
Abstract
Objective
To determine whether patients with single-ventricle physiology who are free from known risk factors could skip routine pre-Fontan hemodynamic evaluation, without affecting the postoperative outcome.
Methods
A diagnostic algorithm including echocardiographic, clinical, and angiographic risk factors was used retrospectively to evaluate all 44 patients who underwent Fontan completion at Hamad General Hospital between January 2000 and December 2012. We evaluated the efficacy of this algorithm as a screening tool to identify inoperable and high-risk patients in whom pre-Fontan cardiac catheterization should be performed.
Results
Mean age at Fontan completion was 5.9 years (range 1.08–24.5 years), and mean weight was 18 kg (range 7.4–60 kg). Three patients were found to be inoperable based on hemodynamic cardiac catheterization results. The algorithm was highly sensitive in detecting all 3 inoperable patients who were classified as high-risk subjects. Of the other 41 patients, 17 (41%) had no risk factors and 24 (59%) had one or more risk factors. This noninvasive algorithm showed a sensitivity of 83% and specificity of 76% in detecting adverse postoperative outcomes. The sensitivity did not change after adding hemodynamic data obtained by cardiac catheterization as additional risk factors.
Conclusion
This noninvasive diagnostic algorithm could be used as an effective screening tool to detect patients in whom pre-Fontan cardiac catheterization could be avoided; magnetic resonance imaging and computed tomography can be a good substitute.
Keywords
Introduction
The Fontan operation has gone through multiple incarnations since Fontan and Baudet’s initial description in 1971. 1 In the final stage, this operation achieves complete separation of the pulmonary and systemic venous circulation and hence adequate systemic arterial saturation in patients who are unable to undergo biventricular repair.2,3 There is significant morbidity and mortality in Fontan surgery. 4 To minimize the morbidity and mortality, hemodynamic and anatomical abnormalities such as ventricular function, pulmonary artery pressure and resistance, ventricular filling pressure, coarctation of aorta, pulmonary artery distortion and abnormal collateral vessels should be evaluated. Invasive hemodynamic and angiographic evaluation by cardiac catheterization used to be part of pre-Fontan assessment, aimed at detection of inoperable patients and those with a high risk of postoperative complications. Pre-Fontan catheterization also provides a chance to identify patients in whom additional interventions are required before or during the Fontan procedure. Complications have been reported in 5%–10% (and death in 0.1%) of patients undergoing cardiac catheterization.5–7 Furthermore, the development of noninvasive diagnostic tools, such as cardiac magnetic resonance imaging (MRI) and computed tomography (CT), provides attractive alternatives to obtain the angiographic data needed for pre-Fontan assessment. Consequently, there is increased interest in substituting invasive pre-Fontan catheterization by noninvasive procedures. 8 In the absence of certain known risk factors (clinical and echocardiographic), a patient is unlikely to be considered unfit for a Fontan procedure. 9 These risk factors, determined clinically or by noninvasive imaging, have been shown to be associated with increased risk of adverse outcomes after the Fontan operation.9–11 Hence the value of invasive evaluation of single-ventricle patients without these risk factors has been questioned. Noninvasive risk criteria have been assessed in retrospective and prospective studies, and some have been included in algorithms. We used an algorithm that included previously studied risk factors and applied it retrospectively to our Fontan patients to divide them into high-risk and low-risk groups. Only patients with one or more risk factors were subjected to hemodynamic assessment by cardiac catheterization. Our aim was to assess the sensitivity of the algorithm in detecting inoperable patients as well as to determine the effect of eliminating invasive hemodynamic data on postoperative outcomes. CT and MRI data were not available in our patients. Similar to Prakash and colleagues, 10 we utilized angiography to identify risk factors. This approach considered CT/MRI imaging to be equivalent to catheterization, as shown in a number of studies.12–15 Echocardiography was used to detect aortopulmonary collaterals using color Doppler in suprasternal view. The right pulmonary artery is easier to detect than the left pulmonary artery by echocardiography, for which stenosis or discontinuity may be difficult to assess by echocardiography as the sole modality.
Patients and methods
Demographic data of 44 patients undergoing Fontan completion.
