
Abstract
Background
Although spontaneous hemopneumothorax is rare, emergency surgery may be necessary if massive bleeding is present.
Methods
We examined therapeutic strategies and outcomes as well as background factors in 16 patients with spontaneous hemopneumothorax treated at our hospital between April 2002 and August 2013.
Results
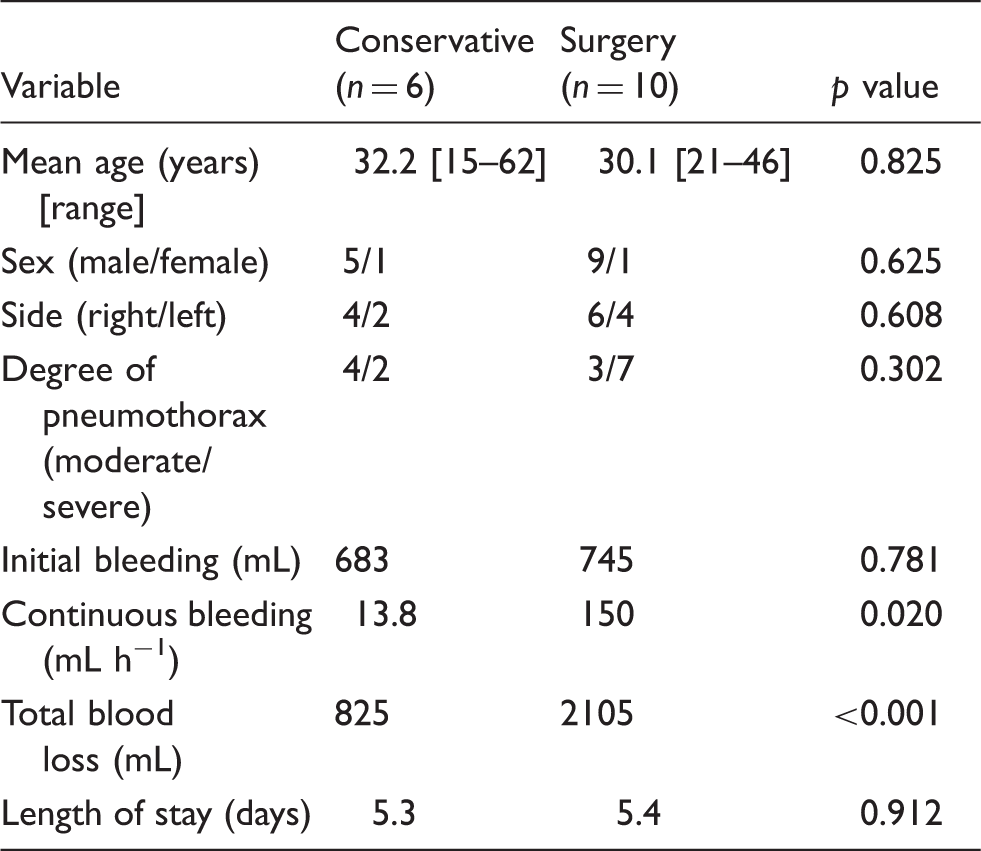
Emergency surgery was performed in 3 patients, all of whom were hemodynamically unstable. Elective surgery was performed in 7 patients, all of whom showed continuous bleeding from a pleural cavity drain. The surgery consisted of intrapleural hematoma removal, hemostasis, and bullectomy; 3-port thoracoscopy was used in all of the surgical cases. Six patients, none of whom showed continuous bleeding, recovered with conservative therapy. Comparing the conservative therapy and surgery groups revealed the mean continuous bleeding volume and total blood loss to be significantly greater in the latter, but no significant difference was noted between the two groups in terms of the initial bleeding volume following tube thoracostomy. None of the cases required a blood transfusion.
Conclusions
Spontaneous hemopneumothorax is not necessarily an indication for surgery, and even when the initial volume of blood drained through the chest tube is large, some patients can still be treated conservatively with careful monitoring of vital signs and continuous bleeding volumes. However, it is important not to miss the optimal timing of surgery in order to avoid administering unnecessary blood transfusions to young patients.
Introduction
Spontaneous hemopneumothorax (SHP) is rare, accounting for only 1%–12% of spontaneous pneumothorax cases.1–3 However, it is often life-threatening because of the associated hypovolemic shock. We herein report 16 SHP patients and discuss their clinical features, management, surgical findings, and outcomes.
