
Abstract
Management of postpneumonectomy bronchopleural fistula remains a major challenge for thoracic surgeons. Successful closure of a postpneumonectomy bronchopleural fistula was performed in a 60-year-old man, using a flap made by a combination of serratus anterior and latissimus dorsi muscle which had been divided during the pneumonectomy operation. The flap was prepared on the presence of a dependable collateral serratus anterior branch to the lateral thoracic artery, which provides retrograde flow to the latissimus dorsi muscle.
Keywords
Introduction
The incidence of postoperative bronchopleural fistula (BPF) has been reported to be 1.5% to 28% in pneumonectomy cases. It can lead to life-threatening conditions such as postpneumonectomy empyema. 1 The mortality of a BPF is reported to be 15% to 75%. 2 Intrathoracic muscle flap transposition has been shown to be useful in controlling postpneumonectomy BPF. 3
Case report
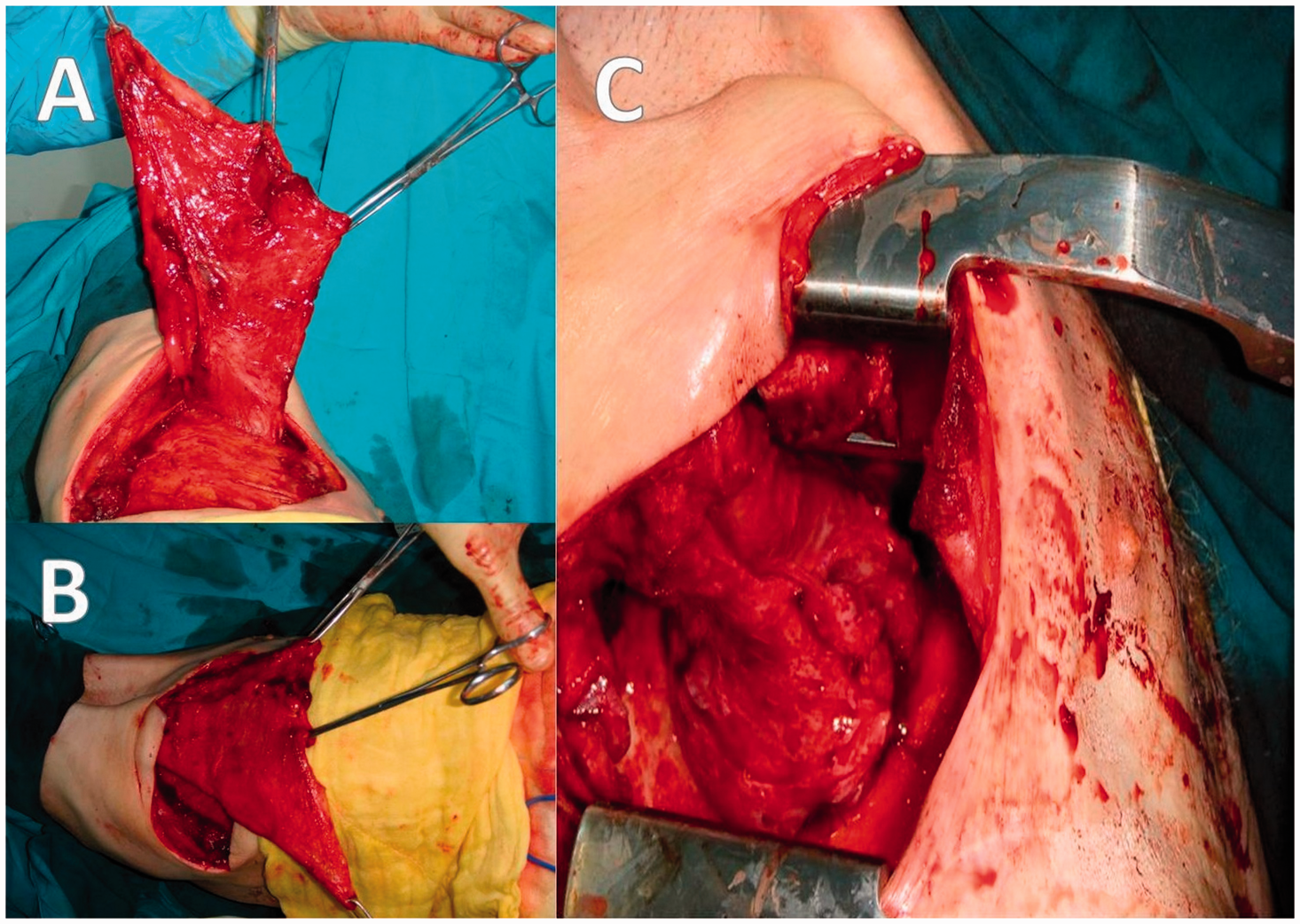
A 60-year-old man was admitted to our hospital with cough and sputum and was diagnosed with stage IIIA (T2N2M0) squamous cell carcinoma of the right upper lobe and intermediate bronchus. He had 3 cycles of neoadjuvant chemotherapy (gemcitabine, cisplatin) before undergoing a right pneumonectomy. No complication was observed during the immediate postoperative period, however, at the 1-year follow-up, a BPF was detected (Figure 1). Several attempts were made to treat the BPF with intrabronchial glue, but they were unsuccessful. At the 2-year follow-up, we noted empyema in the right hemithorax. We inserted a chest tube and irrigated the right intrathoracic space with antibiotic solution for 30 days. After confirming by culture that there was no infection in the thoracic cavity, we recommended treatment options to the patient, including chronic open drainage, direct stump closure with muscle reinforcement, or thoracoplasty, but the patient decided on closure of the BPF by transferring an intrathoracic muscle flap. The operative plan involved