
Abstract
A totally calcified ascending aorta prevents aortic crossclamping and aortotomy during aortic valve replacement, and replacement of the ascending aorta is a valid option in these cases. We describe a simple technique for calcified ascending aorta replacement using the Cavitron Ultrasonic Surgical Aspirator. This can be used in aortic endarterectomy for removal of the calcified plaque in the anastomotic part.
Keywords
Introduction
A heavily calcified porcelain aorta is associated with increased morbidity and mortality during aortic valve replacement (AVR) because of the increased risk of intraoperative atheroembolism and dissection. A totally calcified ascending aorta prevents aortic crossclamping and aortotomy, and replacement of the ascending aorta is a valid option in these cases. In this report, we describe an ascending aortic replacement technique using the Cavitron Ultrasonic Surgical Aspirator (CUSA Excel+; Integra LifeSciences Corporation, Plainsboro, NJ, USA) in aortic endarterectomy for removal of the calcified plaque in the anastomotic part.
Technique
Cardiopulmonary bypass is commenced with a delivery cannula placed in the right axillary artery. The patient’s body temperature is lowered to an esophageal temperature of 20℃. An initial aortotomy is made and unilateral cerebral perfusion is added via the right axillary artery by crossclamping the proximal innominate artery during circulatory arrest. The ascending aorta is transected 1 cm above the level of the sinotubular junction, and subsequently transected 1 cm below the level of the innominate artery. Antegrade blood cardioplegia is selectively delivered to obtain cardiac arrest. A localized endarterectomy of the distal anastomosis site (circumference of the aortic edge, 1-cm wide) is performed using a CUSA. The CUSA is used on the intima to break up and remove all major calcified deposits. Close attention must be paid to keep the adventitia intact, and the adequacy of decalcification is determined by palpation. A woven Dacron graft (Triplex; Terumo Corporation, Tokyo, Japan) is implanted at the open distal anastomosis (Figure 1). The distal end of the ascending aorta is wrapped with a 1-cm-wide felt strip. The graft is sutured to the distal end of the ascending aorta with 3/0 polyfilament braided sutures, using a horizontal mattress stitch. The distal end of the Dacron graft (1 cm in length) is fixed in an everted position. After completion of the distal anastomosis, the graft is crossclamped and antegrade systemic perfusion is started via the right axillary artery. After positioning the prosthetic aortic valve, proximal anastomosis of the ascending aorta is performed in the same manner as the distal anastomosis. After removal of the aortic clamp, the distal and proximal anastomoses are reinforced with additional 4/0 polypropylene over-and-over sutures.
Schema of the procedure. (a) Endarterectomy of the aortic edge is performed using an ultrasonic surgical aspirator, (b) A Dacron graft edge is everted and inserted into the aorta, and the graft is sewn to the distal end of the ascending aorta with 3/0 polyfilament braided sutures in horizontal mattress fashion, and (c) The anastomosis is reinforced with 4/0 polypropylene over-and-over sutures.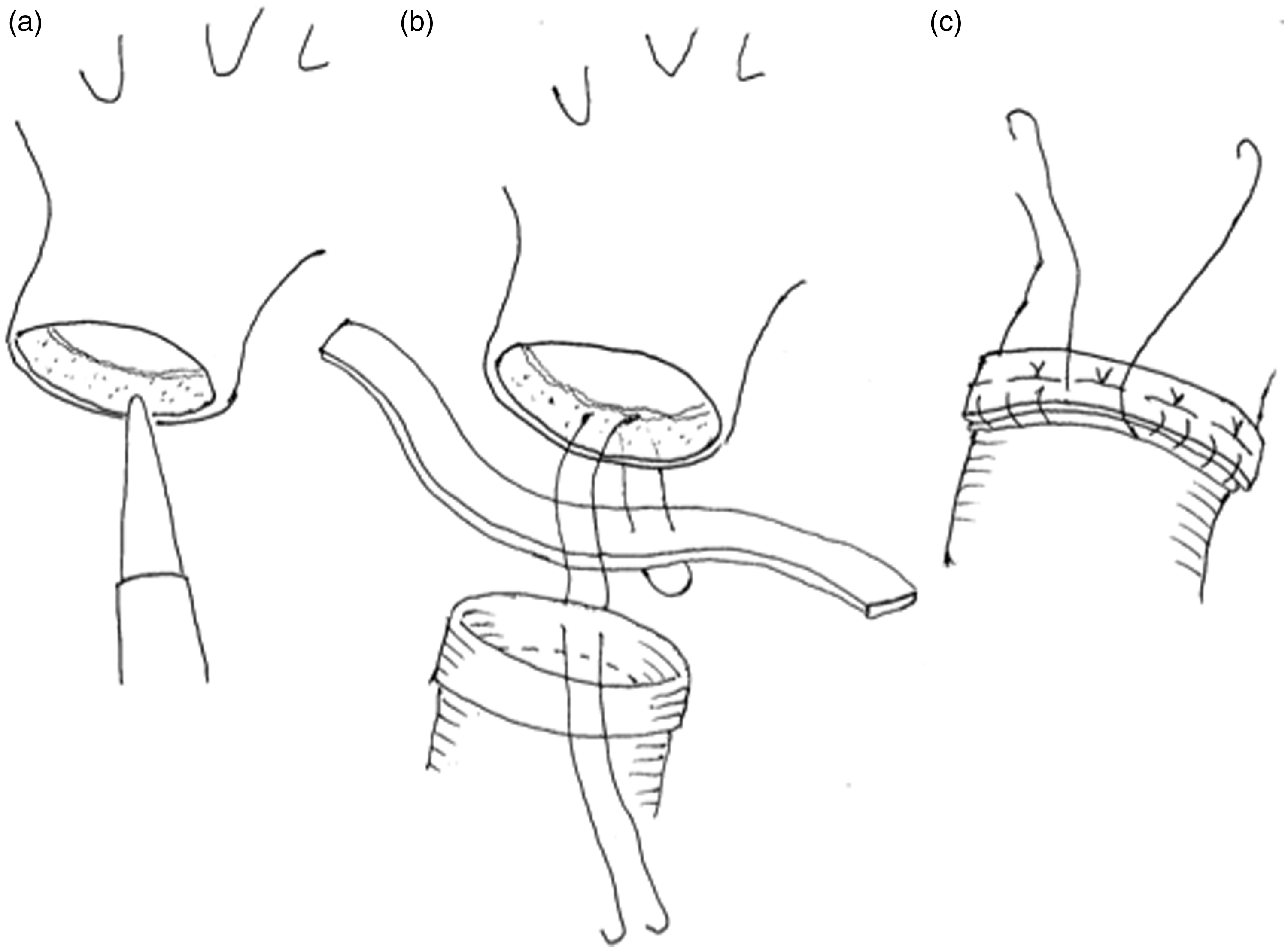
Discussion
Two patients underwent this procedure: one with severe aortic and mitral stenosis and angina pectoris had AVR and mitral valve replacement with concomitant coronary artery bypass grafting, and another with severe aortic stenosis had AVR. In both of these procedures, the CUSA was used in replacement of the ascending aorta. The cardiac arrest times were 215 and 90 min, respectively. We found that this graft replacement technique resulted in good hemostasis and reduced procedure time. For >10 postoperative months, these patients have been in a stable condition without development of an ascending aortic pseudoaneurysm (Figure 2).
Computed tomographic scans before and after surgery. (a) The distal ascending aorta showing circumferential calcification, (b) The distal ascending aorta after surgery, (c) The proximal ascending aorta showing dense circumferential calcification, and (d) The proximal ascending aorta after surgery.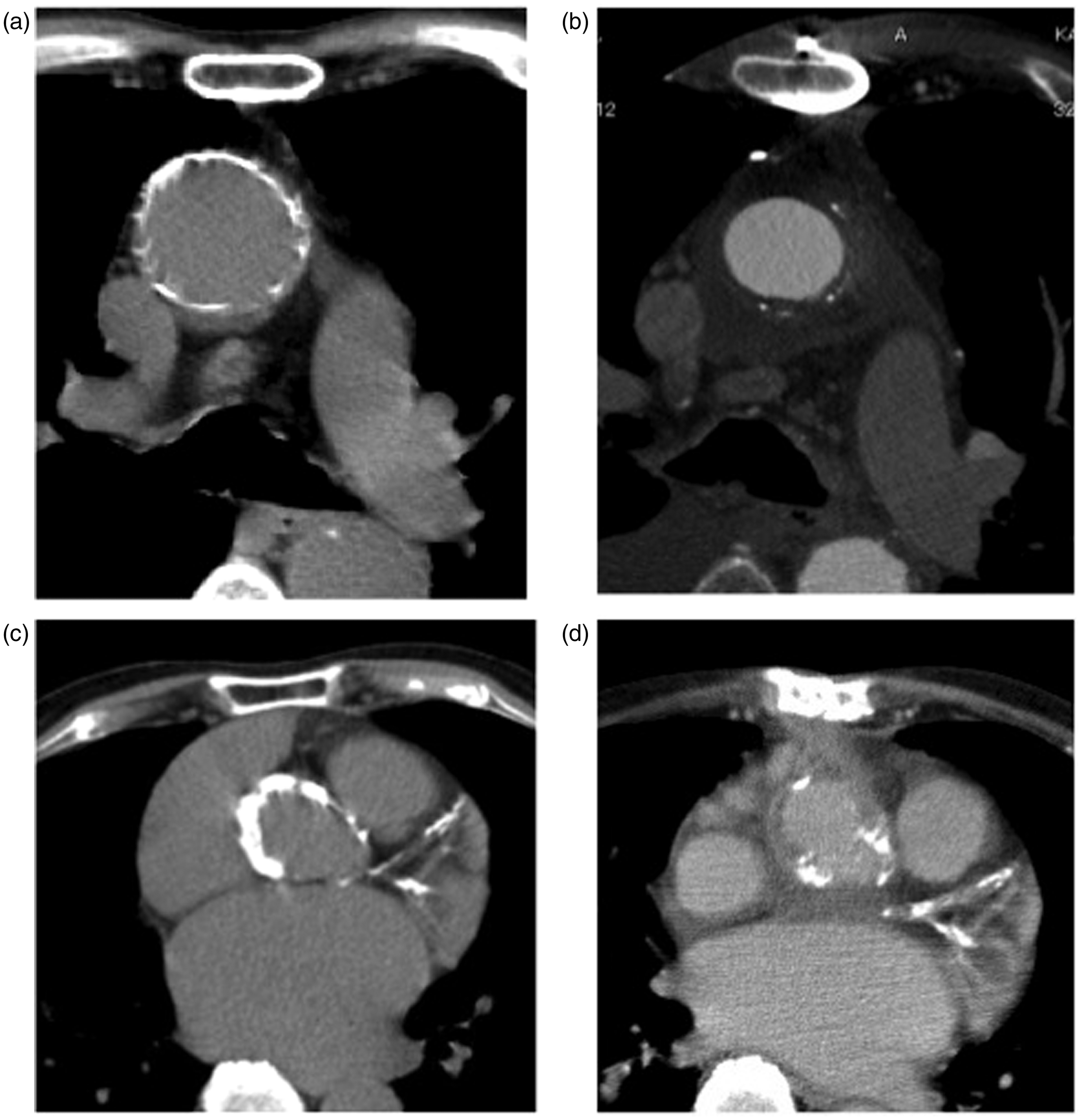