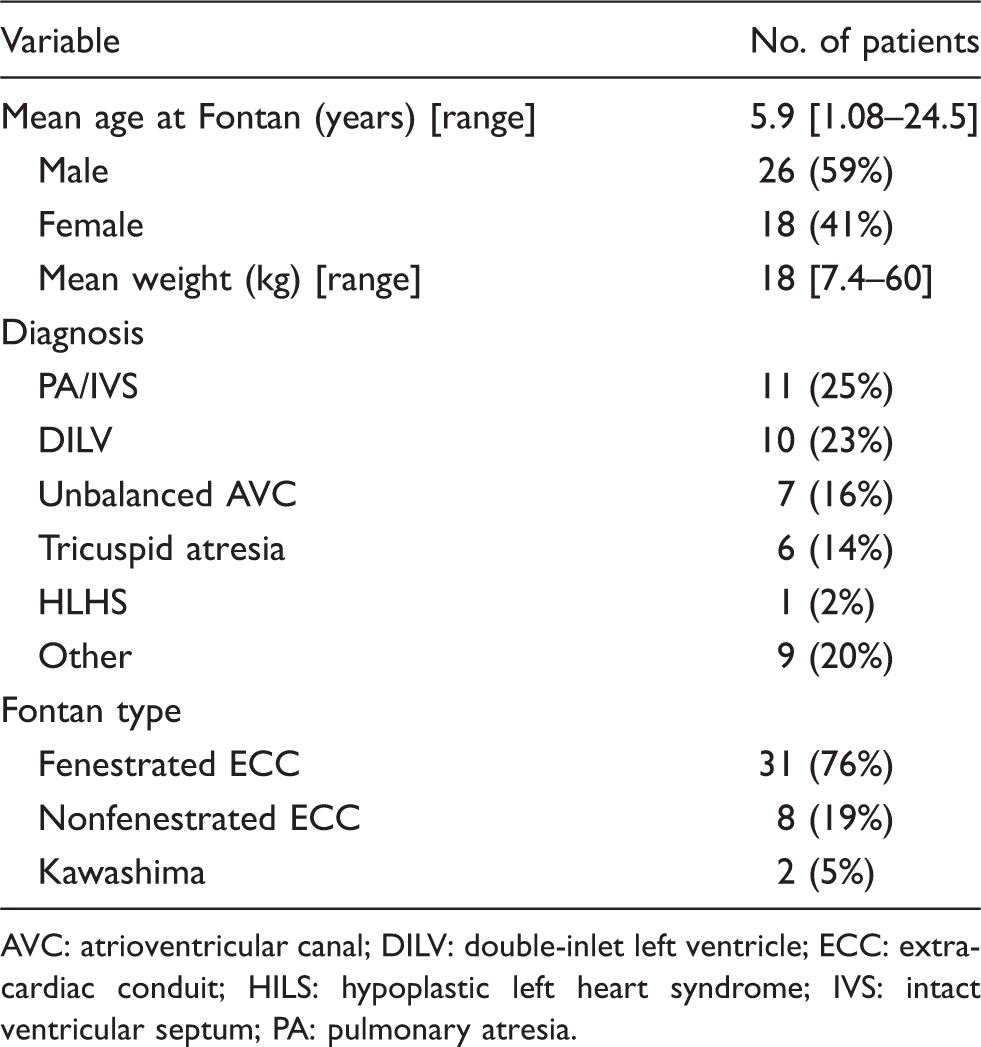
AVC: atrioventricular canal; DILV: double-inlet left ventricle; ECC: extracardiac conduit; HILS: hypoplastic left heart syndrome; IVS: intact ventricular septum; PA: pulmonary atresia.
