
Abstract
Background
This systematic review with meta-analysis sought to determine the efficacy and safety of intramyocardial transplantation of bone marrow stem cells during coronary artery bypass graft surgery on postoperative cardiac functional parameters such as left ventricular ejection fraction and left ventricular end-diastolic volume.
Methods
Medline/PubMed, Embase, Elsevier, Sciences online database, and Google Scholar literature search were searched. The effect sizes measured were risk ratio for categorical variables and weighted mean difference with 95% confidence interval for calculating differences between mean values of baseline and follow-up cardiac functional parameters. A value of p < 0.1 for Q test, or I2 > 50%, indicated significant heterogeneity among studies. The literature search retrieved 2900 studies from screened databases, of which 2866 (98.6%) were excluded and 34 (619 patients) were included for scoping review. The final analysis included 9 studies (335 patients).
Results
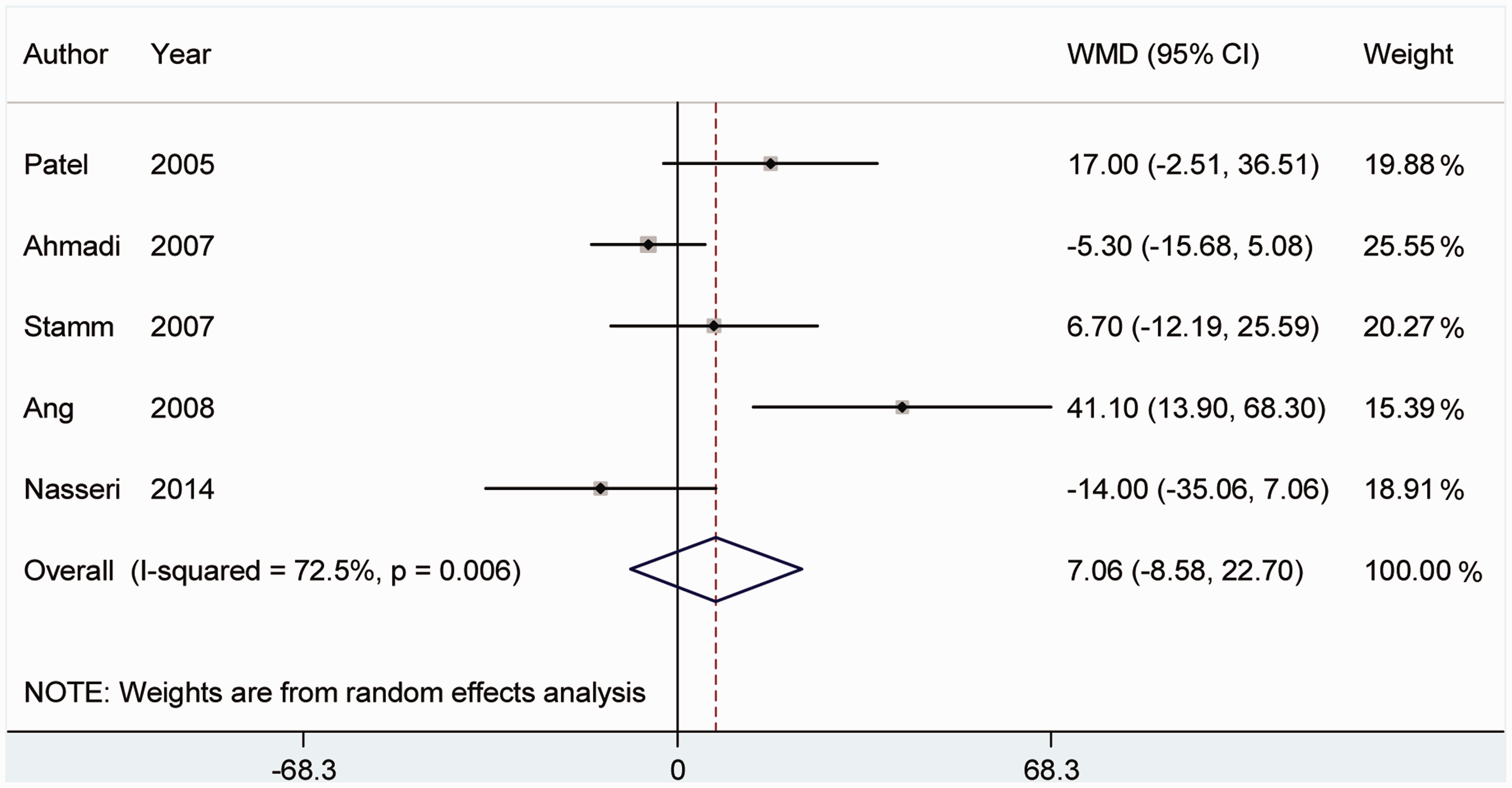
Pooled effects estimates of left ventricular ejection fraction and left ventricular end-diastolic volume showed that bone marrow stem cell transplantation had a weighted mean difference of 4.06 (95% confidence interval: 0.41–7.72; p = 0.02) and 7.06 (95% confidence interval: −8.58–22.7; p = 0.3), respectively.
Conclusions
Intramyocardial transplantation of bone marrow stem cells improves cardiac functional parameters, significantly increasing left ventricular ejection fraction with a nonsignificant reduction in left ventricular end-diastolic volume. Also, this therapeutic method has no life-threatening complications and was therefore found to be an effective and safe method.