Patients and methods
From April 2002 through August 2013, 930 patients with spontaneous pneumothorax were treated in the Yokohama Rosai Hospital. Of these patients, 16 (1.7%) developed SHP; there were 14 males and 2 females, ranging in age from 15 to 62 years (mean age 30.9 years). In this study, SHP was defined as the accumulation of more than 400 mL of blood in the pleural cavity, based on the criteria of Ohmori and colleagues. 4 All patients initially underwent a closed thoracostomy and we closely monitored their vital signs as well as determining the initial and continuous bleeding volumes after tube thoracostomy. In one group, designated the emergency surgery group, we decided to perform surgery immediately after tube thoracostomy. In the elective surgery group, surgery was performed several hours after the thoracostomy procedure. The remaining patients comprised the conservative therapy group.
We analyzed clinical outcomes to make comparisons among these 3 groups. The independent t test and chi-square test were used for two-group comparisons. A value of p < 0.05 was considered to indicate a statistically significant difference.
Results
Clinical characteristics of 16 patients with spontaneous hemopneumothorax.
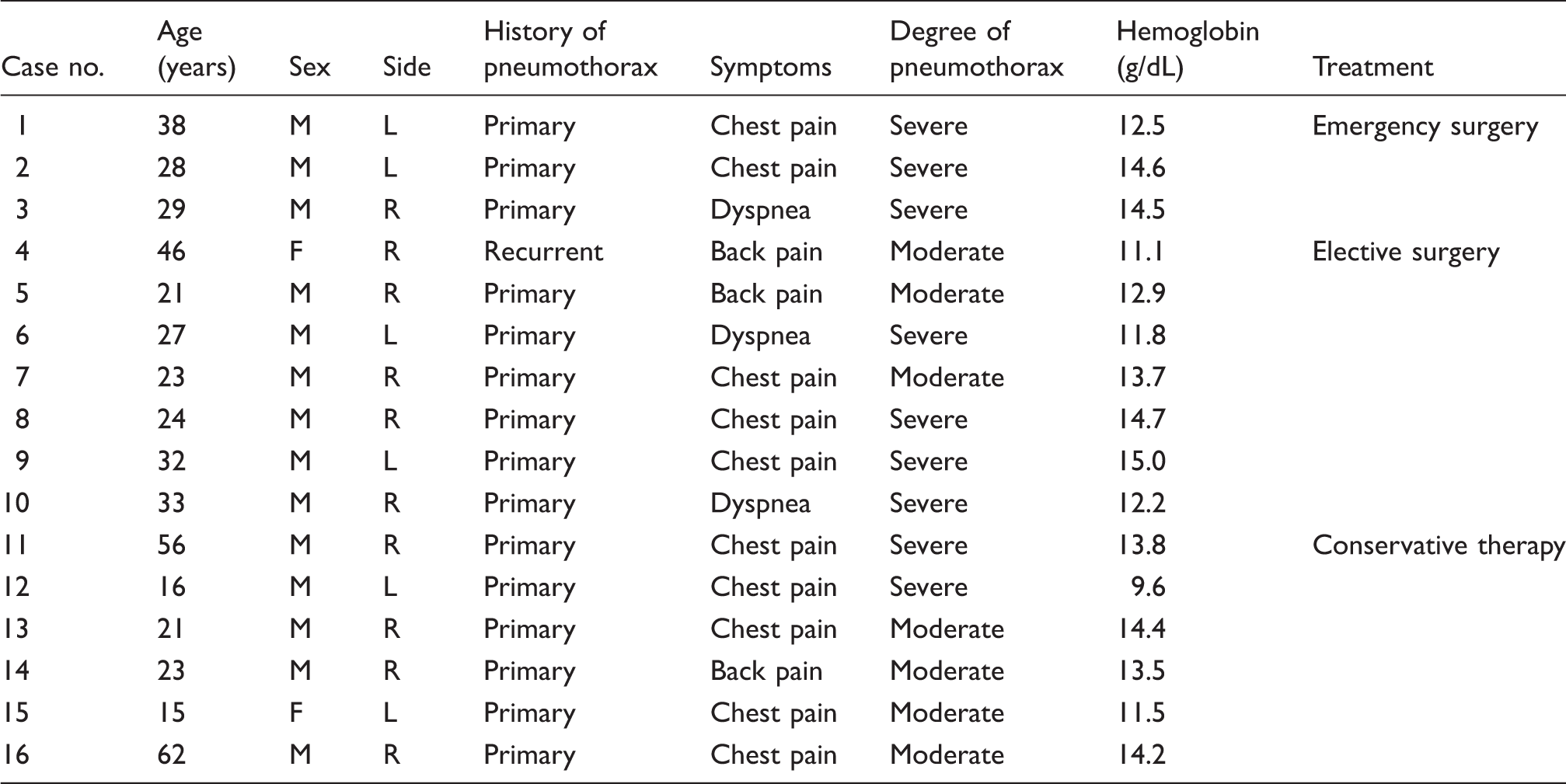
Emergency surgery group.

MinHb: minimum hemoglobin.
Elective surgery group.
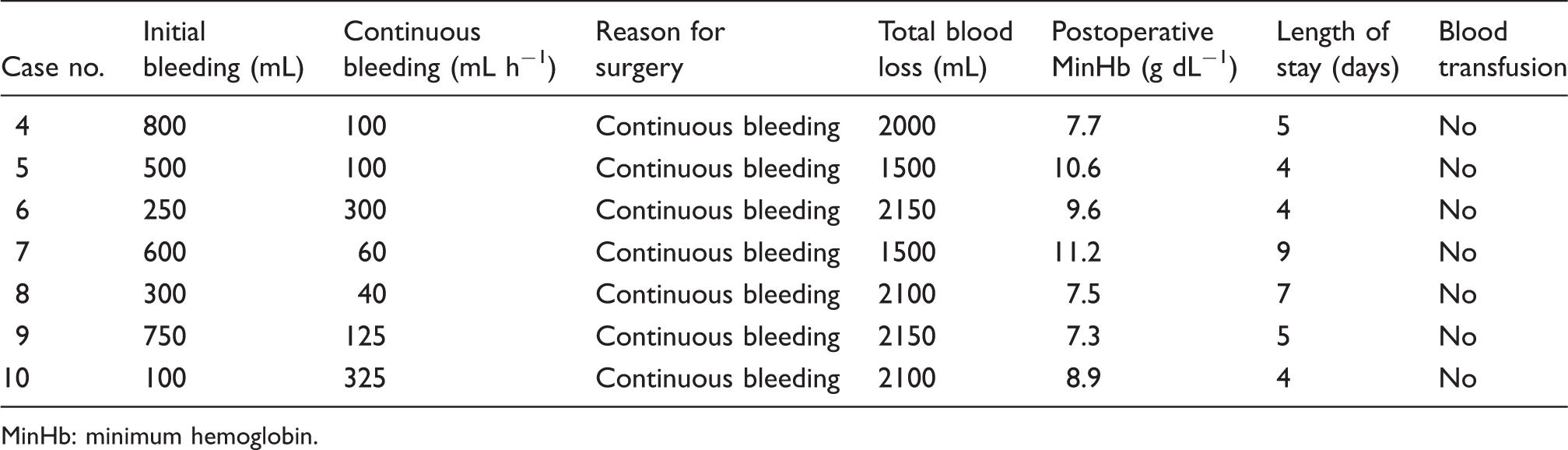
MinHb: minimum hemoglobin.
Conservative therapy group.
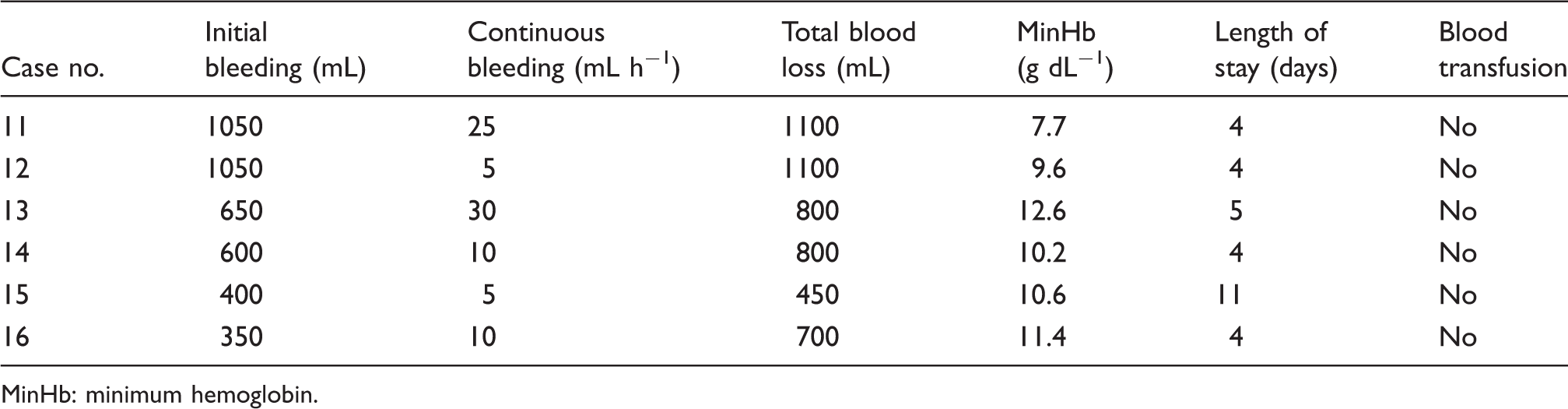
MinHb: minimum hemoglobin.
