
Abstract
Background
Severe patient-prosthesis mismatch, defined as effective orifice area index ≤0.65 cm2 m−2, has demonstrated poor long-term survival after aortic valve replacement. Reported rates of severe mismatch involving the Perimount Magna aortic bioprosthesis range from 4% to 20% in patients with a small annulus.
Methods
Between June 2008 and August 2011, 251 patients (mean age 70.5 ± 10.2 years; mean body surface area 1.55 ± 0.19 m2) underwent aortic valve replacement with a Perimount Magna bioprosthesis, with or without concomitant procedures. We performed our procedure with rigorous patient-prosthesis matching to implant a valve appropriately sized to each patient, and carried out annular enlargement when a 19-mm valve did not fit. The bioprosthetic performance was evaluated by transthoracic echocardiography predischarge and at 1 and 2 years after surgery.
Results
Overall hospital mortality was 1.6%. Only 5 (2.0%) patients required annular enlargement. The mean follow-up period was 19.1 ± 10.7 months with a 98.4% completion rate. Predischarge data showed a mean effective orifice area index of 1.21 ± 0.20 cm2 m−2. Moderate mismatch, defined as effective orifice area index ≤0.85 cm2 m−2, developed in 4 (1.6%) patients. None developed severe mismatch. Data at 1 and 2 years showed only two cases of moderate mismatch; neither was severe.
Conclusions
Rigorous patient-prosthesis matching maximized the performance of the Perimount Magna, and no severe mismatch resulted in this Japanese population of aortic valve replacement patients.
Keywords
Introduction
In many studies, severe patient-prosthesis mismatch (PPM) has demonstrated poor long-term survival after aortic valve replacement in a variety of patient groups.1–3 The Carpentier-Edwards Perimount Magna (CEPM) aortic bioprosthesis (Edwards Lifesciences, Irvine, CA, USA) was introduced in 2002 as a modification of the Carpentier-Edwards Perimount standard (CEPS). The CEPM has an improved cuff design that allows implantation into a smaller aortic annulus. Dalmau and colleagues 4 reported lower mean and peak pressure gradients (PG), larger effective orifice areas (EOA), and lower rates of PPM with CEPM compared to CEPS. However, the reported rate of severe PPM using CEPM still ranged from 4% to 20% in patients with small annular diameters.5–8 To maximize CEPM performance and reduce the incidence of severe PPM, we performed aortic valve replacement surgery under rigorous patient-prosthesis matching with 3 policies. First, we chose a CEPM size based on careful measurement of annular size with a CEPM sizer. We consider the bioprosthesis size to be a size smaller than the sizer that passes through the annulus into the left ventricle, and always try to implant the exact size of bioprosthesis based on a sizer that precisely fits the annulus and does not enter the left ventricle. Complete annular decalcification is mandatory to perform this procedure. Second, we carry out annular enlargement when a 19-mm valve does not fit or when the EOA index (EOAI) is less than 0.85 cm2 m−2, based on the EOA data provided by Dalmau and colleagues, 4 but we did not have any such cases in this series. Third, we use a simple interrupted suturing technique instead of pledgeted everting or non-everting mattress sutures because the former has recently been reported to improve the performance of CEPM. 8 In addition, intraoperative transesophageal echocardiography (TEE) is used to measure the annulus. During TEE image acquisition, every effort is made to ensure that the largest annulus diameter is obtained. The objective of this study was to analyze the impact of our aortic valve replacement procedure, with rigorous patient-prosthesis matching, on the hemodynamic performance of the CEPM in the Japanese population.
Patients and methods
Characteristics of 251 patients undergoing aortic valve replacement.
