
Abstract
Supravalvular aortic stenosis as a late complication of transposition of the great arteries is very rare, and only a few cases have been reported. We describe the case of a 14-year-old girl who developed supravalvular aortic stenosis as a late complication of the arterial switch operation for transposition of the great arteries. The narrowed ascending aorta was replaced with a graft. The right pulmonary artery was transected to approach the ascending aorta which adhered severely to the main pulmonary trunk, and we obtained a good operative field.
Keywords
Introduction
The arterial switch operation (ASO) for type I or II transposition of the great arteries became the mainstream anatomical repair during the mid-1980s and has shown stable outcomes. Recently, numerous studies have reported the long-term outcomes of the ASO, with pulmonary artery stenosis, aortic insufficiency, and coronary artery events as late complications. However, neoaortic stenosis after ASO is uncommon.1,2 We describe a case of supravalvular aortic stenosis (SVAS) after ASO in a young female who had undergone reconstructive surgery.
Case report
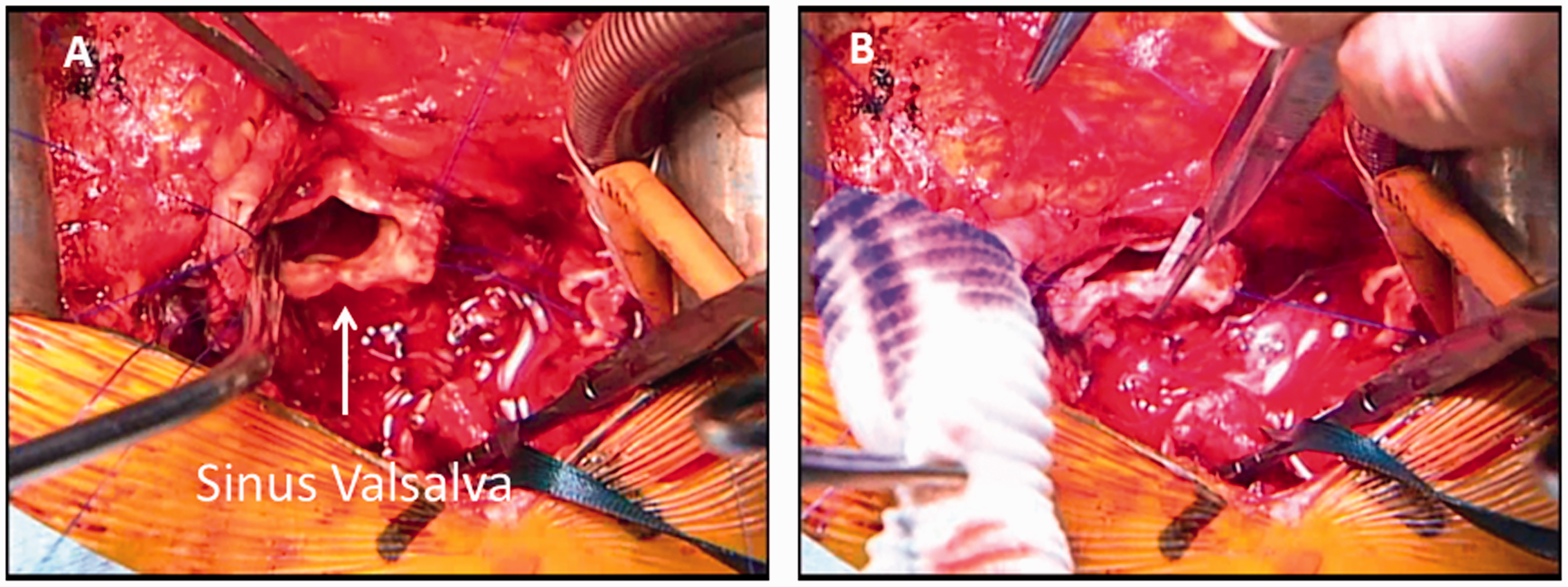
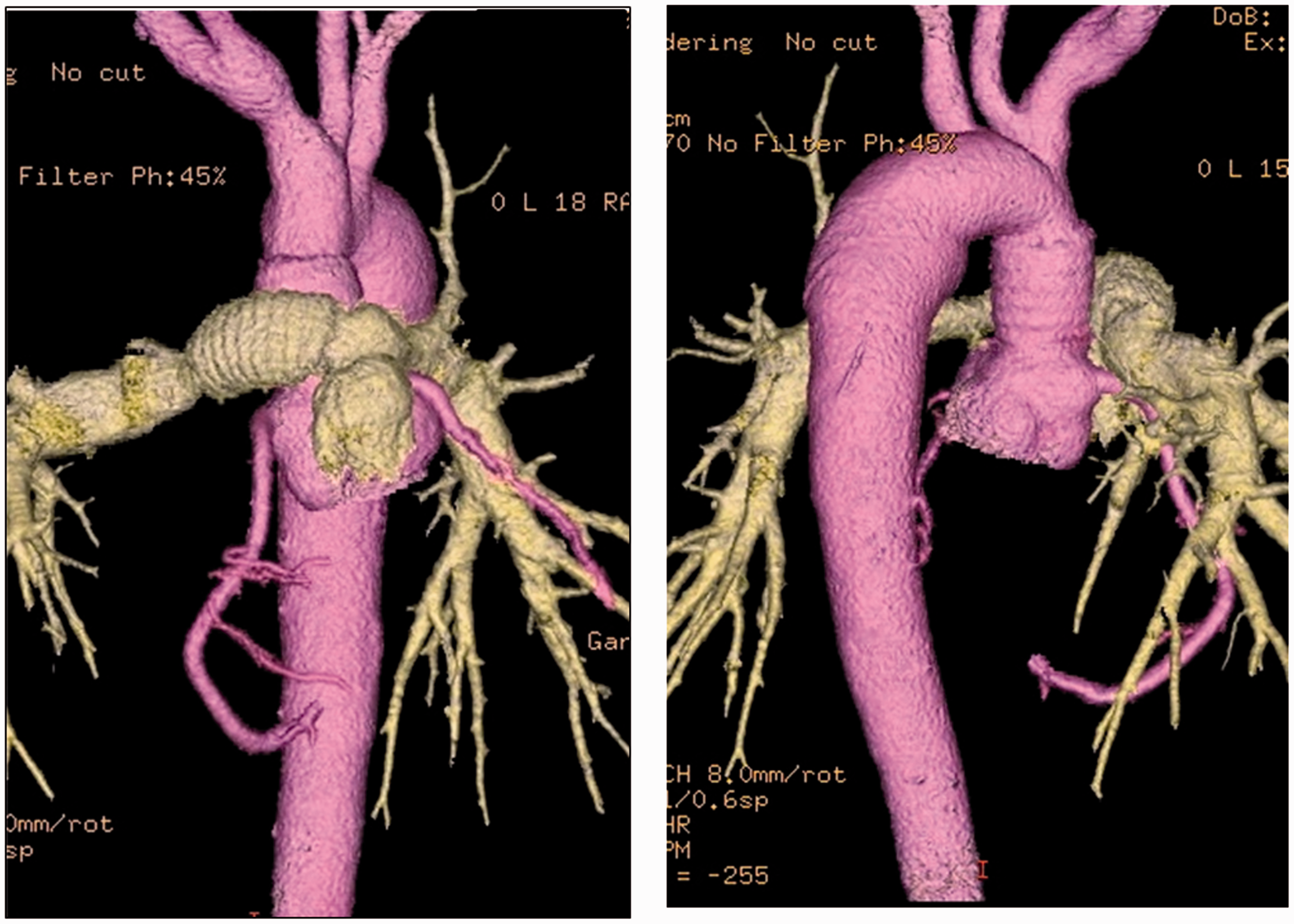
A 14-year-old girl had been diagnosed with type I complete transposition of the great arteries at birth, and underwent ASO at 16 days of age. At 4 years of age, cardiac catheterization showed SVAS with a pressure gradient of 20 mm Hg. Dyspnea on exertion appeared 1 year prior to this admission. Physical examination