Introduction
Ischemic heart disease (IHD) is one of the leading causes of morbidity and mortality worldwide. 1 Currently, interventional revascularization and coronary artery bypass grafting (CABG) constitute the mainstays of treatment of patients with IHD. 1 Despite significant improvement in survival rates after myocardial infarction, impairment of left ventricular function from irreversible loss of cardiomyocytes remains incurable.1,2 On the other hand, the only definitive treatment options, implantation of a mechanical assist device or heart transplantation, are still associated with morbidity and mortality on long-term follow-up.1,2 More than 10 years ago, stem cell applications were introduced for regenerative purposes in cardiovascular surgery. 3 Hematopoietic bone marrow stem cells (BMC) are able to form cardiomyocytes through cell fusion. 3 These cells closely correlate with myocardial regeneration, most likely caused by reduced apoptosis and increased neovascularization.4,5 Recent studies have reported at least 4 mechanisms of the regenerative potential of BMC: cell transdifferentiation from BMC to cardiac myoblasts directly, cytokine-induced myocyte growth, stimulation of endogenous myocardial stem cells, and induction of cell fusion between resident myocytes and transplanted BMC.4–6 Myogenesis and angiogenesis are considered the major mechanisms involved in improving the performance of ischemic myocardium by stem cells.4–6 However, data from randomized controlled trials (RCT) and cohorts are limited and so far largely inclusive. This systematic review with a meta-analysis sought to determine the strength of evidence for intramyocardial transplantation of BMC, including CD133/CD34 and mononuclear BMC (MN-BMC), during CABG surgery to improve cardiac performance parameters such as left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume (LVEDV), and New York Heart Association (NYHA) class.
Methods
A comprehensive search was conducted in Medline/PubMed, Embase, Elsevier, Sciences online database, and Google Scholar from their inception through March 01, 2014, to identify all studies on human subjects and RCT or cohort studies that reported the effects of intramyocardial transplantation of BMC on cardiac functional parameters such as LVEF and LVEDV following CABG. Search terms included: “bone marrow”, “stem cells”, “progenitor cells”, “intramyocardial”, “transplantation” and “cardiac surgery”, “cardiothoracic surgery”, “heart surgery”, “cardiopulmonary bypass”, “CPB”, “coronary artery bypass graft”, “CABG”, “CAB”. There was no language limitation. All references cited in the included studies were also reviewed to determine additional published papers not indexed in common databases.
To review the history of intramyocardial transplantation of CD133, CD34, and MN-BMC stem cells and to provide an overview of past and current studies and reports, the data of 34 studies concerning injection of stem cells into myocardium during CABG were collected. Data retrieved from these investigations included: author, year of publication, study design, number of patients, type of surgery, cell type (CD34, CD133 or MN-BMC), number of cells injected, endpoint measurements such as echocardiographic parameters or magnetic resonance imaging (MRI), and conclusions of the study. All data were presented in a table sorted by year of publication.
Two investigators (S.A-H-S and S.J.M) extracted data separately, and discrepancies were resolved via a consensus standardized abstraction checklist used for recording data in each study. Data retrieved from these investigations included: author, year of publication, geographic location of the study, study design, type of control and treatment groups, cell type (CD34, CD133 or MN-BMC), number of cells injected, inclusion and exclusion criteria, endpoint measurement (echocardiographic parameters, MRI), follow-up duration, number of patients for efficacy and safety follow-up, sample size, mean age, percentage of males, location of myocardial infarction (MI), number of diseased coronary vessels, infarct age, LVEF at baseline and follow-up, LVEF changes from baseline to follow-up for control and treatment groups, LVEDV at baseline and follow-up, LVEDV changes from baseline to follow-up for control and treatment groups, preoperative and postoperative average NYHA classifications. For safety analysis, major adverse cardiovascular events including ventricular arrhythmias and the composite of other serious cardiovascular events such as death, recurrent MI, and stroke were extracted.
Quality assessment of RCT was scored using the Jadad score calculation. 7 The Jadad score has 3 items for calculation of RCT: randomization (0–2 points), blinding (0–2 points), and withdrawals and drop-outs (0–1 point). In the Jadad scale, higher scores indicate better reporting. Studies were enrolled if they met the following criteria: RCT or cohort of human subjects, adult patients undergoing CABG, comparison of CABG alone with intramyocardial injection of BMC in addition to CABG, injection of BMC into ischemic areas of myocardium, and at least 3-months follow-up after injection of BMC. The major exclusion factors were: other types of injection, such as intracoronary and catheter-based-injection methods; stem cell injection during other cardiac surgical procedures; treatment of acute MI; insufficient information on LVEF; cells derived from sources other than bone marrow; and abstracts published without peer-review publication of manuscripts. The primary outcome was the change in LVEF form baseline to follow-up for control and treatment groups. Other outcomes evaluated were LVEDV, NYHA class, and adverse events.
For exploration of sources of probable heterogeneity in studies, we evaluated disparities in characteristics including type of cells injected (CD34, CD133 or MN-BMC), study design (RCT vs. cohort), average age (<65 vs. ≥65 years), percentage of males (<80% vs. ≥80%), mean preoperative LVEF (≥35% vs.<35%), endpoint measurement (MRI vs. echocardiographic parameters), and Jadad score (≤3 vs. >3).
Data were analyzed by STATA version 11.0 software, utilizing METAN and METABIAS modules. The effect sizes measured were risk ratio (RR) for categorical variable and weighted mean difference (WMD) with 95% confidence interval for calculating differences between mean values of LVEF and LVEDV in treatment and control groups. According to a pervious meta-analysis carried out by Donndorf and colleagues,
8
to calculate the changes in LVEF from baseline to follow-up, we used the reported standard deviation (SD) of LVEFBMC changes and LVEFcontrol changes to calculate the correlation coefficients within each group, as described by Stamm and colleagues:
9

The calculation resulted in R = 0.85 for the control group and R = 0.45 for the treatment group. SD of LVEFBMC changes and LVEcontrol changes were calculated by formula:

For analysis of adverse effects, we calculated the relative risk and corresponding standard error using the method of Armitage and colleagues 10 to solve the zero-cells problem. A value of p < 0.1 for Q test or I2 > 50% indicated significant heterogeneity among the studies. The presence of publication bias was evaluated using the Begg and Egger tests. Results were statistically significant at p < 0.05.
Results
The literature search retrieved 2900 studies from screened databases, of which 2866 (98.6%) were excluded after initial review (Figure 1). Of 34 studies included initially, 25 were excluded after detailed evaluation, due to insufficient reporting of endpoints of interest (Figure 1). The final analysis included 9 studies (335 patients; 6 RTC and 3 cohort studies). These RCT and cohorts had 217 (64.7%) and 118 (35.2%) patients, respectively (Figure 1).
Flow chart of included studies.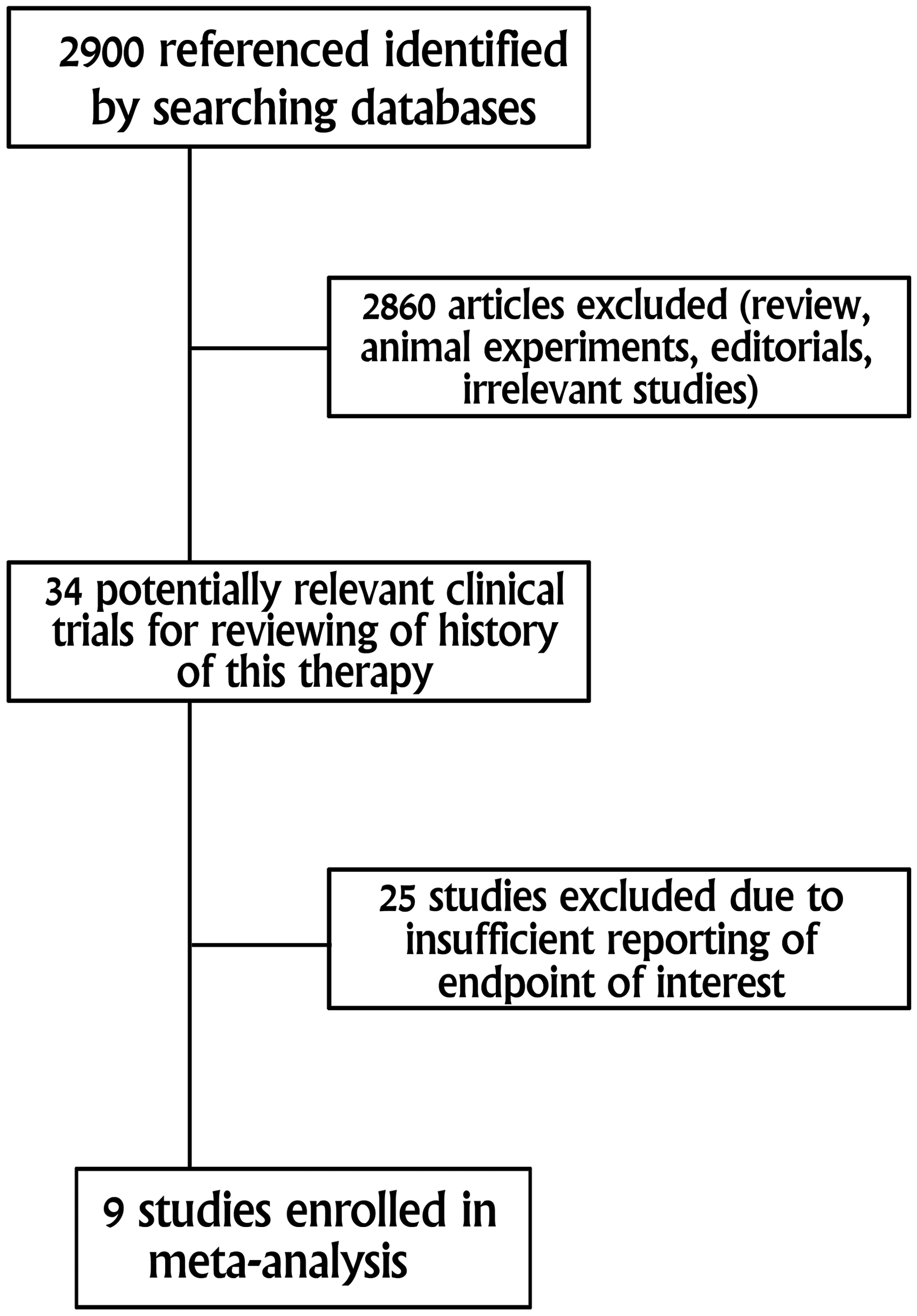
Past and current reports on intramyocardial transplantation of bone marrow stem cells during CABG.

PERFECT phase 3 trial (study protocol for RCT). CABG: coronary artery bypass grafting; CMR: cardiac magnetic resonance; CR: case report; CT: computed tomography; ECG: electrocardiogram; Echo: echocardiography; EF: ejection fraction; 18 F-PET: 18 F-fluorodeoxyglucose positron-emission tomography; LVEF: left ventricular ejection fraction; MN: mononuclear cells; MRI: magnetic resonance imaging; NCT: non-controlled trial; ND: no data; NRCT: non-randomized controlled trial; NYHA: New York Heart Association; RCT: randomized controlled trial; SPECT: single-photon-emission computed tomography; TMLR: transmyocardial laser revascularization.
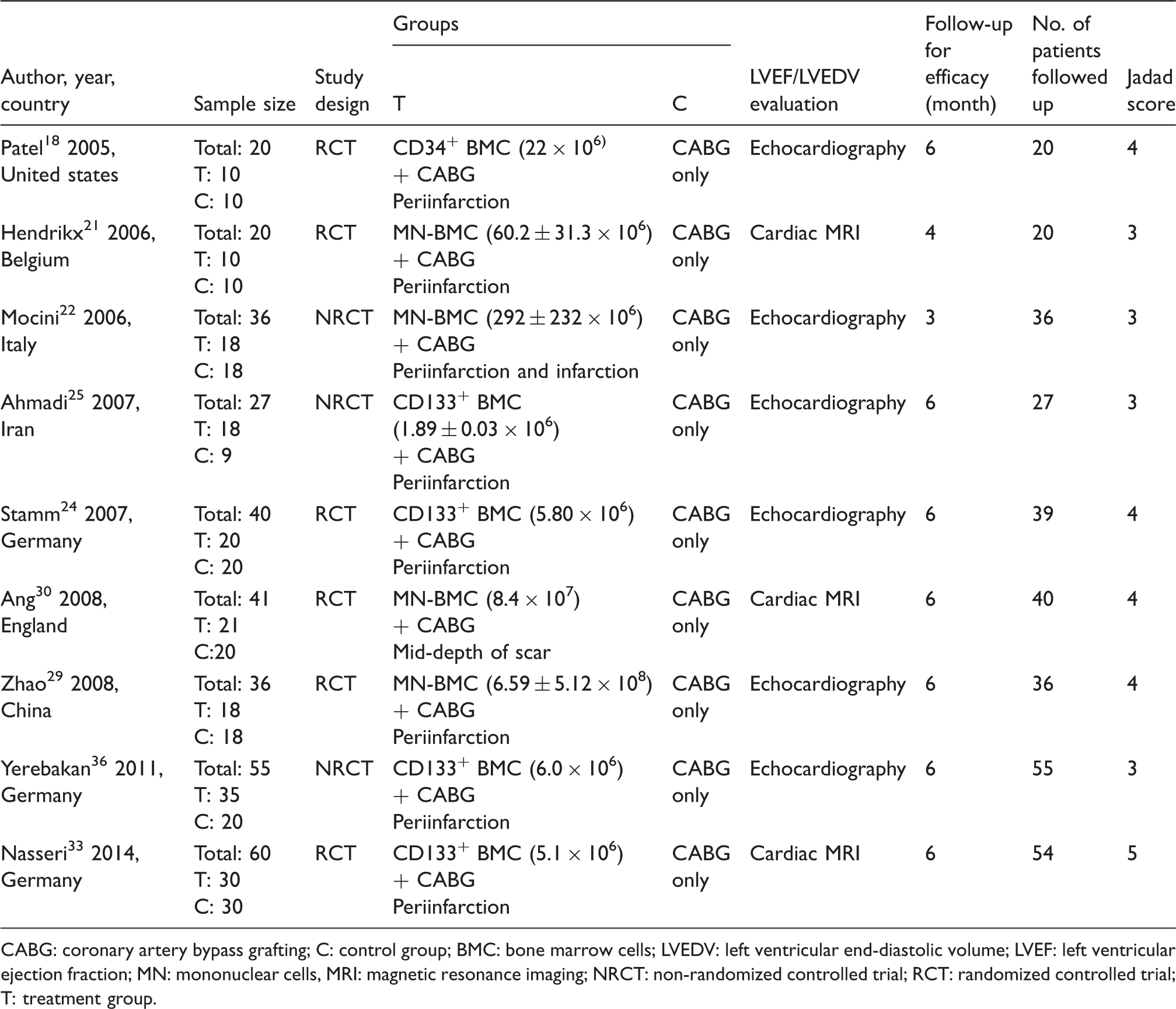
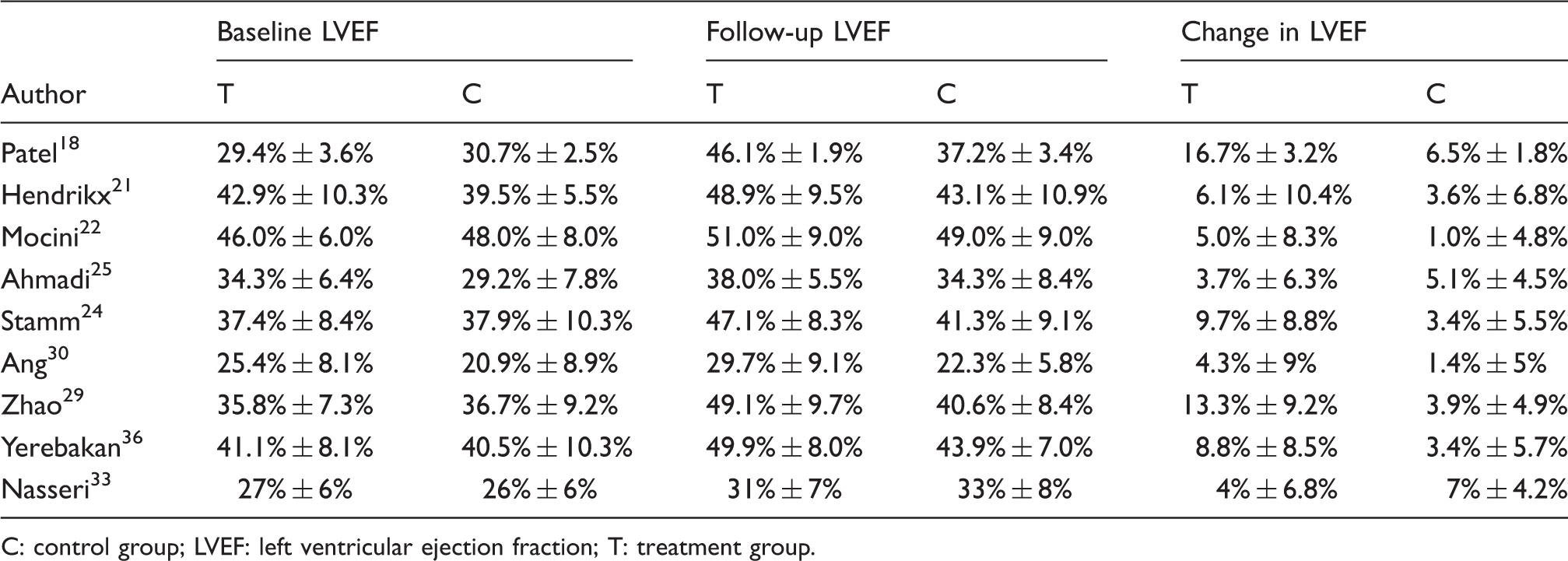
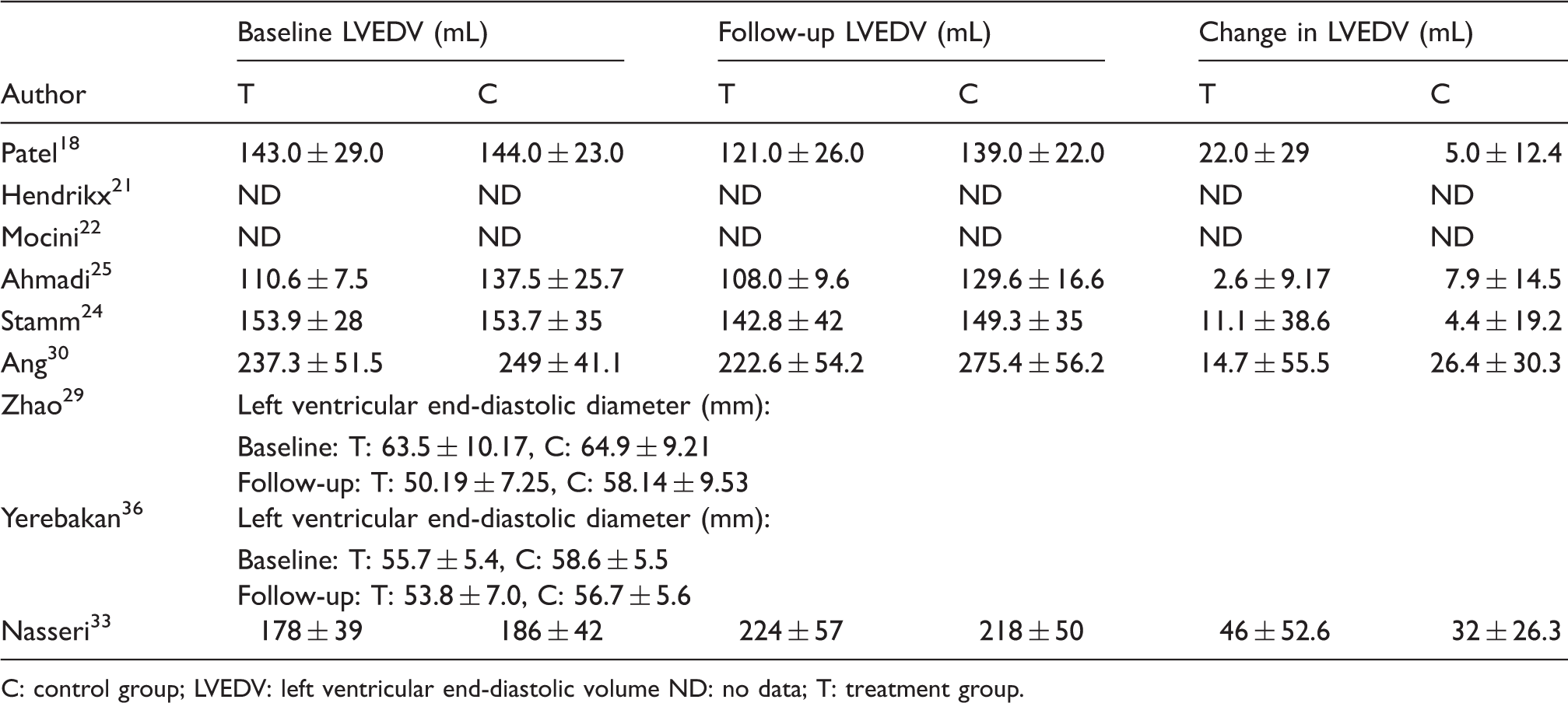
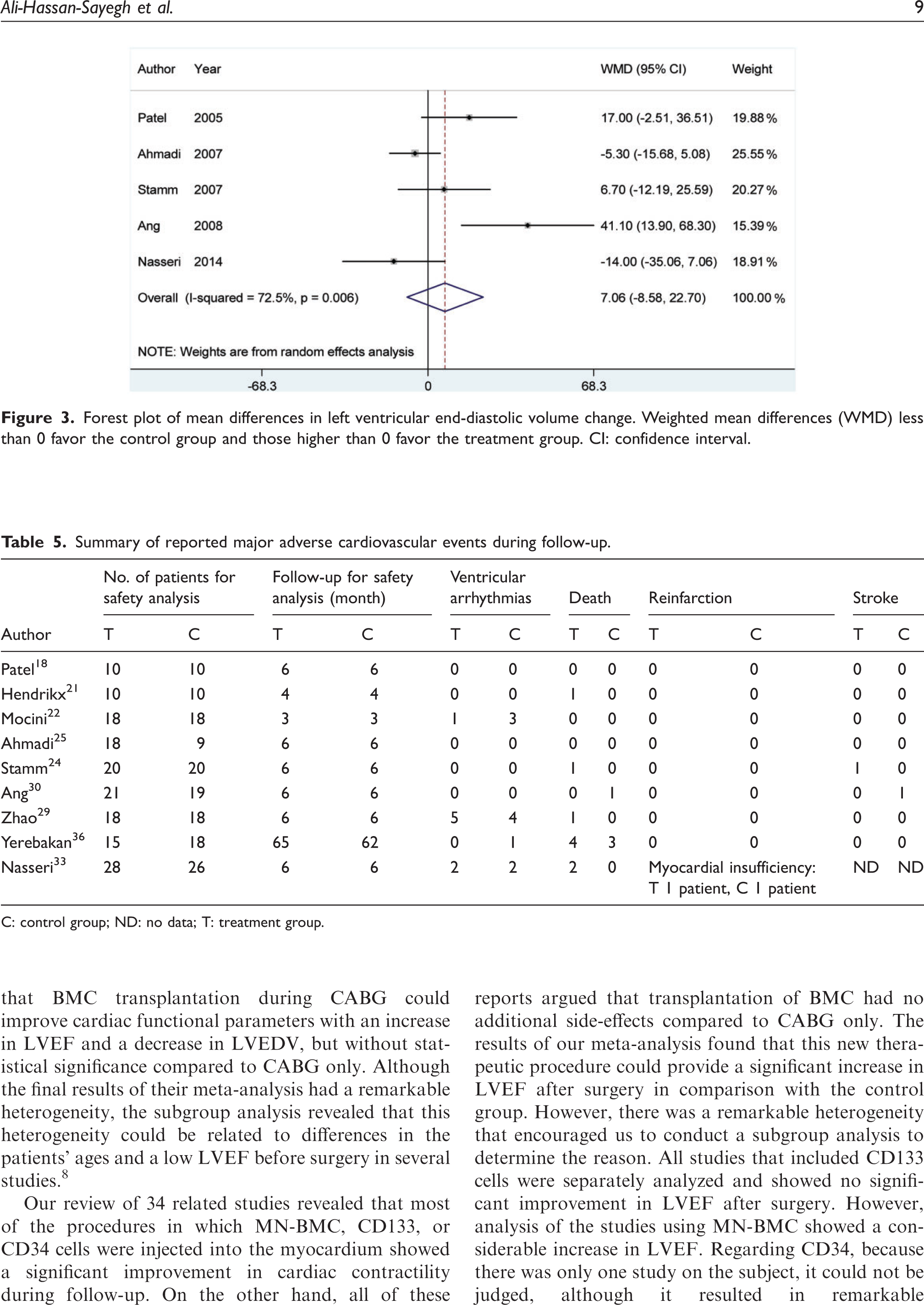
Nine RCT with a total of 335 patients were included in the meta-analysis. Three trials had been conducted in Germany and one each in the United States, United Kingdom, Iran, China, Italy, and Belgium (Table 2). RCT patient populations ranged from 20 to 60 patients with a mean age of 61.7 years (range 49.7–65.6 years), and 83.3% (range 71.6%–94.9%) were males (Supplemental Table 1). Follow-up duration was 3–6 months (median 6 months). Mean preoperative LVEF was 34.85% (treatment group LVEF 35.4%, control group LVEF 34.3%). In the selected studies, LVEF and LVEDV were evaluated by echocardiography (6 studies, 214 patients) and cardiac MRI (3 studies, 121 patients). Eight studies targeted the periinfarction zone for stem cell injection, and 2 targeted injections into the center of the infarcted area. Types of cell injected were CD34 in one study (20 patients), CD133 in 4 studies (182 patients), and MN-BMC in 4 studies (133 patients). All inclusion and exclusion criteria of these studies are presented in Supplemental Table 2. In the treatment group, baseline and follow-up LVEF was 35.23% ± 9.91% and 42.65% ± 11.48%, respectively. The change in LVEF in patients who received BMC was 7.42% ± 8.77%. Baseline and follow-up LVEF in the control group was 33.90% ± 10.75% and 37.83% ± 10.19%, respectively. Mean change in LVEF in patients who underwent CABG only was 3.92% ± 4.87% (Table 3). Pooled treatment effect analysis revealed that BMC therapy plus CABG significantly improved LVEF compared to CABG only, with a WMD of 4.06 (95%CI: 0.41–7.72; p = 0.02, Figure 2) using the random effect model. Significant heterogeneity was observed in these studies (Q test = 62.82, I2 = 87.3%; p < 0.001). Subgroup analysis was performed for exploration of heterogenic agents (Supplemental Table 3). Types of cell and preoperative LVEF were heterogenic agents. Of the 9 studies included in this meta-analysis, 5 reported data on LVEDV. In the treatment group, baseline and follow-up LVEDV was 169.90 ± 178.51 and 175.80 ± 188.25 mL, respectively. The change in LVEDV in patients who received BMC was 5.88% ± 50.96%. Baseline and follow-up LVEDV in the control group was 183.27 ± 181.0 and 197.64 ± 209.33 mL, respectively. The mean change in LVEDV in patients who underwent CABG only was 14.37 ± 32.56 mL (Table 4). Pooled treatment effect analysis revealed that BMC therapy plus CABG had a trend towards a reduction of LVEDV compared to CABG only, with WMD of 7.06 (95% CI: −8.58–22.7; p = 0.3; Figure 3) using the random effect model; however, this effect did not reach statistical significance. Significant heterogeneity was observed among studies (Q test = 14.56, I2 = 72.5%; p = 0.006). Subgroup analysis was performed for exploration of heterogenic agents in LVEDV studies (Supplemental Table 3). Data on NYHA class before and after surgery are presented in Supplemental Table 4. All included studies had good methodological quality (mean Jadad score 4, range 3–5; Table 2). In addition, Beeg’s and Egger’s tests showed no publication bias among the included studies: Begg’s test, p = 0.297; Egger’s test, p = 0.055. Pooled analysis (Table 5) showed no significant differences in ventricular arrhythmias and the composite of death, recurrent MI, and stroke between groups [(RRVA: 0.78; 95%CI: 0.34–1.8; p = 0.9), (RRComposite: 0.85; 95%CI: 0.36–1.9; p = 1.0)].
Forest plot of mean differences in left ventricle ejection fraction change. Weighted mean differences (WMD) less than 0 favor the control group and those higher than 0 favor treatment group. Forest plot of mean differences in left ventricular end-diastolic volume change. Weighted mean differences (WMD) less than 0 favor the control group and those higher than 0 favor the treatment group. CI: confidence interval. Principal characteristics of included studies. CABG: coronary artery bypass grafting; C: control group; BMC: bone marrow cells; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; MN: mononuclear cells, MRI: magnetic resonance imaging; NRCT: non-randomized controlled trial; RCT: randomized controlled trial; T: treatment group. Treatment results of studies included in the meta-analysis: left ventricuular ejection fraction. C: control group; LVEF: left ventricular ejection fraction; T: treatment group. Treatment results of studies included in the meta-analysis: left ventricular end-diastolic volume. C: control group; LVEDV: left ventricular end-diastolic volume ND: no data; T: treatment group. Summary of reported major adverse cardiovascular events during follow-up. C: control group; ND: no data; T: treatment group.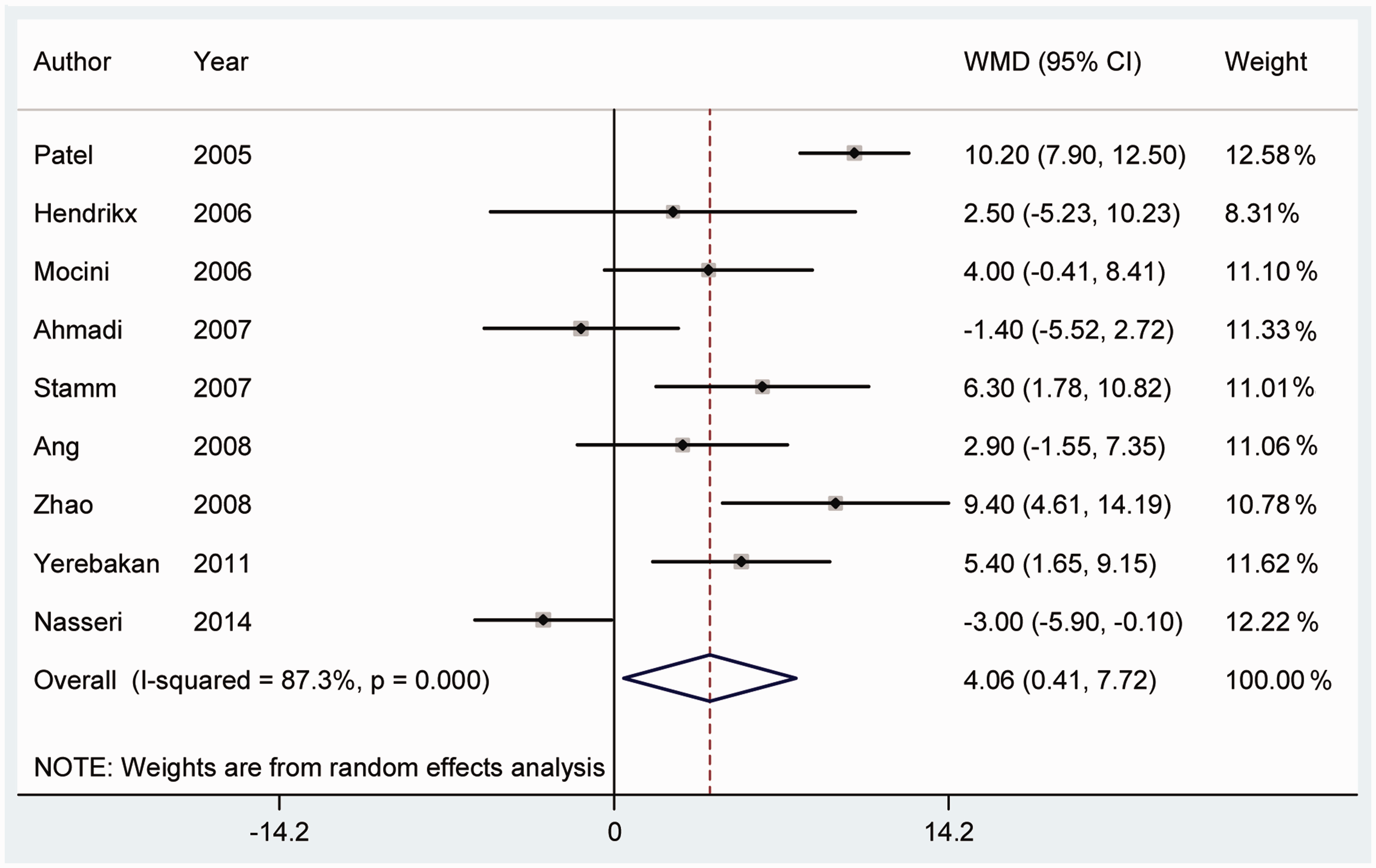
Discussion
In recent decades, a considerable number of studies have investigated the effects of intramyocardial transplantation of BMC during CABG surgery. Most have claimed that this new therapy improves left ventricular function and perfusion, with no significant side-effects. In a meta-analysis, Donndorf and colleagues 8 reviewed 6 studies including 2 cohorts and 4 RCT. They found that BMC transplantation during CABG could improve cardiac functional parameters with an increase in LVEF and a decrease in LVEDV, but without statistical significance compared to CABG only. Although the final results of their meta-analysis had a remarkable heterogeneity, the subgroup analysis revealed that this heterogeneity could be related to differences in the patients’ ages and a low LVEF before surgery in several studies. 8
Our review of 34 related studies revealed that most of the procedures in which MN-BMC, CD133, or CD34 cells were injected into the myocardium showed a significant improvement in cardiac contractility during follow-up. On the other hand, all of these reports argued that transplantation of BMC had no additional side-effects compared to CABG only. The results of our meta-analysis found that this new therapeutic procedure could provide a significant increase in LVEF after surgery in comparison with the control group. However, there was a remarkable heterogeneity that encouraged us to conduct a subgroup analysis to determine the reason. All studies that included CD133 cells were separately analyzed and showed no significant improvement in LVEF after surgery. However, analysis of the studies using MN-BMC showed a considerable increase in LVEF. Regarding CD34, because there was only one study on the subject, it could not be judged, although it resulted in remarkable improvements in cardiac functional parameters. These findings suggest that injection of MN-BMC might lead to better clinical outcomes compared to CD133 and CD34. We assumed that the heterogeneity was due to including cohorts in the meta-analysis along with RCT. Therefore, RCT and cohorts were analyzed separately. It was concluded that RCT tended to be heterogeneous even without considering the cohorts, thus the cohorts were not the cause of heterogeneity. The studies were analyzed regarding the percentage of males less than or more than 80%. This revealed that studies with a male sex proportion >80% showed a better response to treatment. This infers that injection of BMC cells might lead to better outcomes in men compared to women, hence the need for further investigations. One of the effective factors in the heterogeneity of our results was LVEF before surgery; studies with a mean LVEF >35% showed significant improvement in cardiac functional parameters following BMC transplantation compared to those with a mean LVEF <35%. Therefore, it can be assumed that severe disorders affecting left ventricular function might reduce the quality of the response to treatment. For this reason, it might be necessary to inject more cells into a larger area of scared myocardium. Another difference between studies was related to the tools used for assessment of cardiac function; thus studies that used MRI and echocardiography were separately analyzed. The results showed that studies using echocardiographic assessment showed significant improvement in cardiac functional parameters, while those using MRI did not report such an improvement. According to the results of our meta-analysis, we can claim that in general, intramyocardial transplantation of BMC during CABG leads to a significant increase in LVEF.
The previous meta-analysis by Donndorf and colleagues 8 pointed out that transplantation of BMC resulted in a trend towards decreasing LVEDV compared to the control group. We assessed LVEDV in our meta-analysis, and in line with the previous review, no significant difference was detected in LVEDV changes between the treatment and control groups. Subgroup analysis was again performed to determine the effective factors on LVEDV results. Three studies on CD133 were separately analyzed, indicating that CD133 did not significantly decrease LVEDV. CD34 and MN-BMC were each the focus of a single study and were found to decrease LVEDV significantly. However, because the number of studies was not enough for meta-analysis, it is not possible to make a definitive judgment. Regarding the tools used for measurement of LVEDV, the studies were divided into two groups based on radiological assessment: MRI or echocardiography. Both tools suggested that BMC did not have a significant effect on LVEDV changes. Our findings indicate that patients receiving BMC during CABG would probably be in a better condition in terms of NYHA class compared to those undergoing CABG only. One of the most striking issues addressed in our meta-analyses and that of Donndorf and colleagues 8 was evaluation of the complications of BMC transplantation. Both studies concluded that ventricular arrhythmia and a composite of major adverse effects including recurrent MI, stroke, and death, were not significantly different in the treatment and control groups; therefore, intramyocardial transplantation of BMC might be considered a safe treatment.
In terms of the follow-up period, we should consider that most of the studies had short-term follow-up (3–6 months) and few had long-term follow-up. However, Ahmadi and colleagues 44 indicated that transplantation of BMC resulted in remarkable improvements in LVEF and cardiac function after short-term follow-up, whilst in long-term follow-up of 5 years, there was no difference between patients who underwent transplantation of BMC during CABG and those who had CABG only. 44 Nevertheless, on long-term follow-up, no complications such as ventricular arrhythmia, recurrent MI, stroke, or death were reported after BMC. 44 Similarly, Yerebakan and colleagues 36 showed that during a 6-month-follow-up, the BMC receivers had better cardiac function compared to the control group; however, in long-term follow-up, no difference was detected between the two groups. Although the insufficient number of studies with long-term follow-up results makes it impossible to comment on the long-term effects of BMC transplantation, the available evidence suggests that this new therapeutic procedure might lead to cardiac function improvement in a discrete period of time after surgery. Recently, Tian and colleagues 45 evaluated the effects of intramyocardial injection of BMC in patients with IHD, and found that this treatment significantly increased LVEF and decreased LVEDV, recommending it for patients with IHD undergoing revascularization.
Reviewing the literature, a considerable number of researchers believe that transplantation of BMC may lead to an improvement in contractility and myocardial perfusion, and increased LVEF, with no serious complications. Therefore, intramyocardial transplantation of BMC during CABG surgery was found to be a safe and feasible procedure introduced into cardiac surgery in recent decades. It was concluded that myocardial transplantation of BMC improves cardiac functional parameters, significantly increasing LVEF, with a trend towards decreasing LVEDV. Also, this therapeutic method has no life-threatening complications and was therefore found to be effective and safe. Further studies with larger sample sizes and longer follow-up periods might provide better insight for cardiac surgeons into this new method, thus confirming it with more confidence in the near future. One of the most important aspects in terms of implementation of BMC treatment into routine clinical practice and future perspectives is further development of the research environment and infrastructure to facilitate scientific interactions between multidisciplinary basic and clinical scientists and clinicians. This translational bridge between basic and biomedical research and medical healthcare, with involvement of infrastructure, development of stem cell registries, and stem cell banks, seems to be a key point for the routine implementation of stem cell treatment in patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.