Comparison of patients undergoing conservative therapy and surgery for spontaneous hemopneumothorax.
Discussion
SHP is a rare clinical disorder that can progress to hemorrhagic shock, a condition requiring emergency surgery.6,7 The mechanisms underlying the development of SHP include a torn pleural adhesion between the parietal and visceral pleura resulting from tearing of congenital aberrant vessels between the parietal and visceral pleura, or bleeding from rupture of vascularized bullae and the underlying lung parenchyma.4,7–11 In our study, bleeding from the parietal pleura was found in 9 patients and bleeding from the lung parenchyma in one (case no. 5).
Generally, in surgery for spontaneous pneumothorax, it is not uncommon to find a firm adhesion between the apex of the lung and the parietal pleura. Were the vessels of the pleural adhesion band to be torn when the lung underwent major collapse, the patient would be at risk of massive blood loss. Regarding treatment, there are many reports recommending early surgical intervention for conservatively managed patients due to potential complications such as atelectasis, restrictive lung disorders, and infection of residual hematoma.1,2 In this study, we decided to perform emergency surgery when patients experienced hemodynamic instability. In patients who remained hemodynamically stable, we carefully observed the amounts of continuous bleeding and total bleeding, as well as monitoring changes in vital signs. Based on these observations, we decided whether or not surgery was indicated. It is important to perform surgery for SHP at the appropriate time because SHP usually occurs in the young and it is advisable to avoid unnecessary blood transfusions in such patients. All 6 patients managed by closed thoracostomy alone were discharged from the hospital without atelectasis, restrictive lung disorders, or hematoma infection. This suggests that the presence of blood clots is not necessarily an indication for surgery, and that blood clots might be spontaneously absorbed, allowing full resolution of SHP. However, if a large hematoma remains in the pleural cavity, this hematoma may prevent the lung from expanding a few weeks after the onset of SHP. 4 Therefore, we advocate surgery even in cases where complete hemostasis is achieved.
We suggest that surgery is indicated if there are signs of hypovolemic shock, continuous bleeding (>100 mL h−1), persistent air leak, and/or impaired lung expansion because of a large hematoma in the pleural cavity. Even in cases with small amounts of bleeding, surgery may also be indicated if the bleeding continues, and as a result, the total blood loss is anticipated to be large. However, it is important to note that SHP is not an absolute indication for surgery. As shown in Table 4, some of our patients recovered with conservative therapy, despite the initial bleeding volume after drain placement being as large as 1050 mL, and the hospital stays of such patients did not differ from those undergoing surgery. We prefer VATS to thoracotomy because VATS allows easy access to the bleeding site. As to the problem of blood clot removal through a port incision, we use specimen retrieval bags. We advocate VATS as a minimally invasive procedure for SHP because postoperative pain is reduced, allowing shorter hospitalization. 13
We concluded that for managing SHP, surgery should be performed in the early stage in patients who are hemodynamically unstable or show continuous bleeding from a pleural cavity drain. There are some patients who respond well to conservative therapy with careful monitoring of vital signs and the amount of bleeding from a pleural cavity drain. However, it is important not to miss the optimal timing of surgery in order to avoid administering unnecessary blood transfusions. VATS facilitated the identification of bleeding sites, thereby allowing safe and minimally invasive treatment.
Part of this manuscript was presented at the 114th Annual Congress of the Japan Surgical Society, April 3, 2014, Kyoto, Japan.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.