showed height 1.55 m, weight 50.2 kg, and auscultation revealed a grade 4/6 ejection systolic murmur. Aortography showed severe SVAS with a pressure gradient of 67 mm Hg between the left ventricle and descending aorta. Preoperative computed tomography showed the dimensions of the sinus Valsalva (28 × 30 mm), SVAS site (9 × 8 mm), and aortic arch (19 × 17 mm). The main pulmonary artery (MPA) trunk was just before the neoaorta as a result of the Lecompte maneuver (Figure 1). Because tenacious adhesions were expected, cardiopulmonary bypass was established with cannulation through the femoral vessels. After a resternotomy, the superior vena cava was cannulated. The adhesions between the MPA and neoaorta were so severe that we transected the right pulmonary artery at its origin. An aortic crossclamp was placed distally to accommodate a space for aortic replacement. We transected the ascending aorta at a narrowed segment, and the aorta was longitudinally incised toward the noncoronary cusp. An additional longitudinal incision was made toward the commissure between the right and left coronary cusps to accommodate the size of an adult ascending aorta (Figure 2A). An artificial graft (18-mm J-Graft) was trimmed to make two scallops on the anterior and dorsal sides, and anastomosed to the proximal side of the ascending aorta so that the scallops corresponded to the incisions (Figure 2B). During anastomosis of the distal side, we used deep hypothermic circulatory arrest with retrograde cerebral perfusion. Because the right pulmonary artery trunk could not be anastomosed to the MPA directly, we reconstructed it using an artificial graft (14-mm J-Graft). Postoperative computed tomography revealed a smooth configuration of the ascending aorta with an adult size (Figure 3). A postoperative echocardiogram showed a maximum pressure gradient of 10 mm Hg at the ascending aorta.
Preoperative computed tomography showing the main pulmonary artery trunk (MPA) just before the neoaorta. LCC: left coronary cusp; NCC: noncoronary cusp; RCC: right coronary cusp; SVAS: supravalvular aortic stenosis. Operative photographs: (A) the ascending aorta was longitudinally incised toward the sinus of Valsalva, and the narrow segment was enlarged; (B) the artificial graft was trimmed to make two scallops on the anterior and dorsal sides. Postoperative computed tomography showing that the supravalvular aortic stenosis was well repaired using the artificial graft. The transected right pulmonary artery was also reconstructed with an artificial graft.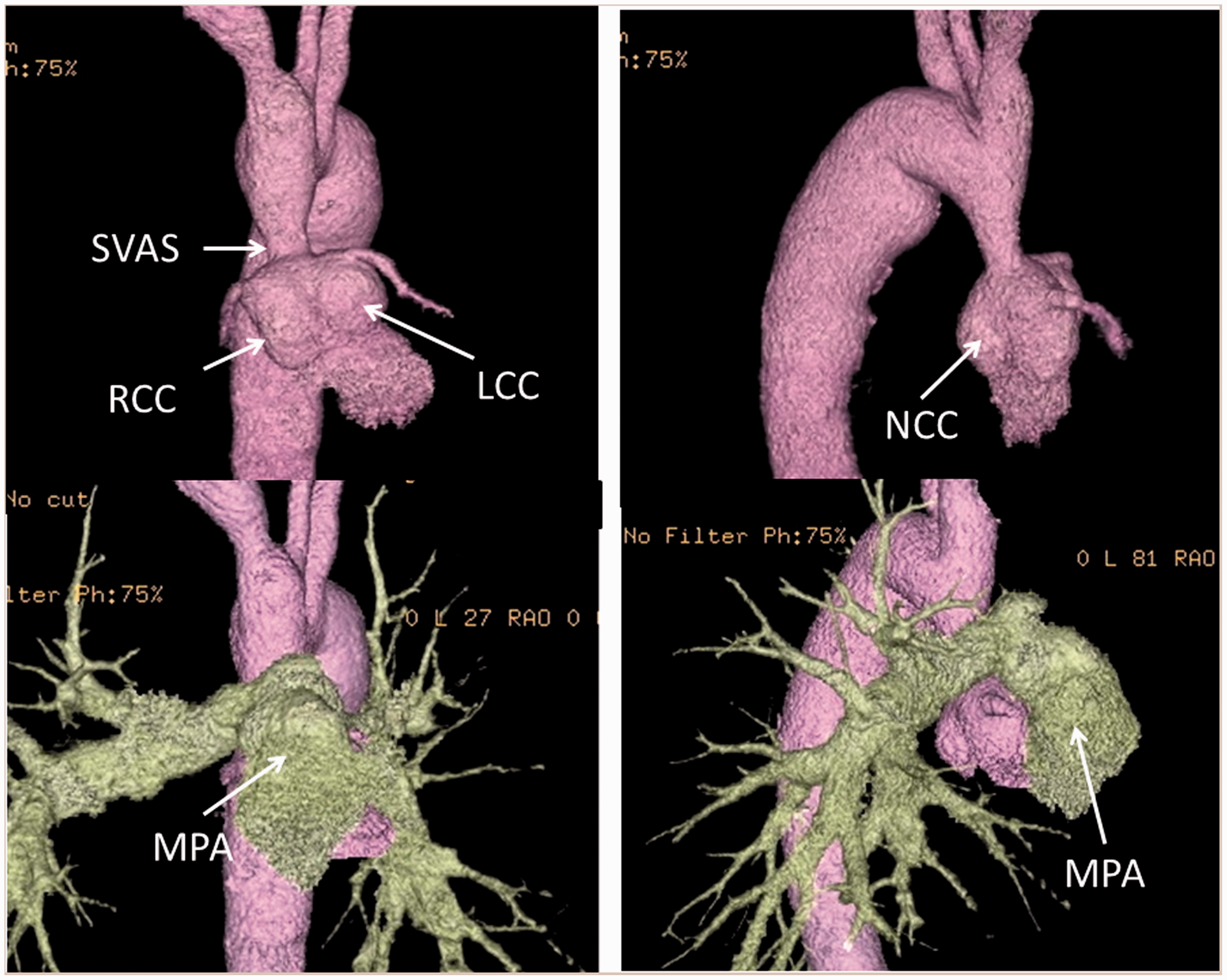
Discussion
Oda and colleagues 2 and Williams and colleagues 3 reported that the reoperation rate for SVAS after ASO was 0.7%–1.3%. Bové and colleagues 4 reported that 4 of 93 post-ASO patients had a gradient across the reconstructed sinotubular junction. They reported a discrepancy in the pulmonary-to-aortic annular size and a ventricular septal defect before the ASO, which strongly correlated with the risk of late neoaortic stenosis. Fujimoto and colleagues 5 reported a case of SVAS in the acute phase following ASO; they speculated that tissue overgrowth resulting from the use of continuous absorbable suture was the main cause of stenosis. We chose continuous nonabsorbable sutures because an excessive tissue response is difficult to achieve. In addition, in several primitive cases, we reinforced the adventitia around the anastomotic site, using single interrupted nonabsorbable sutures. We speculate that the nonabsorbable sutures in the adventitia caused hypoplasia of the anastomotic site. Currently, we do not use single interrupted nonabsorbable sutures, to prevent hypoplasia. In our institution, we have performed 31 ASO procedures, but only this case was complicated with SVAS. Furthermore, since the mild stenosis site did not grow enough in childhood and reached relative stenosis, some other hemodynamic etiology may be present. Two methods were considered as an approach for the neoaorta after the Lecompte maneuver: transection of the MPA, and transection of the right or left pulmonary artery. We chose the latter and obtained a good wide field from the sinus of Valsalva to the distal side of the narrow segment of the neoaorta. To release the SVAS, reconstruction with an artificial graft as well as repair using autologous tissue (e.g. Myers’ technique) or patch expansion were considered. 6 Selection of the repair method is affected by the patients’ age, and because this patient was near adult size, we chose reconstruction with an artificial graft.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.