
Abstract
Patients with a right aortic arch frequently develop an aneurysm at the origin of the left subclavian artery, called Kommerell’s diverticulum; it is a remnant of the left fourth aortic arch. These variants may occur in combination with congenital heart defects or they may be isolated. We report an extremely rare case of symptomatic stenotic origin of an aberrant left subclavian artery arising from a Kommerell’s diverticulum in a 39-year-old man with right-sided aortic arch who had left upper limb pain and numbness on exercise. He was successfully treated by percutaneous angioplasty and primary stent implantation.
Introduction
Right-sided aortic arch is an anatomic variant occurring in approximately 0.04%–0.1% of the population, and half of these patients also have an aberrant left subclavian artery. 1 Patients with a right aortic arch frequently develop an aneurysm at the origin of the left subclavian artery. This is called a Kommerell’s diverticulum and it is a remnant of the left fourth aortic arch. This was originally described by Kommerell in a patient who had a left aortic arch and an aberrant right subclavian artery in 1936. 2 This variant, also known as (aberrant) arteria lusoria aneurysm, may occur in combination with congenital heart defects or it may be isolated. We report an extremely rare case of symptomatic stenotic origin of an aberrant left subclavian artery arising from a Kommerell’s diverticulum in a 39-year-old man with right-sided aortic arch.