Based on the algorithm used (Figure 1), 24 (59%) patients had one or more risk factor and were classified as high-risk, and 17 (41%) were in the low-risk group. Their data were collected retrospectively after thoroughly reviewing the medical records. The following data were included: diagnosis; preoperative clinical, echocardiographic and angiographic risk factors (Table 2); pulmonary artery pressure (PAP) and ventricular filling pressure (VFP) obtained at cardiac catheterization; age at Fontan completion; type of Fontan procedure; and adverse postoperative outcomes including prolonged (>10 days) intensive care stay, prolonged (>15 days) pleural drainage, the need for recatheterization within 3 months postoperatively, or death within one year of the operation. The predictive ability of the algorithm (sensitivity, specificity, positive-predictive value, negative-predictive value, likelihood ratios, and post-test probability) to detect inoperable as well as high-risk cases was calculated. These algorithm predictive values were repeated after including the hemodynamic data obtained by cardiac catheterization (PAP and VFP) as additional risk factors. An extracardiac Fontan procedure was performed in 39 (95%) cases; 31 (79.5%) fenestrated and 8 (20.5%) nonfenestrated, and 2 (5%) patients had a Kawashima procedure.
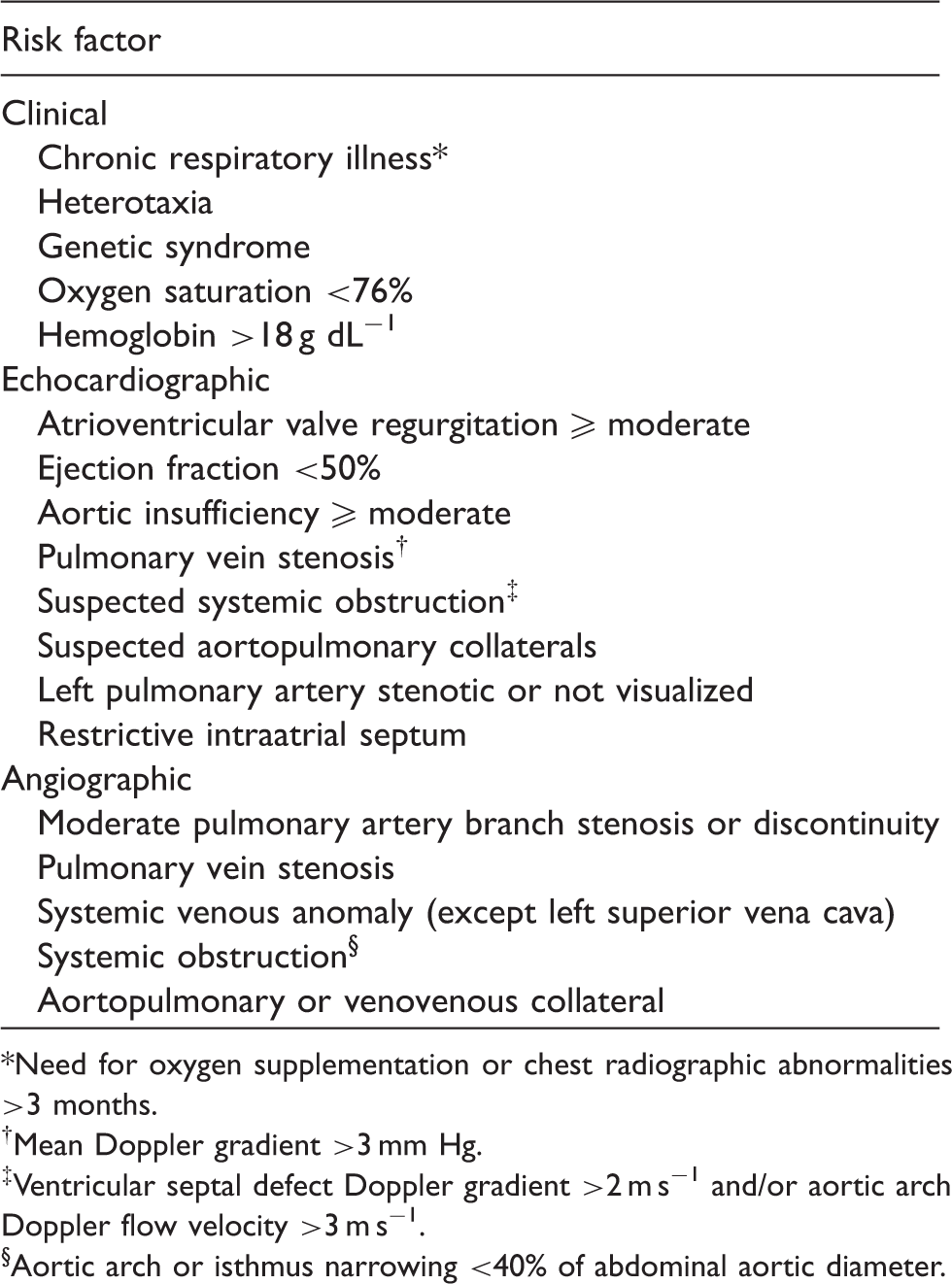
Proposed diagnostic algorithm for pre-Fontan assessment. Cath: catheterization. Risk factors predicting the need for catheterization. Need for oxygen supplementation or chest radiographic abnormalities >3 months. Mean Doppler gradient >3 mm Hg. Ventricular septal defect Doppler gradient >2 m s−1 and/or aortic arch Doppler flow velocity >3 m s−1. Aortic arch or isthmus narrowing <40% of abdominal aortic diameter.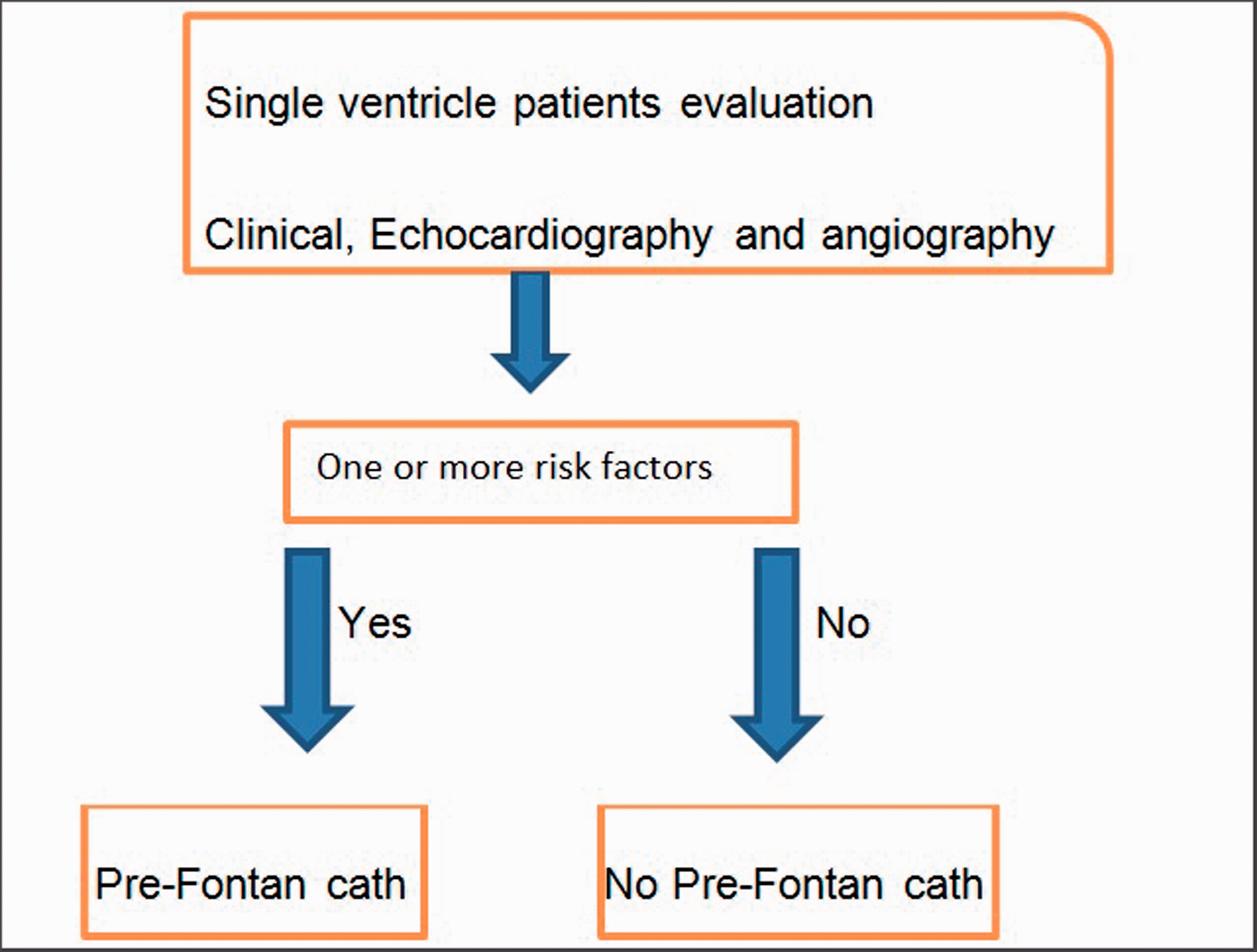
Results
Prediction of adverse post-Fontan outcomes using the algorithm with and without hemodynamic data.