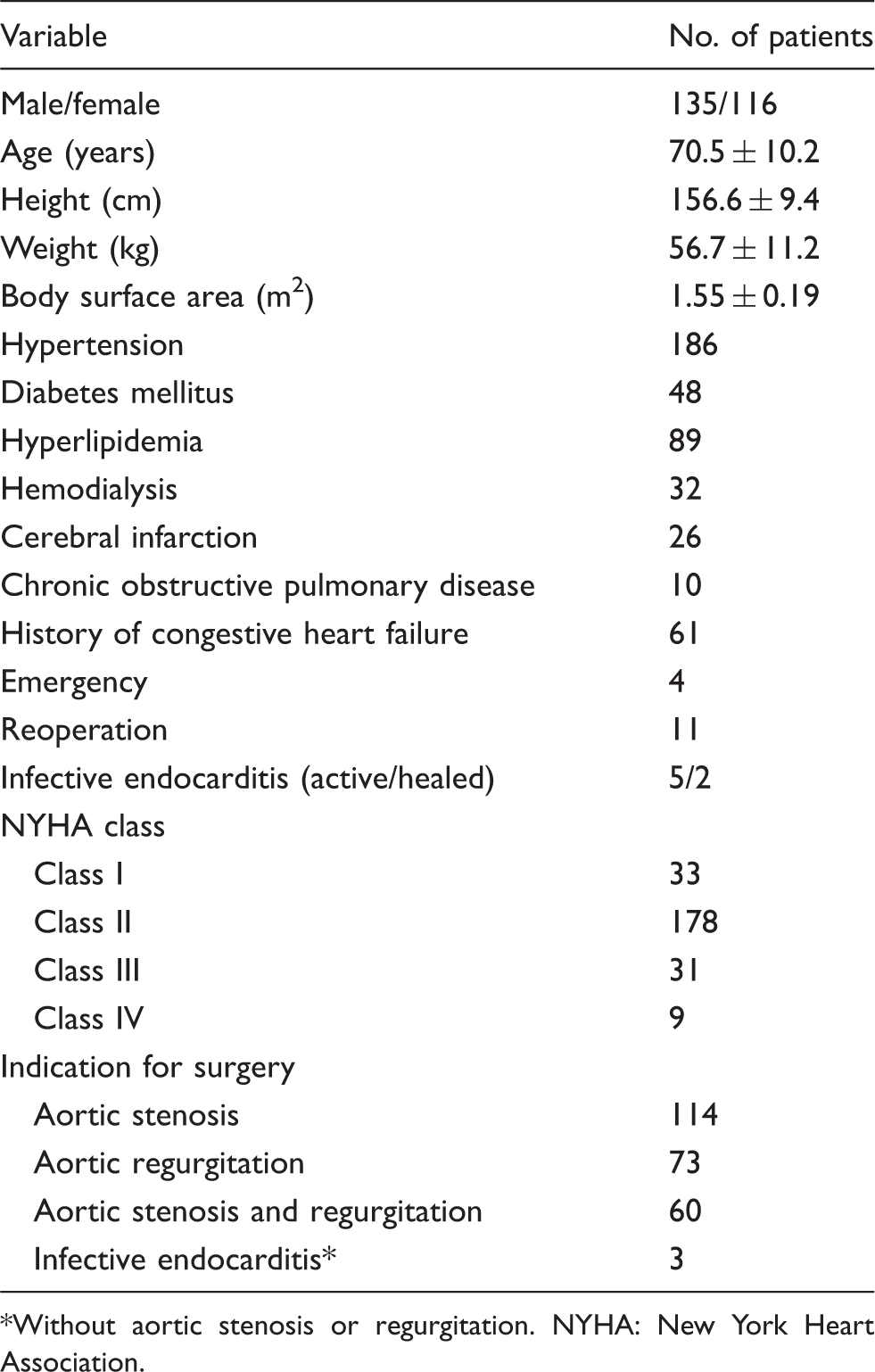
Without aortic stenosis or regurgitation. NYHA: New York Heart Association.