Case report
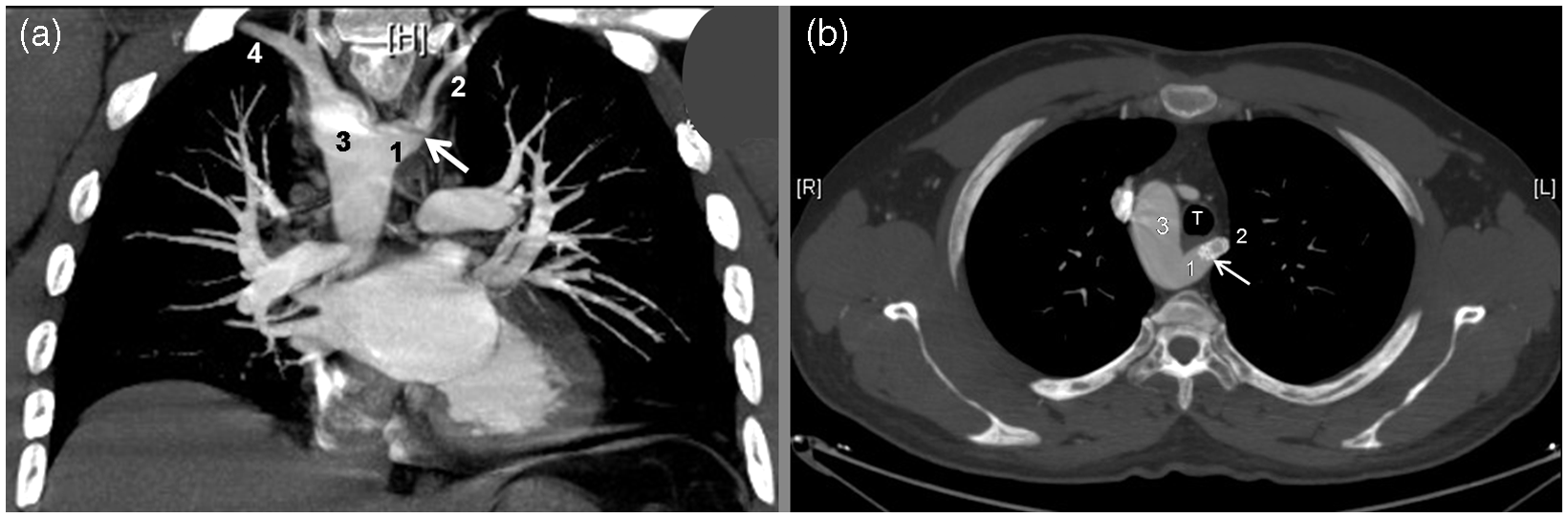
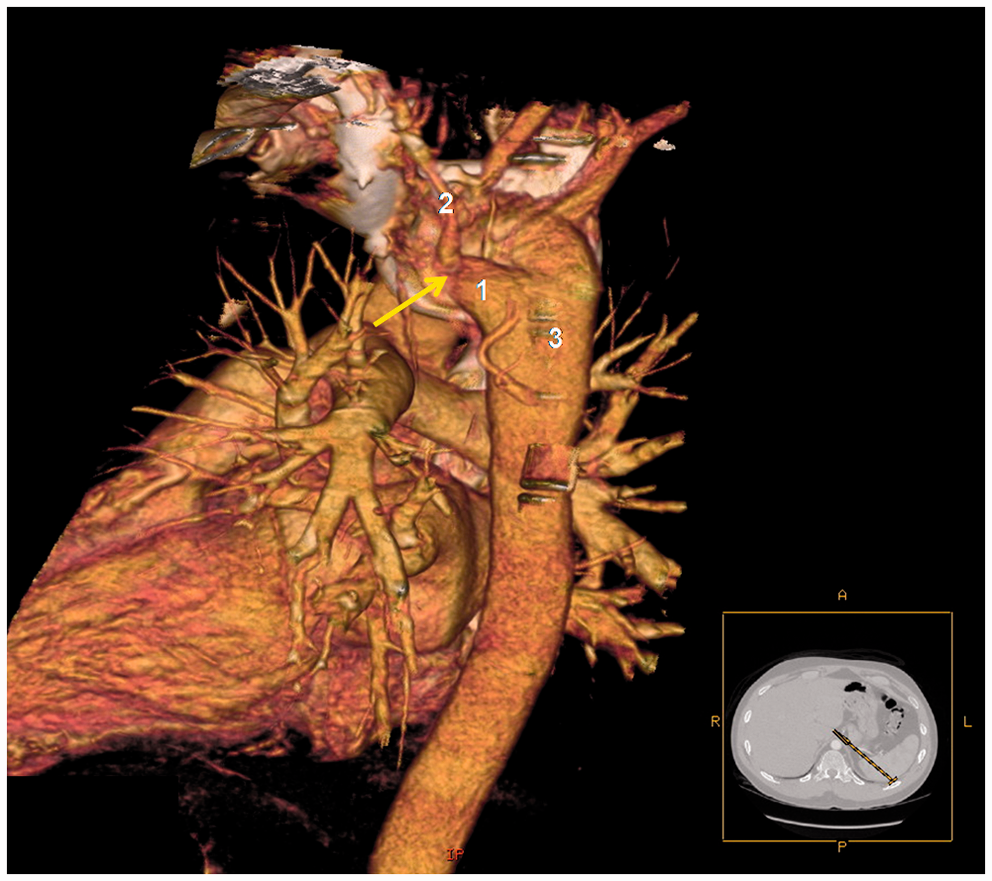
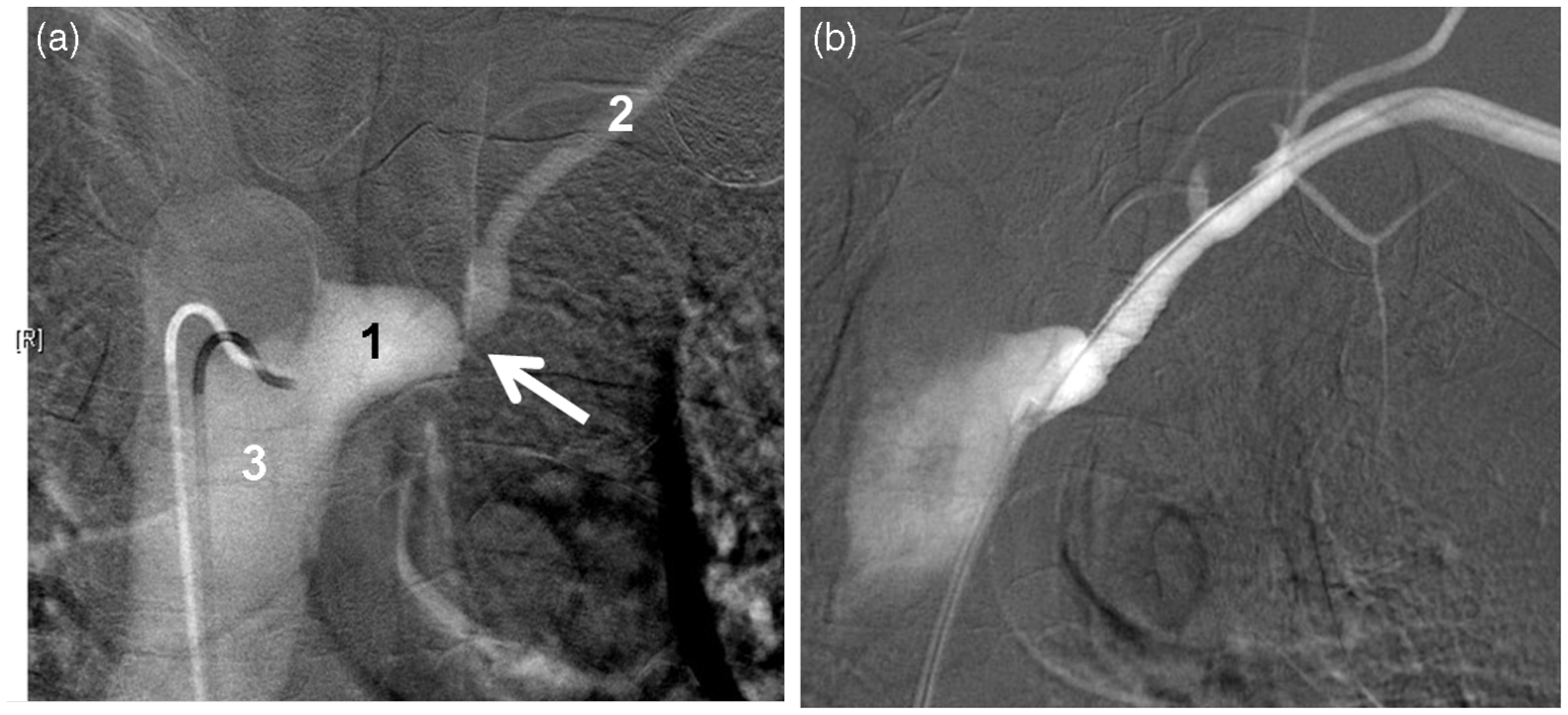
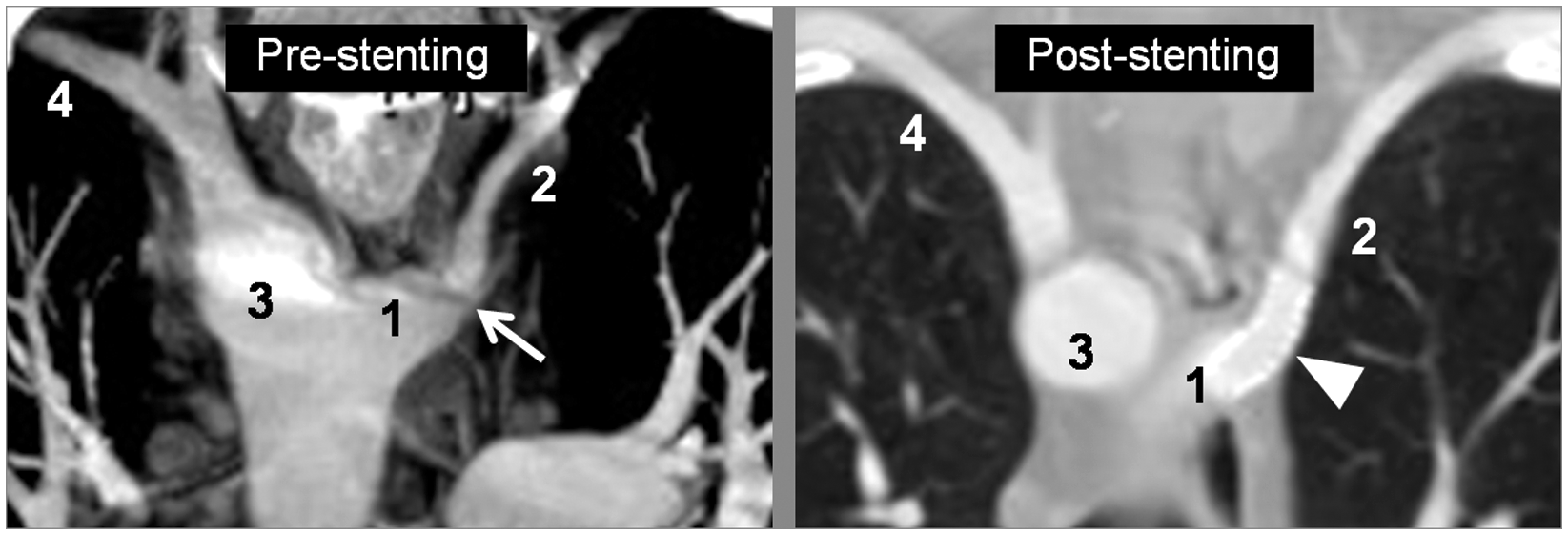
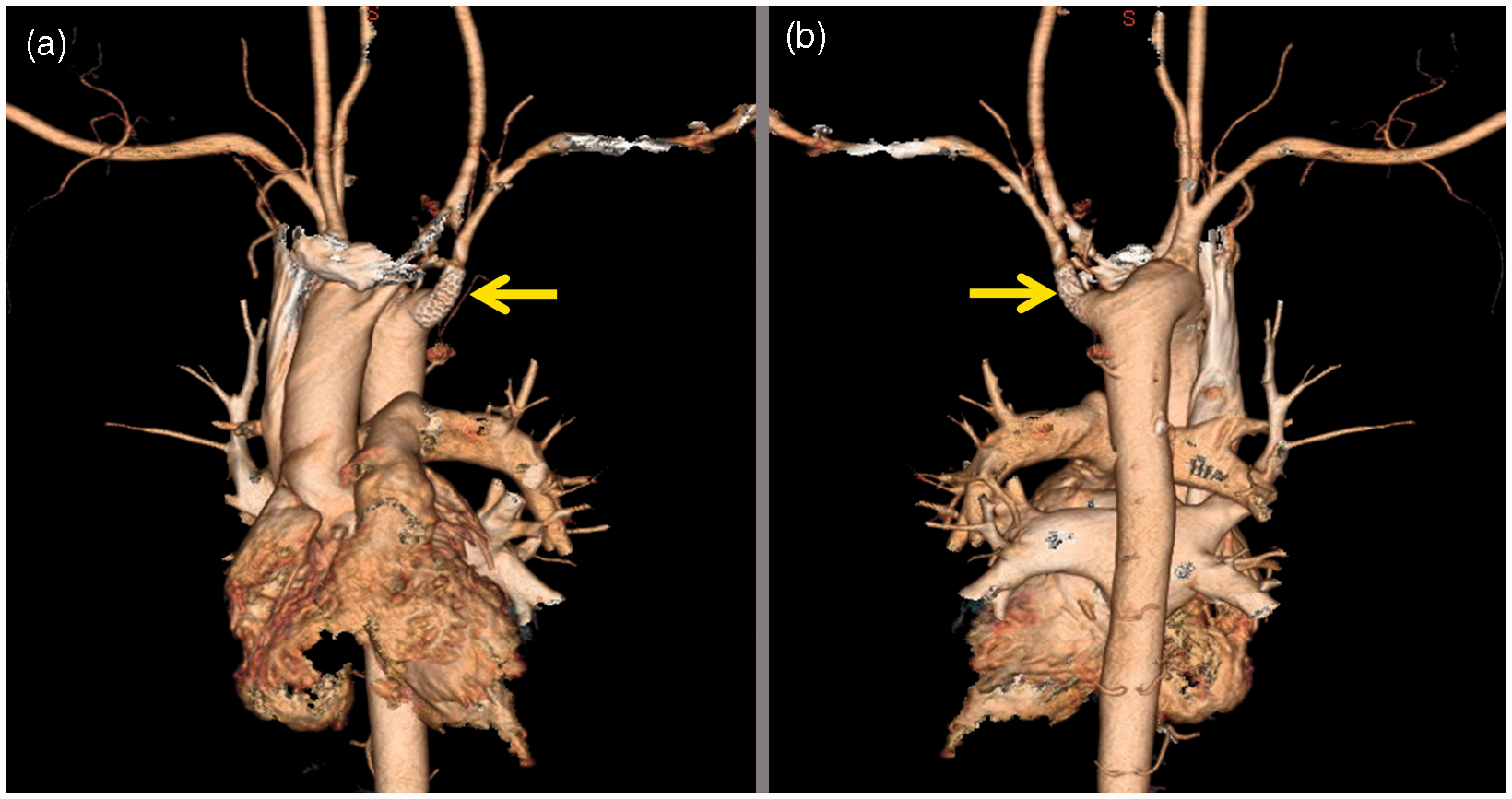
A 39-year-old man was referred to the vascular surgery clinic with exercise-induced left upper limb pain and numbness of more than 20 years duration, which became worse over the previous two weeks. He gave no history of fever, dysphagia, dyspnea, cough, or wheezing. On physical examination, his breathing was smooth. No edema of the head and neck areas was noted. His blood pressure was 142/92 mm Hg in the right arm and 102/71 mm Hg in the left, with slightly decreased left radial and brachial pulses. The left upper limb had no signs of ischemia. Chest radiography showed a right-sided aorta (Figure 1). Chest computed tomography in both coronal and cross-sectional views showed a right aortic arch with an aberrant left subclavian artery arising from a retroesophageal Kommerell’s diverticulum, with focal luminal narrowing at the origin of the aberrant left subclavian artery (Figure 2). The aberrant left subclavian artery