When simple AVR cannot be safely performed because the ascending aorta cannot be clamped, modification of the surgical procedure is mandatory. Several techniques are used for AVR during hypothermic circulatory arrest: endarterectomy or ascending aorta replacement,1,2 endoaortic balloon occlusion, 3 and apicoaortic conduit. 4 In spite of aggressive attempts to deal with the calcified ascending aorta, current surgical outcomes remained unsatisfactory. As an alternative to open surgery, the transcatheter aortic valve implantation (TAVI) procedure offers hope for patients with porcelain aorta, and a calcified ascending aorta is a good indication for TAVI. In these patients, TAVI can be performed safely and with a low incidence of neurological events and mortality.5–8 However, TAVI is not the optimal treatment for all patients with aortic stenosis, particularly patients requiring concomitant procedures such as coronary artery bypass grafting and/or mitral valve surgery. Thus surgeons should continue to modify their strategies by using conservative techniques to achieve better outcomes.
When severe aortic calcification is present at the aortotomy incision site, which makes suturing impossible, endarterial decalcification only around the suture line using a CUSA enables the aorta to be sutured safely.1,2 Endarterectomy at the aortic crossclamp site can also be performed safely using a CUSA.1,2 After decalcification with a CUSA, weakness of the aortic wall did not occur. This endarterectomy technique can be applied to replacement of the ascending aorta. Furthermore, mobile components of plaques and solid calcified lesions around the anastomotic part are quickly cleared by a CUSA without adventitial injury. After completion of the graft anastomosis, no suture line bleeding was noted, making this a safe, simple, and timesaving technique.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.