
Abstract
Sternal cleft is a rare chest wall deformity associated with various malformations. Primary closure is the gold standard in the newborn period. Alternative techniques are possible for older patients. A 23-year-old woman with a partial sternal cleft and no additional deformity, underwent reconstruction using costal cartilage grafts. Postoperative physical and functional were excellent.
Introduction
Sternal cleft is a rare congenital anomaly; there are approximately 100 cases reported in the literature. This anomaly can be partial or complete and may be associated with many malformations (anterior cervical web, hemangiomatosis, central nervous system malformations, coloboma, and pectus excavatum). 1 Visible pulsation in the chest may be the presenting sign. 1 A sternal cleft may be V-shaped when it reaches the xiphoid process, or broad and U-shaped with a bony bridge joining the two edges, ending at the 3rd or 4th costal cartilages. 2 Surgical correction is indicated as soon as possible after birth to protect vital intrathoracic organs. Surgery is preferred in the neonatal period because the flexibility of the sternum is maximal and compression of underlying structures is minimal. 3
Case report
A 23-year-old woman with a congenital sternal cleft presented to the thoracic surgery outpatient clinic. Her physical examination was otherwise normal. She had undergone a dermoid cyst operation 4 years earlier. Laboratory examinations, pulmonary function tests, electrocardiography and imaging results were normal. Surgical repair was undertaken. In a supine position, a 10-cm vertical incision were made at the midline where the sternal cleft was located. The soft tissues on the sternal faces of both sides were dissected. It was seen that the upper two thirds of the sternum was not fused at the midline. Costal cartilages were resected on both sides, and the perichondrium was sutured back. The posterior sternal wall was formed with periosteal flaps from the sternal bars with absorbable sutures (Figure 1). Both sides of the sternal cleft were approximated with the aid of 4 wire sutures. Four autologous cartilage grafts (3rd–4th costal cartilages from both sides) were placed at the sternal opening to fill the gap. After bleeding control, the pectoralis muscle fiber was sutured back. Two closed-suction drainage tubes were placed, and the incision was primarily closed. The operation lasted for 120 min. Postoperative analgesia was provided by intravenous patient-controlled analgesia for two days, and continued with intermittent intravenous analgesics. There were no postoperative complications. The patient wore a sternal corset after the surgery. She was discharged two days postoperatively. The functional and cosmetic results were good after complete healing. A follow-up examination at 6 months revealed a stable sternal repair with well-healed soft tissue coverage.