TTE was performed predischarge and at one and two years after surgery. The modified Bernoulli equation was used to calculate the maximum and mean PG across the valve. We calculated the EOA according to the continuity equation: EOA (cm2) = (LVOT diameter × 0.5)2 × π × (VTILVOT/VTIvalve), where LVOT and VTI are the left ventricular outflow tract and velocity time integral, respectively. 9 The EOAI was calculated by dividing the EOA by the body surface area. The left ventricular mass (LVM) was measured preoperatively and one year after surgery by TTE and calculated as: LVM = 0.8 × (1.04 × [(LVIDd + PWTd + SWTd)3 − (LVIDs) 3 ]) + 0.6 g, where the LVIDd and LVIDs are the diastolic and systolic left ventricular internal diameters, respectively, and PWTd and SWTd are the diastolic posterior and septal wall thicknesses, respectively. 11 The LVM index (LVMI) was calculated by dividing the LVM by the body surface area. Based on the definition by Blais and colleagues, 12 we defined PPM as severe or moderate when the prosthetic aortic valve EOAI was ≤0.65 cm2 m−2 or >0.65 and ≤0.85 cm2 m−2, respectively. The mean follow-up period was 19.1 ± 10.7 months (range 0.4–42.2 months), and the follow-up completion rate was 98.4%.
Continuous variables are expressed as mean ± standard deviation and categorical variables as frequencies (%). The t test for continuous variables was used to assess patients’ preoperative and operative data, and the chi-square or Fisher’s exact tests was used to assess categorical variables. Pearson’s correlation test was used to analyze the relationship between the annulus size measured by TEE and the implanted bioprosthesis size. The SPSS program (Dr. SPSS II; SPSS Inc., Chicago, IL, USA) was used to analyze all data. A p value <0.05 was considered to indicate statistical significance.
Results
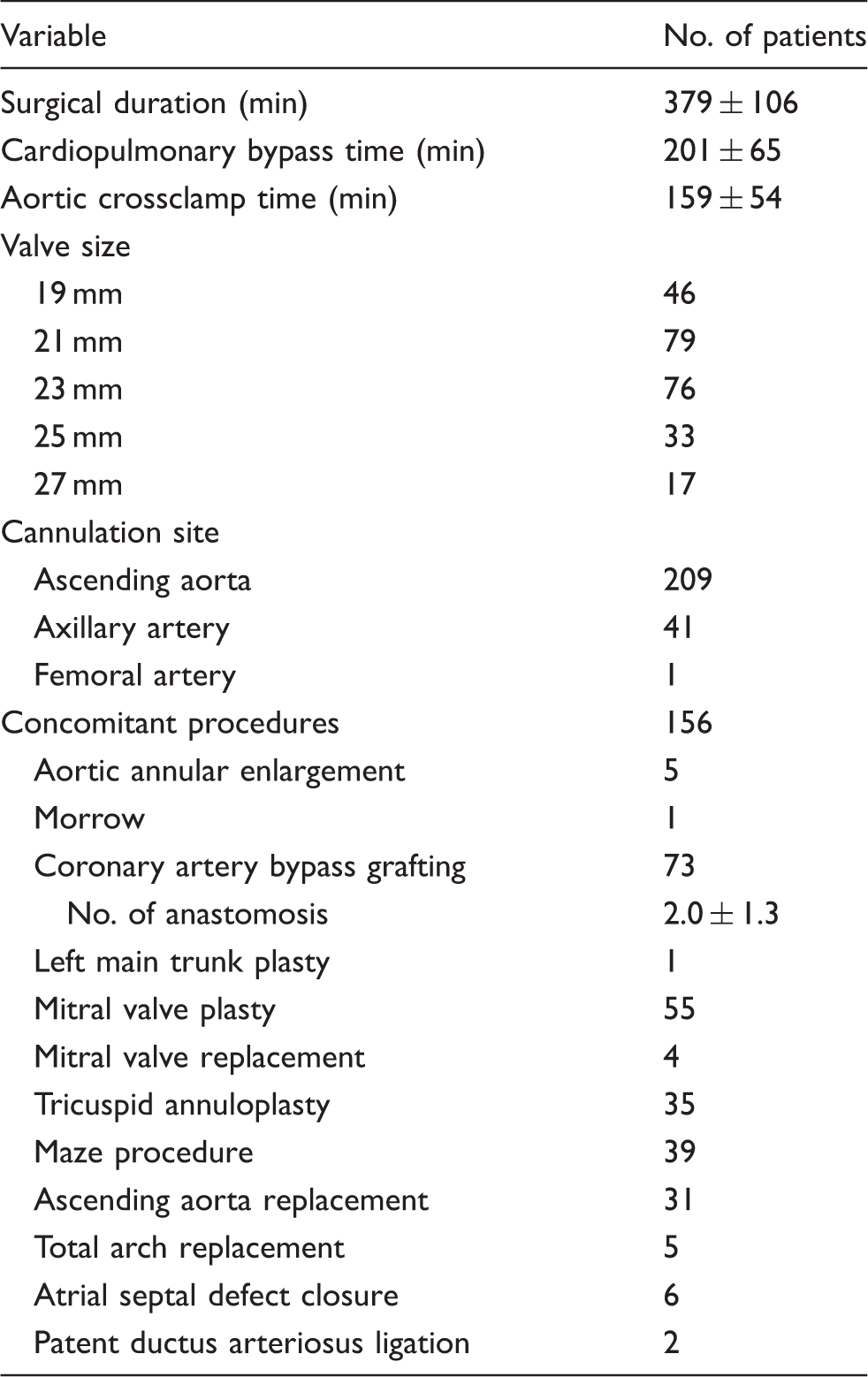
Surgical details of 251 patients undergoing aortic valve replacement.
Follow-up transthoracic echocardiography data.
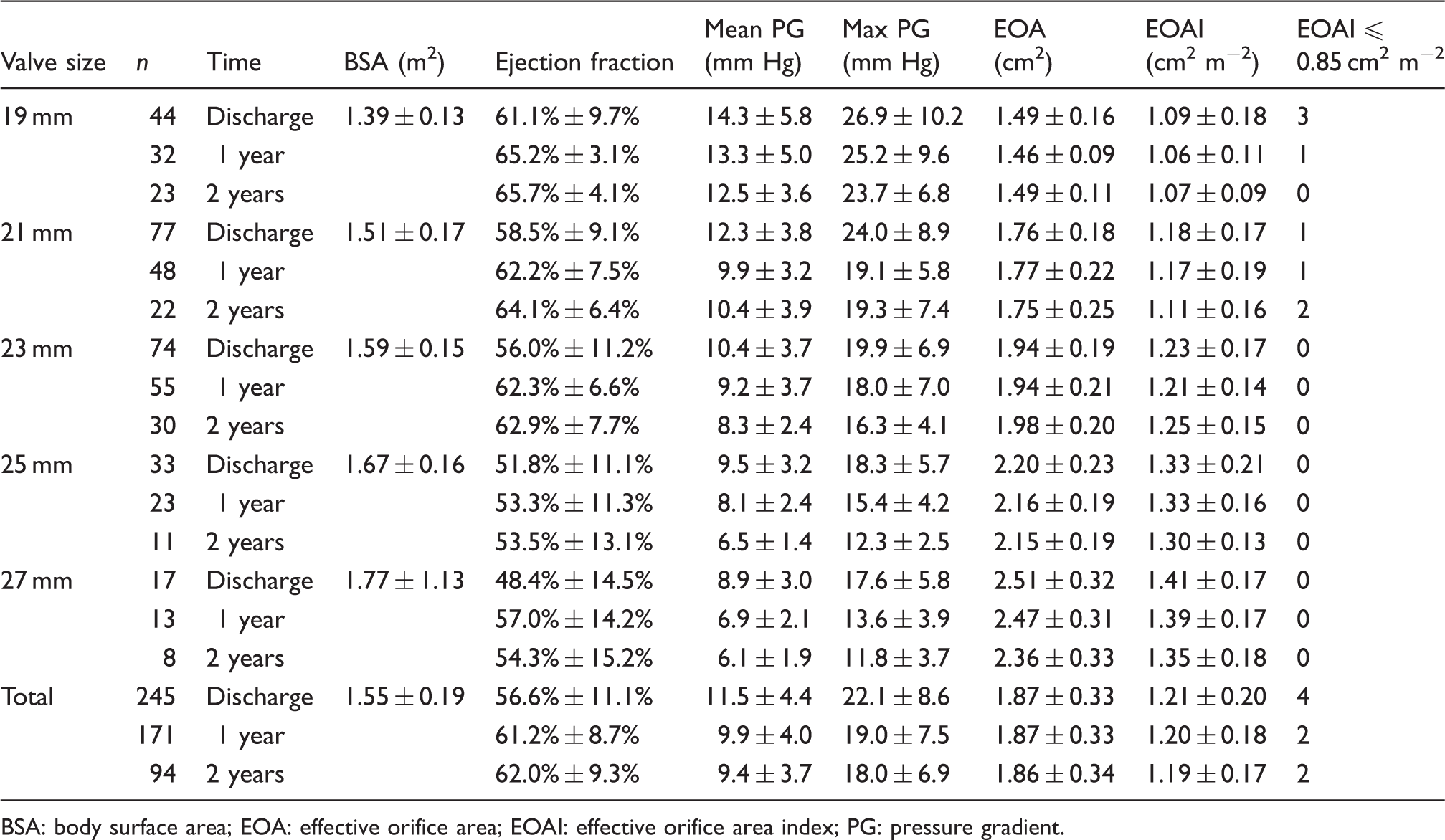
BSA: body surface area; EOA: effective orifice area; EOAI: effective orifice area index; PG: pressure gradient.
Changes in left ventricular mass, left ventricular mass index, and New York Heart Association class.
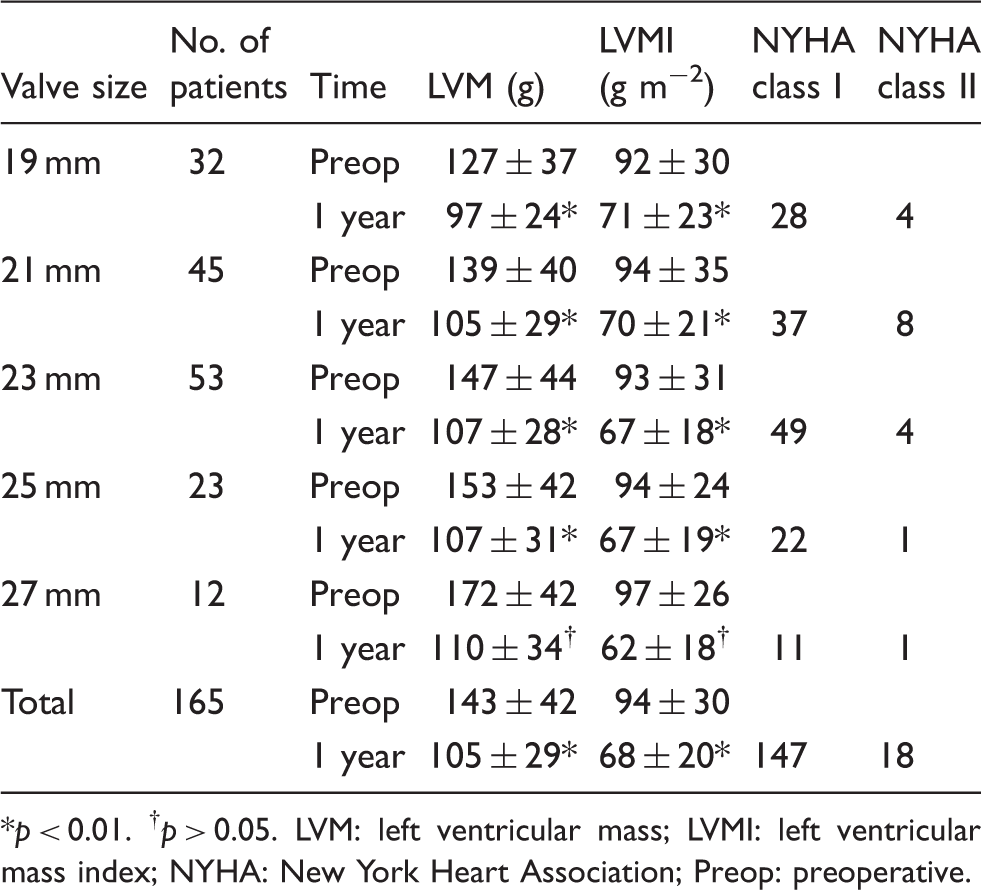
p < 0.01. †p > 0.05. LVM: left ventricular mass; LVMI: left ventricular mass index; NYHA: New York Heart Association; Preop: preoperative.