the segmental perforators of latissimus dorsi muscle as a reverse flap. In the operating room, the patient underwent double-lumen left-sided intubation, and the thoracotomy incision was reopened to the bronchial stump site at the 4th intercostal space. The bronchial stump was debrided and closed in a double-layer fashion with interrupted polypropylene sutures. We confirmed the presence of a dependable collateral serratus anterior branch to the lateral thoracic artery, which provides retrograde flow to the latissimus dorsi muscle. Cautious dissection was applied, the flap was elevated properly (Figure 2A, 2B), and inset to the fistula with a partial serratus anterior muscle flap without any problem (Figure 2C). We did not do any rib resection for this procedure, and ended the operation by placing a chest tube in the thoracic cavity. The patient was discharged on the 15 th postoperative day and he was well without any evidence of infection or BPF at the 6-months follow-up.
Bronchoscopic view of the bronchopleural fistula. (A) The latissimus dorsi muscle flap. (B) The combined latissimus dorsi and partial serratus anterior muscle flap. (C) The bronchopleural fistula was closed with the latissimus dorsi and serratus anterior muscle flap.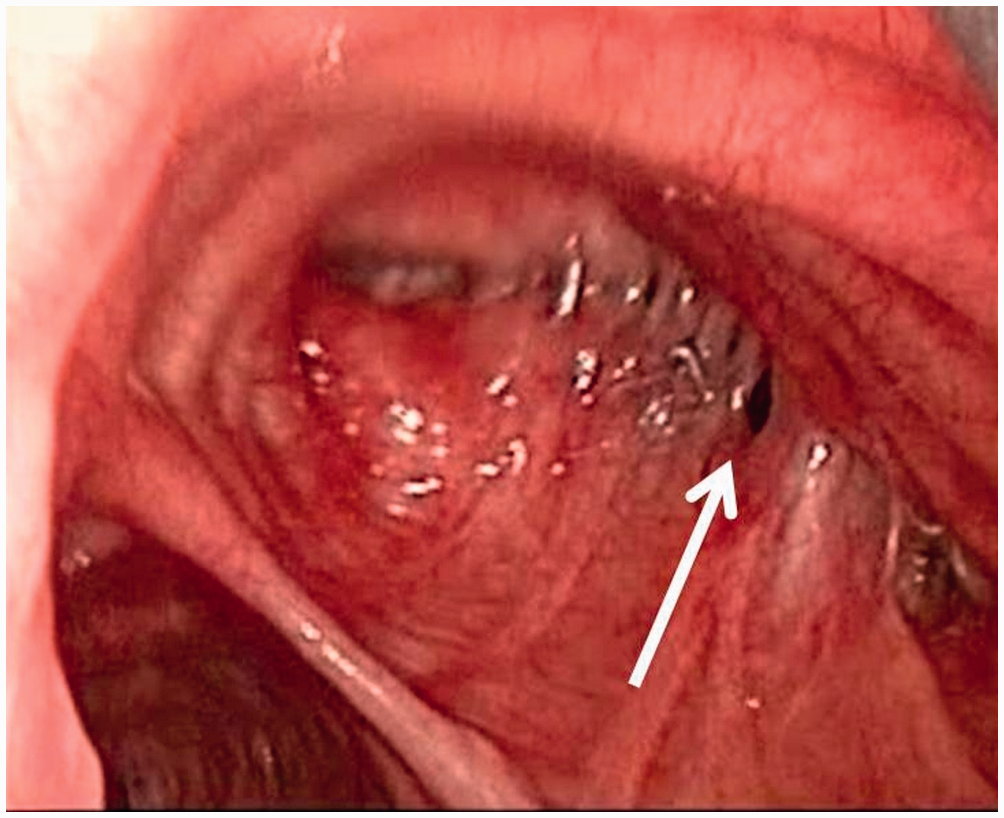
Discussion
Bronchopleural fistula remains the most frightening complication following pneumonectomy. The major factors contributing to the development of BPF after pneumonectomy are induction chemo/radiotherapy, a right pneumonectomy, and postoperative mechanical ventilation. 1 The factors in our patient were induction chemotherapy and a right pneumonectomy. If empyema and BPF are detected after pneumonectomy, the first step is to put a chest tube into the thoracic cavity for drainage and irrigation with antibiotic solution. Surgical approaches include chronic open drainage, direct stump closure with muscle reinforcement, an omental flap, transsternal bronchial closure, and thoracoplasty with or without extrathoracic chest wall muscle transposition.2,3 In this case, the BPF was small and we tried to manage it with endobronchial glue several times before surgery, but obtained inadequate results, so we recommended chronic open drainage first, but the patient opted for BPF closure with muscle reinforcement.
A standard posterolateral thoracotomy generally divides the latissimus dorsi muscle and rarely divides the serratus anterior muscle, so after a previous posterolateral thoracotomy, a serratus anterior muscle flap is frequently the choice for BPF closure. 3 Transposition of the serratus anterior muscle results in some degree of scapular winging. Segmental use of the serratus anterior muscle for intrathoracic transposition has been used to overcome this situation. 3 Nevertheless, the serratus muscle flap is thin, short, and has 3 separate parts, which sometimes limits its use for closure of a BPF. Latissimus dorsi muscle is a type V muscle according to its blood supply, thoracodorsal vessels, or intercostals or lumbar perforators. The proximal part of the muscle can be pedicled on the thoracodorsal vessels or the serratus branch. The thoracodorsal artery gives off 1–2 branches to the serratus muscle prior to entering the latissimus dorsi muscle.3,4 It can be elevated at full length and has a bulky tissue that provides reliable closure of a BPF. This procedure should have a multidisciplinary approach involving plastic surgeons because it needs advanced skills in the preparation of the pedicled latissimus dorsi flap on the segmental perforators and branch vessels. 4 In this case, the operation was performed by a team of thoracic and plastic surgeons. The procedure ended successfully, and the healing period was uneventful without scapular winging. We concluded that the use of a latissimus dorsi muscle flap pedicled on the collateral serratus branch of the thoracodorsal artery is a safe and valuable option for closing a BPF, even after a previous posterolateral thoracotomy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.