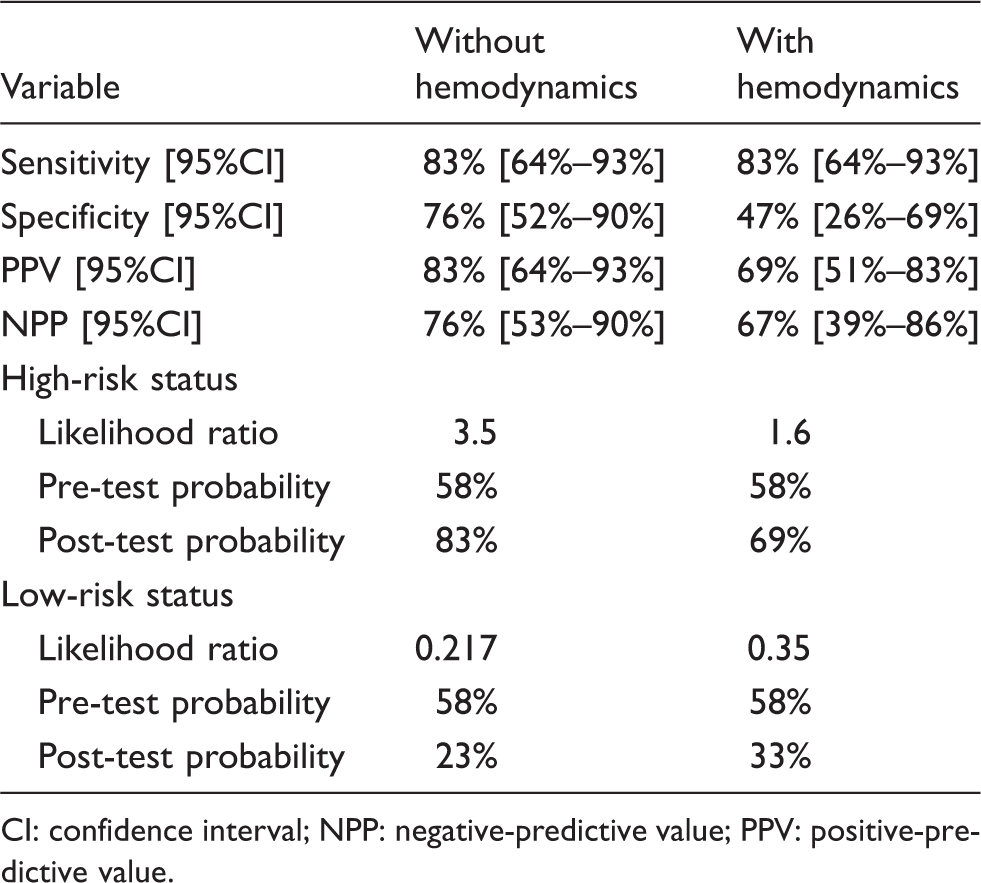
CI: confidence interval; NPP: negative-predictive value; PPV: positive-predictive value.