was smaller than the right subclavian artery. On chest computed tomographic angiography in posterior view (Figure 3), the flow stream of the diverticulum could be traced. The Kommerell’s diverticulum arose from the right aortic arch and drained into the aberrant left subclavian artery which had focal luminal narrowing at its origin. An aortic angiogram performed via a right femoral approach using a 5F diagnostic catheter (SIM 1; Cordis, Bridgewater, NJ, USA) and a standard 0.035” guide wire, confirmed the diagnosis of a congenital variation of the vasculature with severe narrowing of the origin of the aberrant left subclavian artery (Figure 4a) as the cause of the patient’s symptoms. He underwent percutaneous 7 × 29-mm stent implantation (Genesis; Cordis, Bridgewater, NJ, USA) to the narrowed segment of the aberrant left subclavian artery (Figure 4b), using a 6F guiding catheter (Guider Soft Tip; Boston Scientific, Natick, MA, USA) and the standard 0.035” guide wire. The patient’s symptoms improved and he was discharged on aspirin (81 mg once daily) and clopidogrel (75 mg once daily). Follow-up chest computed tomographic angiography after 3 months showed normal caliber of the left subclavian artery, measuring 11.5 mm in diameter, with no evidence of aneurysmal dilatation (Figures 5 and 6).
Chest radiograph showing a right-sided aorta (white arrows), an aortic knob on the right (white arrowheads), and the trachea displaced toward the left (black arrowhead). (a, b) Computed tomographic scan of the chest showing the Kommerell’s diverticulum (1) at the base of aberrant left subclavian artery (2), which is smaller than the right subclavian artery (4), a right-sided aortic arch (3), the trachea (T), and focal luminal narrowing at the origin of the left subclavian artery (arrow). Computed tomographic angiography of the chest showing the Kommerell’s diverticulum (1) at the base of the aberrant left subclavian artery (2), which has focal luminal narrowing at its origin (arrow), and a right-sided aortic arch. Aortic angiograms: (a) pre-stenting showing the Kommerell’s diverticulum (1) at the base of aberrant left subclavian artery (2) which has severe focal luminal narrowing at its origin (arrow), and a right-sided aortic arch (3); (b) Post-stenting. Pre- and post-stenting computed tomographic scans of the chest showing the Kommerell’s diverticulum (1), aberrant left subclavian artery with (2) focal luminal narrowing at its origin (arrow), the stent in situ (arrowhead), a right-sided aortic arch (3), and the right subclavian artery (4). (a) Anterior and (b) posterior post-stenting computed tomographic angiography of the chest showing the stent in situ (arrow).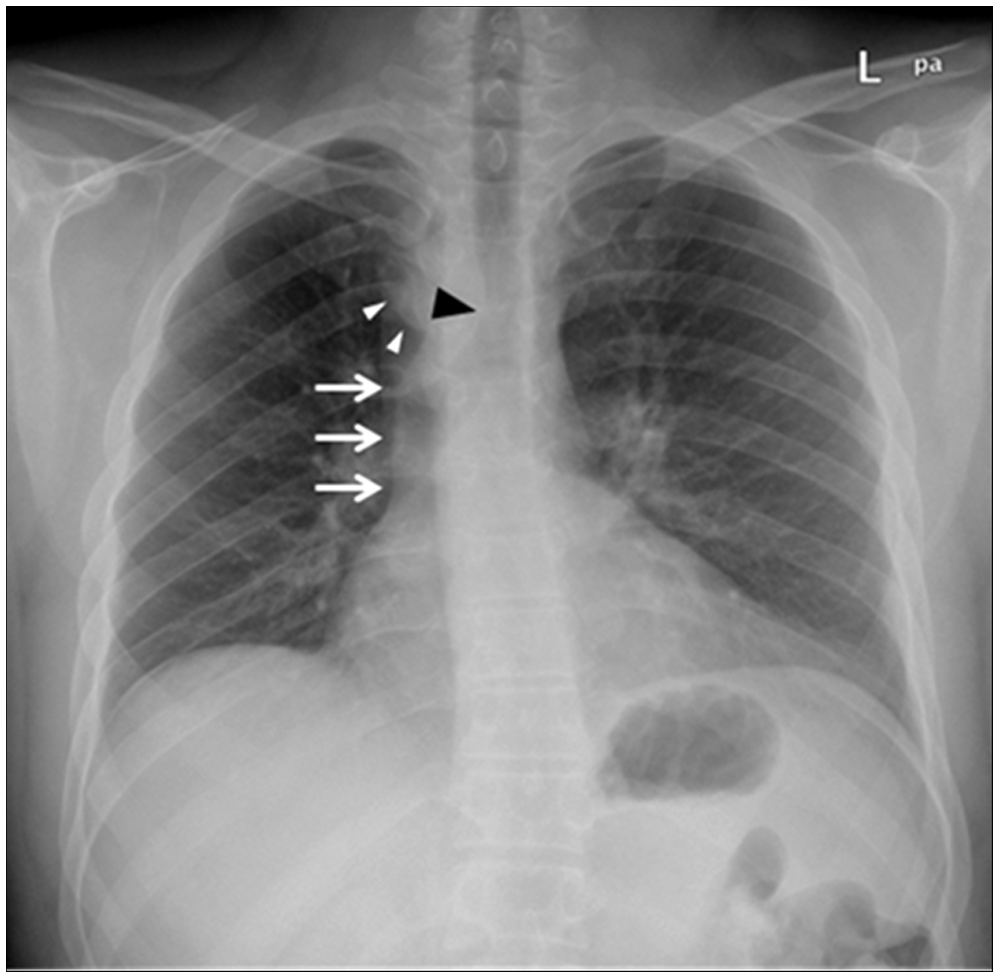
Discussion
Left aberrant subclavian artery is a rare anatomic anomaly that originates from a right-sided aortic arch, crosses the posterior part of the mediastinum, and drains into the left upper limb. Right-sided aorta is present in 0.04% to 0.1% of the population, and 50% of right-sided aortic arches are associated with an aberrant left subclavian artery. 1 Right-sided aortic arch with aberrant origin of the left subclavian artery is caused by involution of the left fourth aortic arch with concomitant persistence of the right fourth aortic arch which is interrupted between the left common carotid and left subclavian arteries. 3 Patients with a right aortic arch and left ligamentum arteriosum frequently develop an aneurysm at the origin of the left subclavian artery. This is a remnant of the left fourth aortic arch. 4 It is called Kommerell’s diverticulum, named after Burckhard Friedrich Kommerell who demonstrated this diverticulum by barium swallow examination in a patient with left aortic arch and aberrant right subclavian artery in 1936. 2
Kommerell’s diverticulum and aberrant subclavian artery may be discovered incidentally in asymptomatic children or adults, but it is sometimes associated with complications such as compression of adjacent structures, dissection, or rupture. The aneurysmal diverticulum in most cases passes through the retroesophageal space, causing dysphagia, dyspnea, stridor wheezing, cough, recurrent pneumonia, obstructive emphysema, or chest pain by structure compression. Compression of the esophagus may cause dysphagia, termed dysphagia lusoria, and compression of the recurrent laryngeal nerve which causes nerve palsy and hoarseness and is known as Ortner syndrome.5,6 Dissection and rupture of an aberrant artery and Kommerell’s diverticulum have been reported in 20% to 50% of patients. 1
Stenosis at the origin of an aberrant left subclavian artery arising from a Kommerell’s diverticulum with a right-sided aortic arch is extremely rare. Previously, an incidental finding of this anomaly was reported in an asymptomatic 80-year-old man. 7 Also, the prenatal ultrasound appearance of a congenital critical stenosis of an aberrant left subclavian artery in a newborn has been reported. 8 This is the first reported case of symptomatic stenotic origin of an aberrant left subclavian artery arising from a Kommerell’s diverticulum in a patient with a right-sided aortic arch, which was successfully treated by percutaneous stent implantation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared