
Abstract
The incidence of aortoesophageal fistula after thoracic endovascular aortic repair has increased following an increase in thoracic endovascular aortic procedures. A 68-year-old man was diagnosed with aortoesophageal fistula 6 years after thoracic endovascular aortic repair of a descending aortic aneurysm. Due to massive hematemesis and instability, he underwent a left thoracotomy, graft repair of the aorta with stent removal, gastrostomy, and proximal esophagostomy. Unfortunately, he died 1 week later due to sepsis. Aortoesophageal fistula may present long after thoracic endovascular aortic repair, and clinicians treating such cases should always be aware of this complication.
Introduction
Thoracic endovascular aneurysm repair (TEVAR) is a first-line treatment for aortic pathologies.1,2 Despite its wide application, complications are not yet well defined, especially the long-term complications. One such adverse outcome is the development of aortoesophageal fistula (AEF). The incidence of this complication seems to have been appreciated only recently. 3 We describe a case of AEF that developed long after TEVAR.
Case report
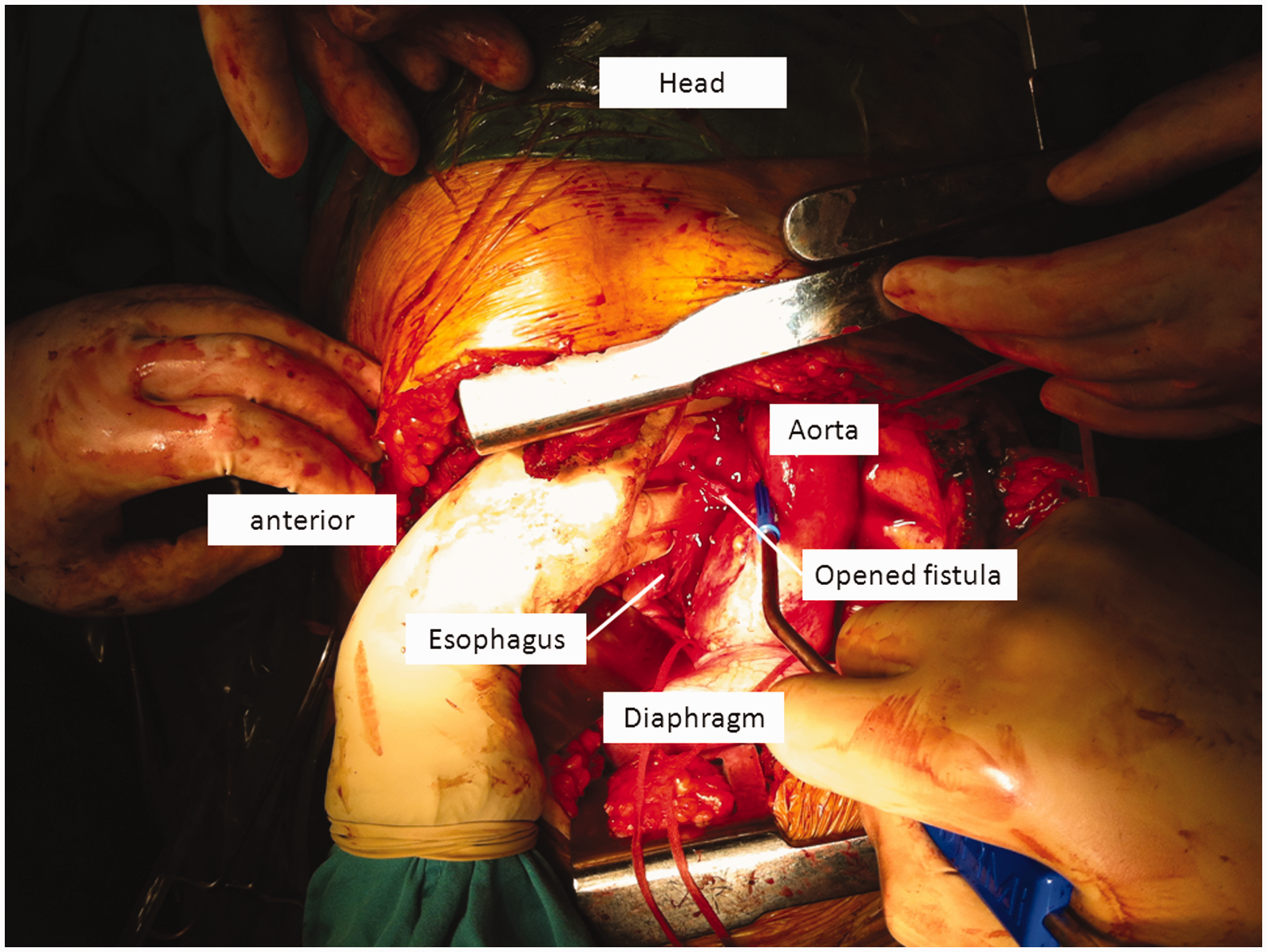
A 68-year-old man presented with hematemesis and fever (39℃). His past medical history was of no significance apart from an episode of collapse 6 years earlier, for which he was admitted to another hospital where a descending aortic aneurysm was diagnosed and treated with TEVAR (Medtronic Talent stent graft). During that admission, he had a fever that was not taken into consideration by the treating physicians. His heart rate was 110 beats·min−1, blood pressure was 90/60 mm Hg, and laboratory tests showed hemoglobin 7.8 g·dL−1, white blood cells 18,000/mm3, and C-reactive protein 32 mg·dL−1. Computed tomography angiography showed an area of increased contrast at the outer rim of the grafted descending aorta towards periesophageal inflammatory tissue (Figure 1). Esophagoscopy and gastroscopy identified a small hole in the middle esophagus, filled with clots and surrounded by inflammatory tissue. The patient was transfused and started on antibiotics (vancomycin 1 g, tazobactam 450 mg, daptomycin 500 mg). An AEF was suspected, and the decision was made to insert a tailored stent-to-stent graft with a plan to perform definitive surgical reconstruction later. However, the patient deteriorated and thus was subjected to surgery. A left thoracotomy was performed. The descending aortic aneurysm was stiffly attached to inflammatory tissue. Dissection towards the arch was easy, whereas dissection towards the diaphragm was difficult because of fibrosis of the peri-aneurysmal tissue. An attempt to separate the aneurysm from the rest of the tissue and the esophageus resulted in opening of the fistula and significant bleeding (Figure 2). A hole was spotted in the upper covered part of the graft, close to the border of the uncovered portion. Femorofemoral cardiopulmonary bypass was established and the heart was arrested at 22℃. The aorta was reconstructed with a 30-mm straight graft. The esophageus was brought to the upper chest and the esophageal fistula was closed. The distal esophageus was stapled and a gastrostomy was performed separately. The patient was transferred to the cardiac intensive care unit. He died on the 7th postoperative day from sepsis.
Computed tomography showing an area of increased contrast towards the periesophageal inflammatory esophageal wall. Dissection of the esophageus near the inflamed aortic aneurysm resulted in opening of the fistula and serious bleeding.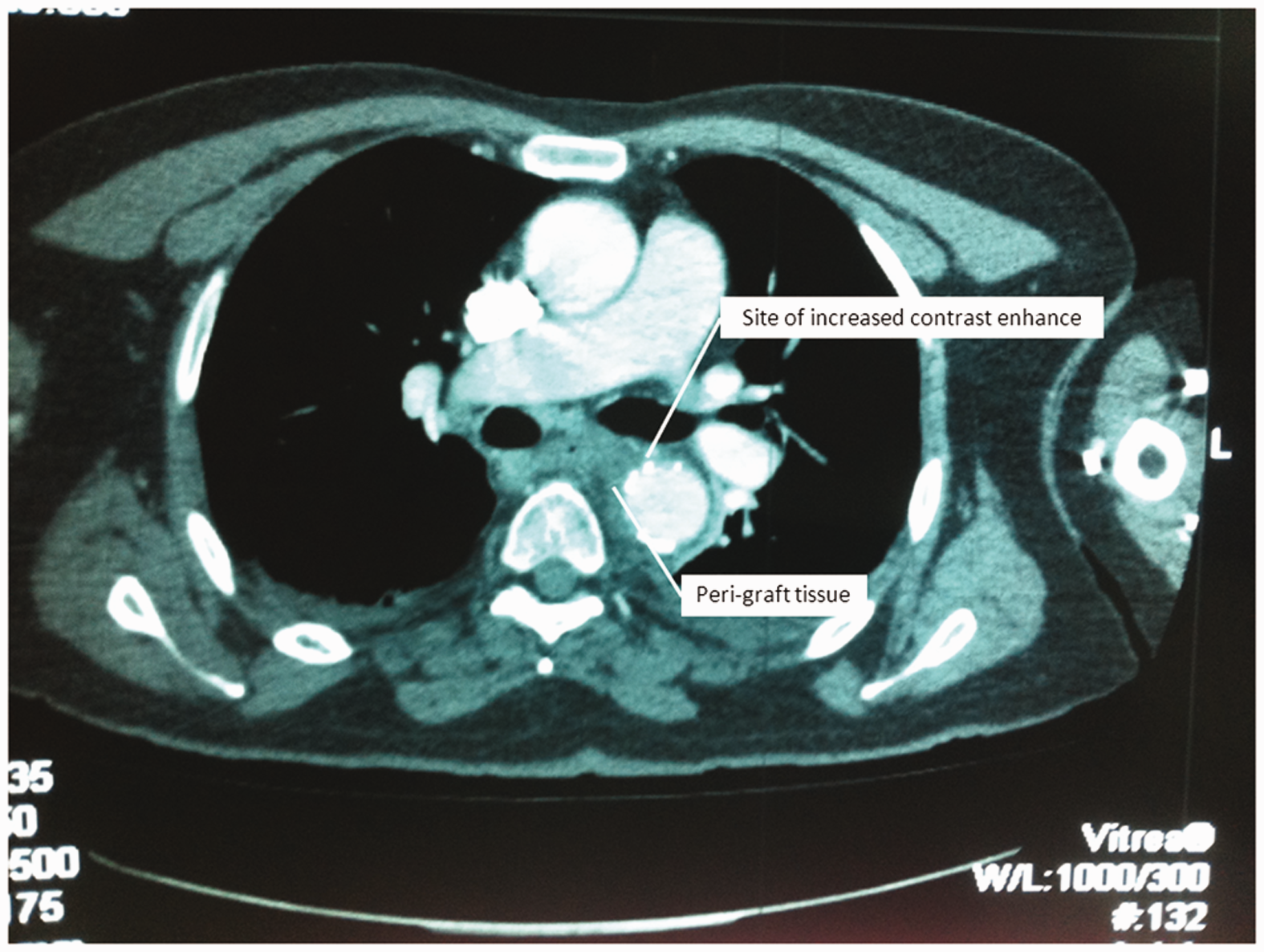
Discussion
The implementation of stenting for treatment of aortic pathologies has given rise to new complications such as the development of AEF.1–3 AEF usually presents early after TEVAR, typically within months.1,4,5 In our case, the patient presented with AEF almost 6 years after TEVAR, which seems to be uncommon in the literature.1–6 The incidence of AEF after TEVAR has been increasing. Until 2009, less than 10 cases had been reported, but many more have been reported thereafter.2,4 The incidence ranges from 0.5%–1.7%. 1 This indicates that AEF represents a considerable complication of TEVAR. The cause of AEF development after stenting is unknown. One possibility is infection of the stent which then perforates into the esophagus wall. 3 The incidence of peri-graft infection is reported to be as high as 0.5%–5%. 1 Risk factors have been recognized to include immunosuppression, diabetes mellitus, chronic renal failure, cancer, wound infections, or the TEVAR itself. An infectious incident may initiate peri-graft infection. 1 The interaction of the radial force of the implanted stent alongside the fragility of the aortic wall at the landing zone needs to be considered in every case of TEVAR. 7
A treatment consensus for AEF, especially after previous TEVAR, has not been agreed upon. However, the outcome is poor; only 37 cases among those published up to 2008 seem to have survived, possibly due to the poor condition of such patients.2–4 However, most reports seem to agree that only an aggressive surgical approach will resolve the issue of esophageal and aortic leaks.2–4,8 The insertion of a new aortic stent to temporarily seal off the fistula provides the time needed to stabilize and prepare the patient for planned surgery.1,2,8 This approach offers the advantage of easier dissection of the peri-graft tissues. Consequently, excessive bleeding might be avoided and better intraoperative conditions achieved. AEF can present long after TEVAR, and a history of TEVAR should always alert clinicians treating such patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.