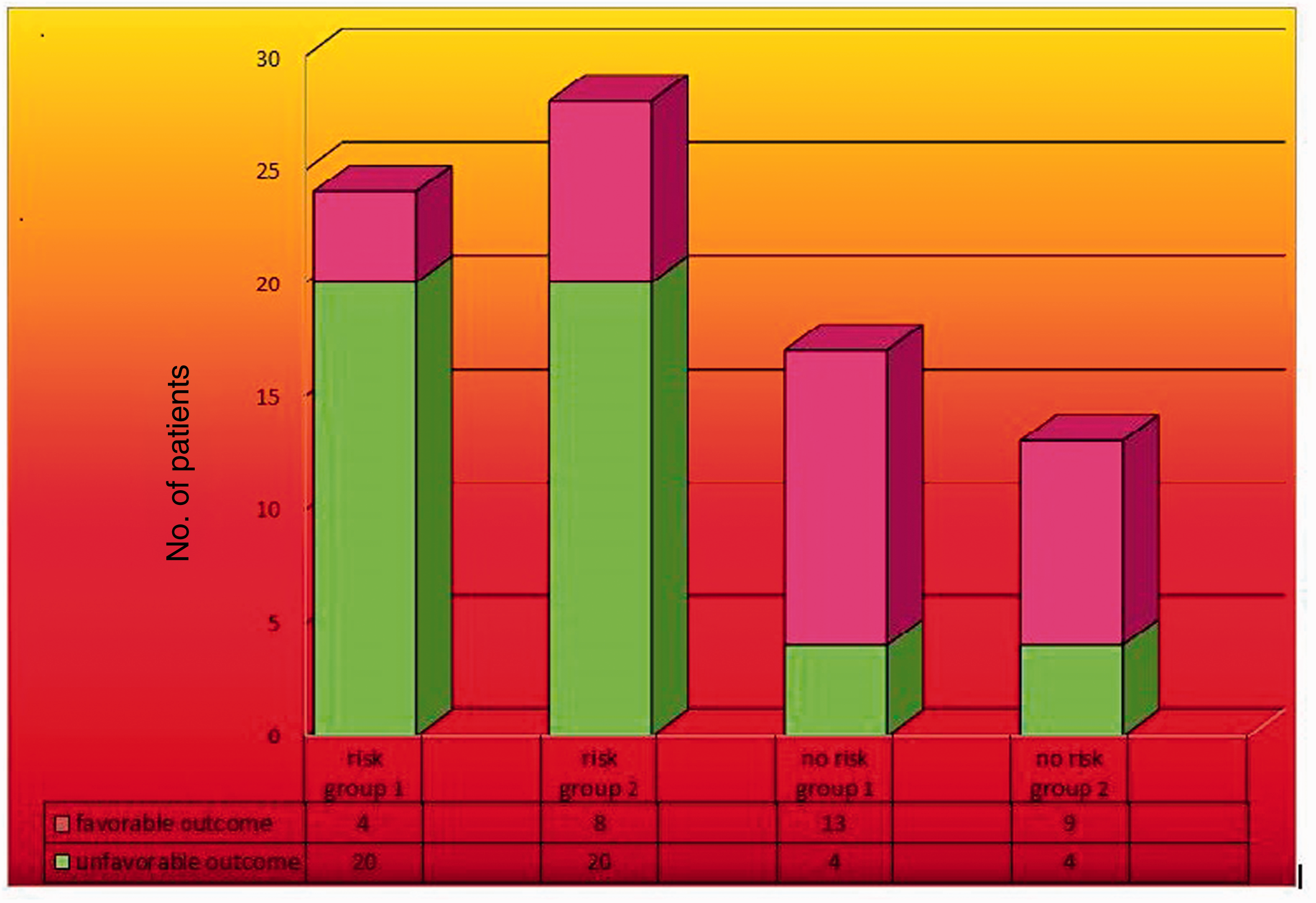
Comparison of Fontan outcome before and after including hemodynamic data. Risk group 1 and no risk group 1: pulmonary artery pressure and ventricular filling pressure not included; risk group 2 and no risk group 2: pulmonary artery pressure and ventricular filling pressure included.