Discussion
Although it is still controversial, many reports have shown that the presence of severe PPM leads to significantly worse long-term survival in a variety of patient groups.1–3 The EOAI at rest is ideally >0.85–0.90 cm2 m−2 to maintain optimal valve performance during exercise. 13 Another study found that EOAI ≤0.80 cm2 m−2 increased the risk of heart failure after valve replacement by approximately 60%, but long-term survival was not significantly affected. 14 These findings suggest that a larger EOAI is one of the most important factors affecting a patient’s prognosis after aortic valve replacement. On the basis of these findings, we performed aortic valve replacement with a focus on careful patient-prosthesis matching. Our standard practice is to carefully implant exact-size prostheses based on the measured annular size. In addition, intraoperative TEE helped our decision-making. We initially trained our echocardiographers to measure the exact annular size. After they had performed measurements for a month, the values very closely matched the actual annular size, as shown by the correlation coefficient of 0.8. We then strived to implant the exact size of CEPM using a simple interrupted suture technique. 8 By combining these techniques, we achieved no severe PPM in our 251 patients.
The most striking feature of the CEPM valve is the narrow suture ring that maintains a large EOA. Dalmau and colleagues 4 described significantly larger EOA with 19-, 21- and 23-mm CEPM valves than with CEPS valves. Botzenhardt and colleagues 15 also reported that the CEPM valve resulted in a low mean PG and large EOA and EOAI compared to the CEPS valves with a 22–23-mm aortic annulus, whereas severe PPM was significantly less prevalent than that observed with CEPS valves with annulus diameters <22 mm. However, the reported rates of severe PPM using CEPM still range from 4% to 20% in patients with small annular diameters.5–8 We have been performing aortic valve replacement surgery by adding aortic annular enlargement (Nicks procedure) when a 19-mm valve did not fit. Although we add annular enlargement when the EOAI is less than 0.85 cm2 m−2, we did not have such cases in this series. The use of the Nicks procedure decreased after the induction of CEPM, and only 5 (2.0%) patients required annular enlargement to implant a 19-mm CEPM among our 251 patients. Again, by applying a careful patient-prosthesis matching policy, we achieved no severe PPM. We observed a postoperative EOAI > 1.0 cm2 m−2 for all sizes. Moreover, EOAI values were higher than those obtained using CEPM as described in previous reports.5–8
The LVMI as a measure of left ventricular hypertrophy has become a popular endpoint for assessing aortic valve replacement at follow-up.16–18 Incomplete regression of left ventricular hypertrophy after aortic valve replacement has been associated with increased mortality rates. 19 Fuster and colleagues 20 demonstrated that significantly higher hospital mortality in patients with high LVMI was promoted by coexisting PPM and a low left ventricular ejection fraction. The present study showed that our aortic valve replacement surgery produced a significant decrease in LVMI at the one-year follow-up, with New York Heart Association class improvement. Improved prognosis as well as quality of life is expected, and we continue to monitor our patients.
This study has several limitations. First, it is a retrospective short-term investigation with postoperative follow-up for only two years. Careful long-term follow-up is warranted. Second, we did not compare CEPM with other bioprostheses, and other valves should be used to further evaluate the careful patient-prosthesis matching. We concluded that a careful patient-prosthesis matching approach for aortic valve replacement surgery, using rigorous annular size measurement and a simple interrupted suturing technique to maximize the performance of CEPM, achieved no severe patient-prosthesis mismatch in 251 Japanese patients.
Footnotes
Acknowledgment
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.