Suturing at the midline of sternal cleft with stainless steel wires.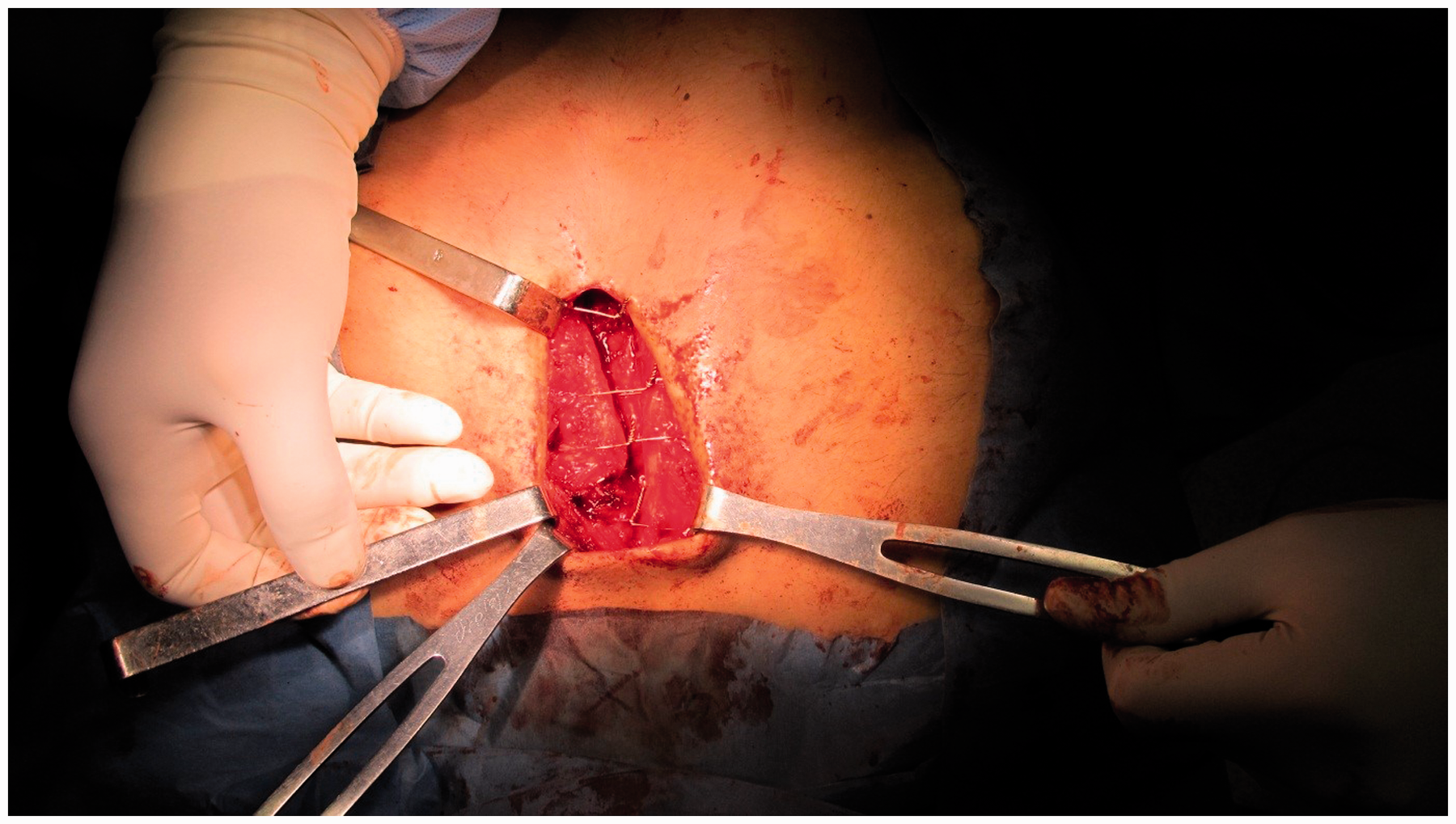
Discussion
Sternal cleft is a rare congenital anomaly resulting from failure of fusion of the two lateral mesodermal sternal bars by eight weeks of gestation. 4 A female dominance (8:1) has been reported. 4 There are many associated anomalies, but our patient had only a dermoid cyst. A concave midline thoracic defect and paradoxical chest wall movements with respiration is one of the main symptoms of this disorder, as seen in our patient. 1 Sternal cleft is a rare deformity and potential injury to the intrathoracic structures could be the indication for surgery. In the absence of vital indications, surgery is cosmetic. Infancy and childhood, especially the first month of life, is the optimal time for this operation, due to the elasticity of the sternum and minimal compression of underlying structures. 1 Isolated sternal cleft has a good prognosis, and surgery is easy and safe in these patients. 4 As the child grows, the decrease in chest volume with surgery may cause restriction. 1 Early operation is also necessary for a better surgical and cosmetic outcome. Chest wall rigidity and no space for accommodation of the intrathoracic organs must be considered in adult patients with sternal cleft. 3 However, successful surgical repairs in adults have also been reported. 3 Our patient was 23-years old and she had a successful operation without any complication.
Various surgical techniques for repair of cleft sternum have been described. Primary approximation, sliding or rotating chondrotomies, and reconstruction of the defects with the use of prosthetic grafts or flaps of bone, cartilage, autogenous tissue, or pectoralis major muscle are the main techniques.
3
In older patients, autologous grafts are preferable due to less reaction and less infection risk.
4
Thus we used the 3rd and 4th rib cartilages as grafts, and closure was obtained with the technique of de Campos and colleagues
5
(Figure 2). The risk of necrosis of the graft is minimal, and neovascularization from the neighboring tissues is achieved after the surgery. For older patients, as in our case, autologous repair is appropriate to avoid problems associated with the use of prosthetic materials.