Discussion
Cardiac catheterization is a common supplement in preoperative evaluation, which provides the benefit of immediate intervention if required. Although catheterization can be performed safely, it is not a risk-free procedure.5–7 Whether cardiac catheterization is necessary before the Fontan operation remains controversial, especially when sufficient data are provided by echocardiography and MRI. 11 Avoiding routine pre-Fontan cardiac catheterization is a new evolving trend for patients without known risk factors. In this study, we aimed to determine the possibility of avoiding routine pre-Fontan cardiac catheterization in the subset of patients without known risk factors. To achieve this, an algorithm that included these risk factors was retrospectively applied and evaluated for its predictive value. Similar to the results of Prakash and colleagues 10 in a similar study, this algorithm proved to be highly sensitive in screening pre-Fontan patients and identified all 3 inoperable patients in our study group. Accordingly, this algorithm can be used as a screening tool to identify high-risk patients who should then have preoperative cardiac catheterization. When considering the algorithm’s ability to identify adverse postoperative outcomes, again it showed high sensitivity and specificity, which did not improve by including hemodynamic data (PAP, VFP) as additional risk factors. In addition, there was no significant difference in PAP and VFP between the high- and low-risk groups. Also, there was a significant correlation between high-risk status and adverse postoperative outcomes in the absence of hemodynamic risk factors. Adding the hemodynamic data obtained by cardiac catheterization did not improve the algorithm’s sensitivity, thus giving a less significant relationship between high-risk status and adverse postoperative outcome. This indicates that omission of the hemodynamic data in patients who are free of such risk factors would not affect its ability to predict adverse postoperative outcomes, and hence this algorithm is a useful screening tool which could determine which type of patient needs to have pre-Fontan catheterization.
A retrospective study by Gaynor and colleagues 16 showed that increased preoperative PAP increased the risk of early death. In a study by Culbertson and colleagues, 17 high mean PAP was found to be one of the factors that increases the risk of a Fontan procedure. Contrary to these studies, our results did not show a significant relationship between hemodynamics obtained by cardiac catheterization and adverse postoperative outcomes. These results are in accordance with a similar retrospective study by Ro and colleagues 9 who developed a set of echocardiography, hemoglobin, and pulse oximetry criteria to determine the need for catheterization prior to Fontan. The negative-predictive value of these criteria to discriminate patients who could forgo catheterization was 76%, but the positive-predictive value of this strategy was rather low. A retrospective study by Brown and colleagues 18 demonstrated that unless indicated by echocardiography, routine cardiac catheterization prior to surgery rarely provided new information or resulted in an intervention. However, echocardiography, was only 70% successful in completely characterizing preoperative patients, and 73% successful in pulmonary artery assessment. Similarly, the algorithm proposed by Prakash and colleagues 10 suggested dividing single-ventricle patients into high-risk and low-risk groups based on history, echocardiography, and angiography data. They stated that the algorithm could effectively screen patients unsuitable for a Fontan procedure, and may be able to determine who needed invasive preoperative testing. Another algorithm proposed by Ali and colleagues 11 in a prospective study, suggested that an accurate noninvasive evaluation by echocardiography and MRI might select patients who could skip cardiac catheterization. Fogel and colleagues 19 concluded that cardiac catheterization in routine cases adds little clinically relevant information but it should be used in the assessment of patients whose noninvasive evaluations were equivocal or demonstrated deterioration or the need for intervention; echocardiography and MRI should be the mainstay of cardiac imaging in the routine evaluation of Fontan patients with single ventricles. Timely staged palliation in the current surgical era with the rarity of significantly elevated PAP or VFP may be the cause of such a poor relationship between cardiac catheterization hemodynamics and adverse postoperative outcomes. 20
This study was retrospective and is subject to all of the inherent biases that come with this type of investigation. Furthermore, the data obtained by noninvasive angiographic techniques such as MRI or CT are a component of the proposed diagnostic algorithm, and the accuracy of MRI or CT was not directly compared with catheter angiography, although this has been demonstrated previously by several investigators in children with complex congenital heart disease.12–15 Based on our results, we concluded that omission of invasive hemodynamic data obtained by routine pre-Fontan catheterization does not impair the ability to predict adverse postoperative outcomes. Furthermore, noninvasive criteria based on clinical, echocardiographic, and angiographic CT/MRI risk factors can be used as an effective screening tool to identify high-risk subjects in whom pre-Fontan cardiac catheterization is indicated. Catheterization should be reserved for cases in which noninvasive evaluations are equivocal, demonstrate deterioration, or need intervention.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.