an exchange wire was passed into the brachial artery. A 0.9 × 5-cm Gore Viabahn stent graft was placed in the right subclavian artery and deployed proximal to the origin of the vertebral artery. Completion angiography showed sealing of the pseudoaneurysm (Figure 3). A post-procedure ultrasound scan confirmed thrombosis of the pseudoaneurysm. The patient was taken to the operating room the next day for a 2-port video-assisted thoracoscopic (VATS) procedure in which 3.2 L of blood and clots were evacuated from her right chest. There was an extrapleural haematoma at the apex of the right chest. This was not explored further because the bleeding had settled. A 32F intercostal drain was inserted in the operating room under direct vision. Serial chest radiographs performed postoperatively revealed an improvement in the right-sided collection, and the patient was discharged home 4 days later.
Computed tomography showing pseudoaneurysm of the right subclavian artery and hemothorax. Blush of contrast from the right subclavian artery. RIMA: right internal mammary artery. Completion angiography showing stent graft in-situ.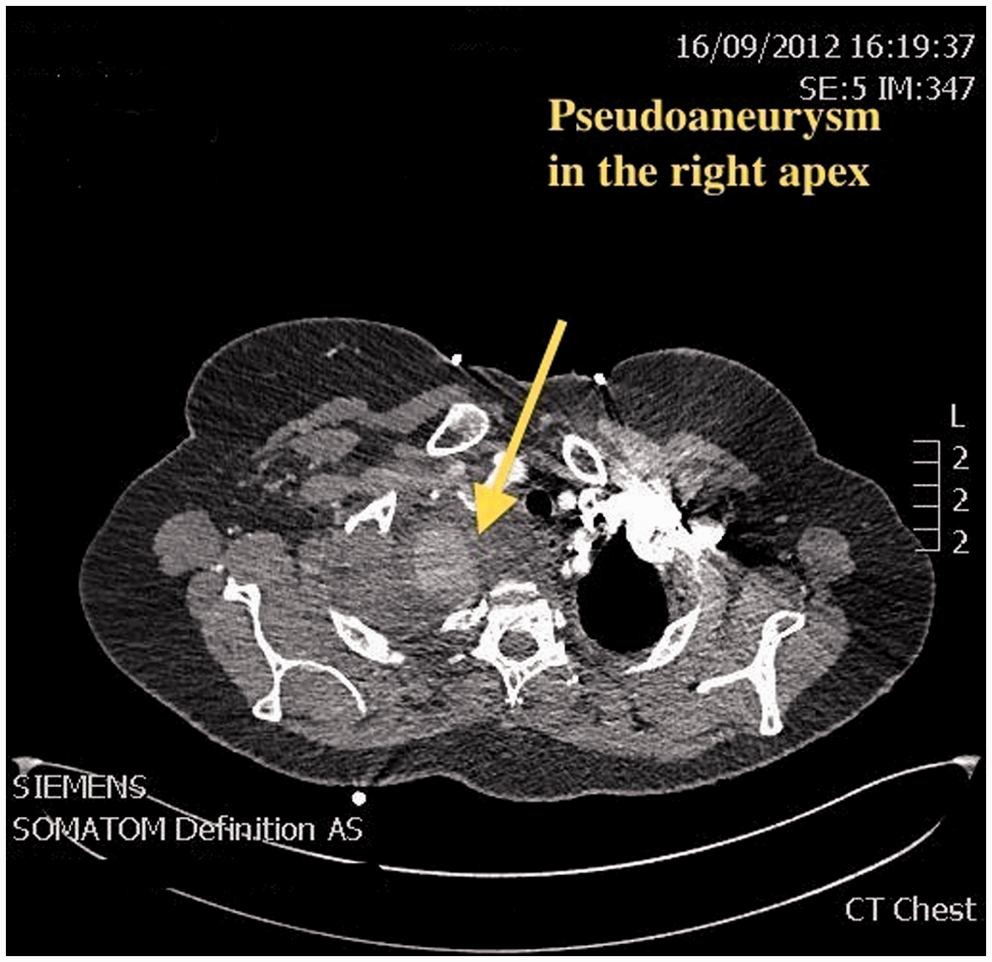
Discussion
Two types of vascular lesions in NF-1 patients have been described, based on the size of the vessel. 6 Smaller vessels (<1 mm in diameter) display dysplastic features, whereas larger vessels lose strength due to neurofibromata invasion of the media and compression of the vasa vasorum, causing ischaemia. 6 The most common vessels involved in the chest include the subclavian, internal mammary, and intercostal arteries. 7 Spontaneous rupture of these aneurysms causing massive haemothorax are rare, dramatic, and life-threatening. Twenty cases have been reported in which the management was conservative treatment (6 cases) or emergency thoracotomy (14 cases). 6
In catastrophic haemorrhage, thoracotomy and ligation of the bleeding vessel is indicated. Nine of 14 cases that required an emergency thoracotomy, survived (mortality rate of 40%).4,6 Repair of the fragile vessel may be complex and often, the only surgical options are ligation, bypass, or replacement of the affected vessel.2,6 Of the other 6 patients, 3 were treated conservatively (with 1 death) and the other 3 were diagnosed at autopsy. 6 Successful treatment of arterial rupture using endovascular techniques has been reported. These methods include coil embolization and stent graft placement.2,3 If preservation of arterial flow is not needed, then coil embolization is popular, safe, and less invasive. 2 Six of 7 patients who underwent coil embolization were successfully discharged. 2 A covered stent graft is required if preservation of arterial flow is crucial. This procedure is more complex and requires more time for planning and preparation. 2 Only 2 cases have been reported in which stent grafts were successfully used to seal subclavian artery bleeding in NF-1; Santin and colleagues 3 followed their procedure by chest drain insertion on the table.
In patients who are hemodynamically stable, it may be prudent to initially perform endovascular procedures such as coil embolization or stent graft insertion to seal the leak. However, in a small number of cases, fatal re-bleeding following endovascular procedures have been reported.2,5 Once the bleeding is controlled, a VATS procedure can be performed to evacuate the haemothorax, with the option of proceeding to open surgical ligation if necessary. In this patient, we felt that inserting a chest drain prior to definitive management could potentially cause exsanguination because the haemothorax was helping to tamponade further bleeding. In conclusion, prompt diagnosis of this rare problem is crucial. Patients who present in hypovolaemic shock should undergo an emergency thoracotomy. For those who present with stable haemodynamics, a conservative two-staged approach using endovascular techniques followed by surgery may be preferred.
Footnotes
Acknowledgments
The authors would like to acknowledge the clinical help and expertise of Dr. Simon Travis, Consultant Interventional Radiologist, Nottingham City Hospital, and Dr. Mark Roberts, Consultant Respiratory Physician, King’s Mill Hospital, Mansfield, UK.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.