Representative figure of surgical procedure. There was no sternal resection in our case. Reproduced with permission from: de Campos JR, Filomeno LT, Fernandez A, et al. Repair of congenital sternal cleft in infants and adolescents. Ann Thorac Surg 1998;66:1151–1154.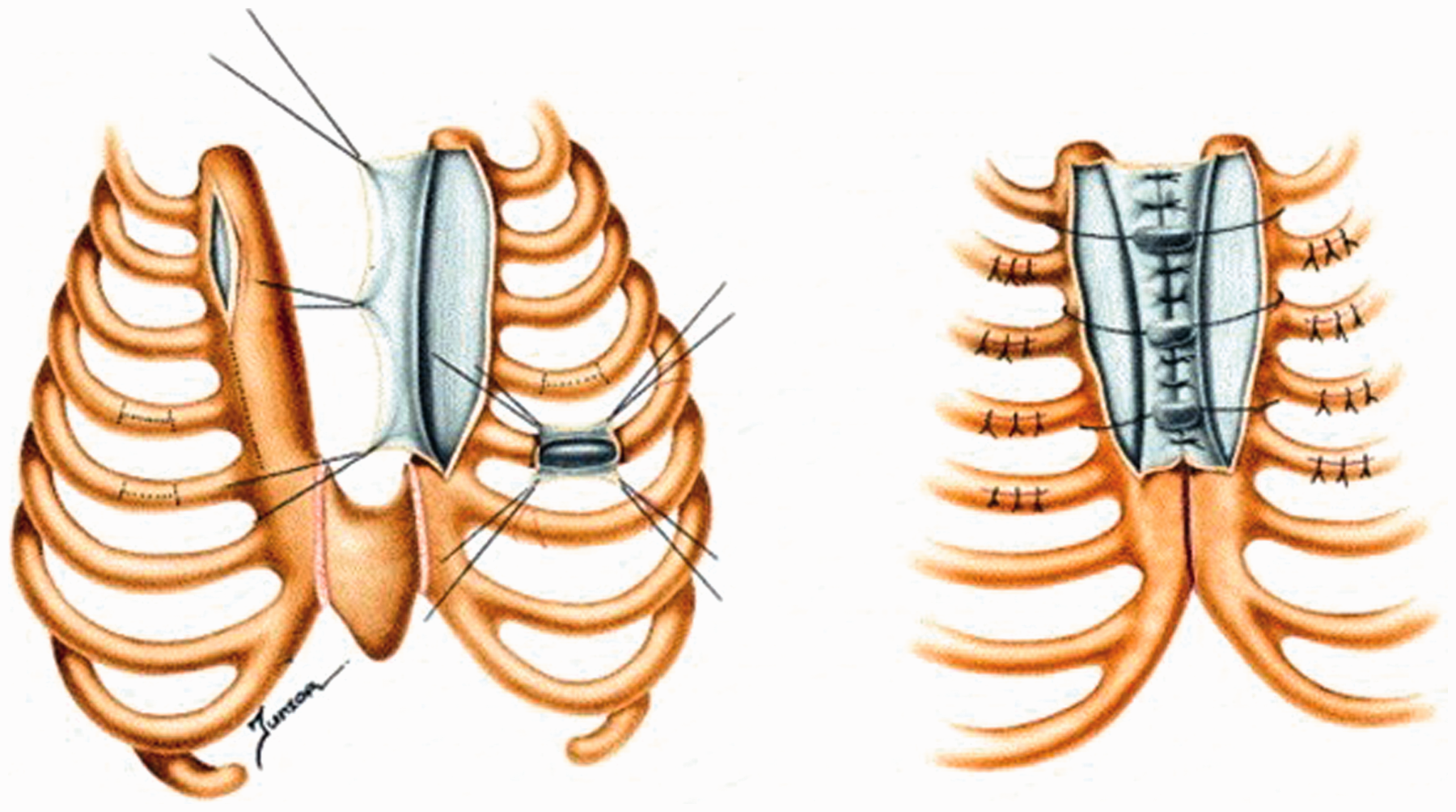
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared