
Abstract
Background
Chronic pulmonary regurgitation is common after repair of tetralogy of Fallot. Despite the deleterious effects of chronic pulmonary regurgitation on right ventricular function, many patients with repaired tetralogy of Fallot remain asymptomatic. Health is defined not only by the absence of disease but also by physical, mental, and social wellbeing. We sought to examine the impact of pulmonary valve replacement on quality of life in asymptomatic patients with repaired tetralogy of Fallot and chronic pulmonary regurgitation.
Methods
From January 2009 to December 2012, 25 (18 male) asymptomatic patients (mean age 23.4 ± 7.4 years) who underwent pulmonary valve replacement for significant pulmonary regurgitation were recruited. Cardiac magnetic resonance was performed pre- and postoperatively. Quality of life was assessed using the Chinese version of the SF-36v2 evaluation tool. Demographics, clinical data, magnetic resonance findings, and quality-of-life scores were collected and calculated for comparison.
Results
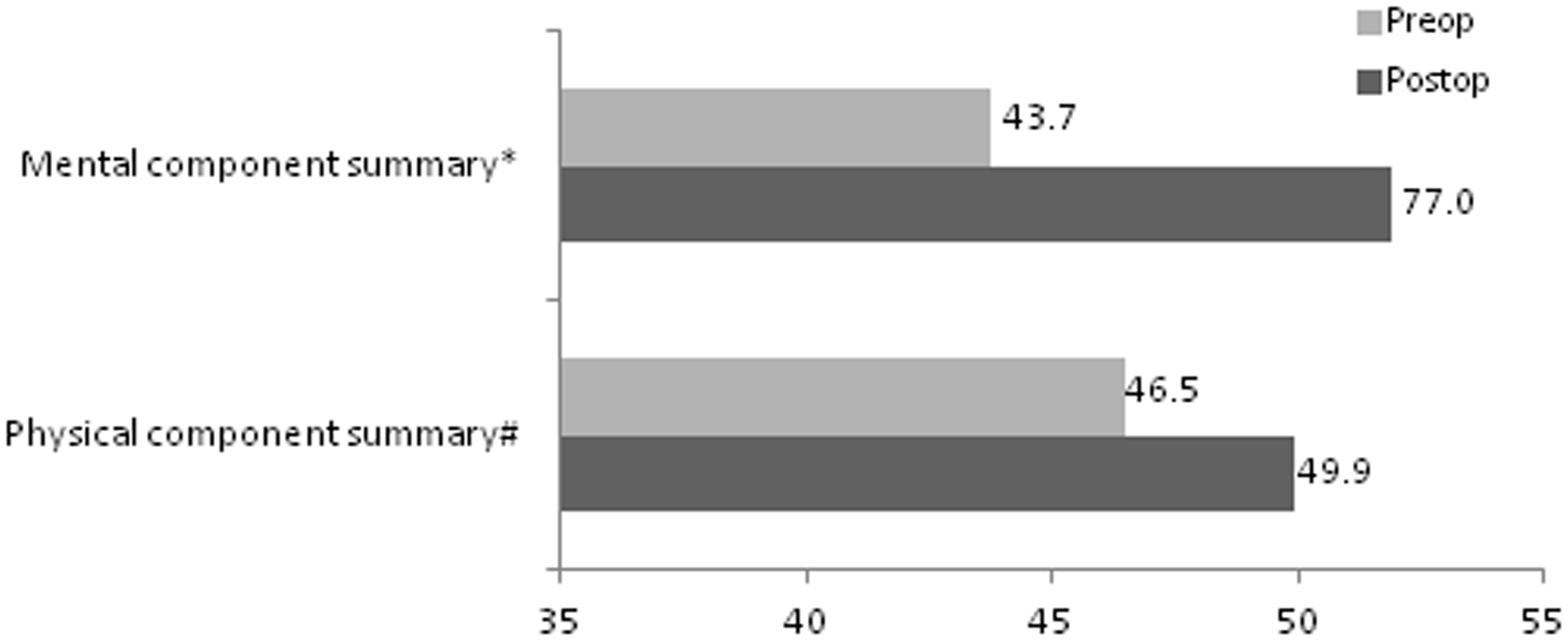
After surgery, the indexed right ventricular end-diastolic volume (193 ± 47.3 vs. 105.6 ± 29.6 mL m−2, p < 0.001) and indexed right ventricular end-systolic volume (108.5 ± 32.9 vs. 61.1 ± 23 mL m−2, p < 0.001) decreased significantly. The response rates for pre- and postoperative quality-of-life assessments were 100%. Patients demonstrated improvements in all 8 domains of the SF-36v2 assessment. The physical (46.5 ± 6.6 vs. 49.9 ± 6.4, p = 0.012) and mental (43.7 ± 7.8 vs. 51.9 ± 7.6, p < 0.001) component summary scores increased after surgery.
Conclusion
Pulmonary valve replacement can improve the quality of life in patients with chronic asymptomatic pulmonary regurgitation.
Keywords
Introduction
With the current trend towards earlier repair of tetralogy of Fallot (TOF) necessitating transannular repair, pulmonary regurgitation (PR) has become more common. Patients with chronic PR can be asymptomatic for a long period of time. However, it has been shown that PR is not benign; chronic PR is known to result in right ventricular (RV) dilatation and dysfunction, ventricular arrhythmia, impaired exercise tolerance, and sudden cardiac death.1–3 Pulmonary valve replacement (PVR) was found to improve patients’ subjective exercise tolerance,4–6 left ventricular function, and RV remodeling,7,8 and it may have beneficial effects on the QRS duration.8,9 Unfortunately, it has been suggested that PVR may not be beneficial in terms of overall survival and the incidence of ventricular tachyarrhythmias in patients with chronic PR after repair of TOF. 10 It is generally advised that PVR should be performed in symptomatic patients with severe chronic PR and also in asymptomatic patients with progressive RV dilatation and dysfunction and left ventricular dysfunction. Many patients with chronic PR are asymptomatic. Traditional indicators such as mortality and objective clinical parameters are no longer sufficient to assess the effect of illness. Health-related quality of life (QOL) measures are therefore necessary. Convincing patients who have no symptoms to undergo PVR may not be easy because they may not feel the urge to undergo this surgery. However, the effects of PVR on patients’ QOL have not been well studied. It is hypothesized that PVR in patients with severe chronic PR would also improve their QOL. We studied the preoperative and postoperative QOL of patients with asymptomatic chronic PR, and investigated whether there was improvement in QOL after PVR.
Patients and methods
Demographic data of asymptomatic patients undergoing pulmonary valve replacement.
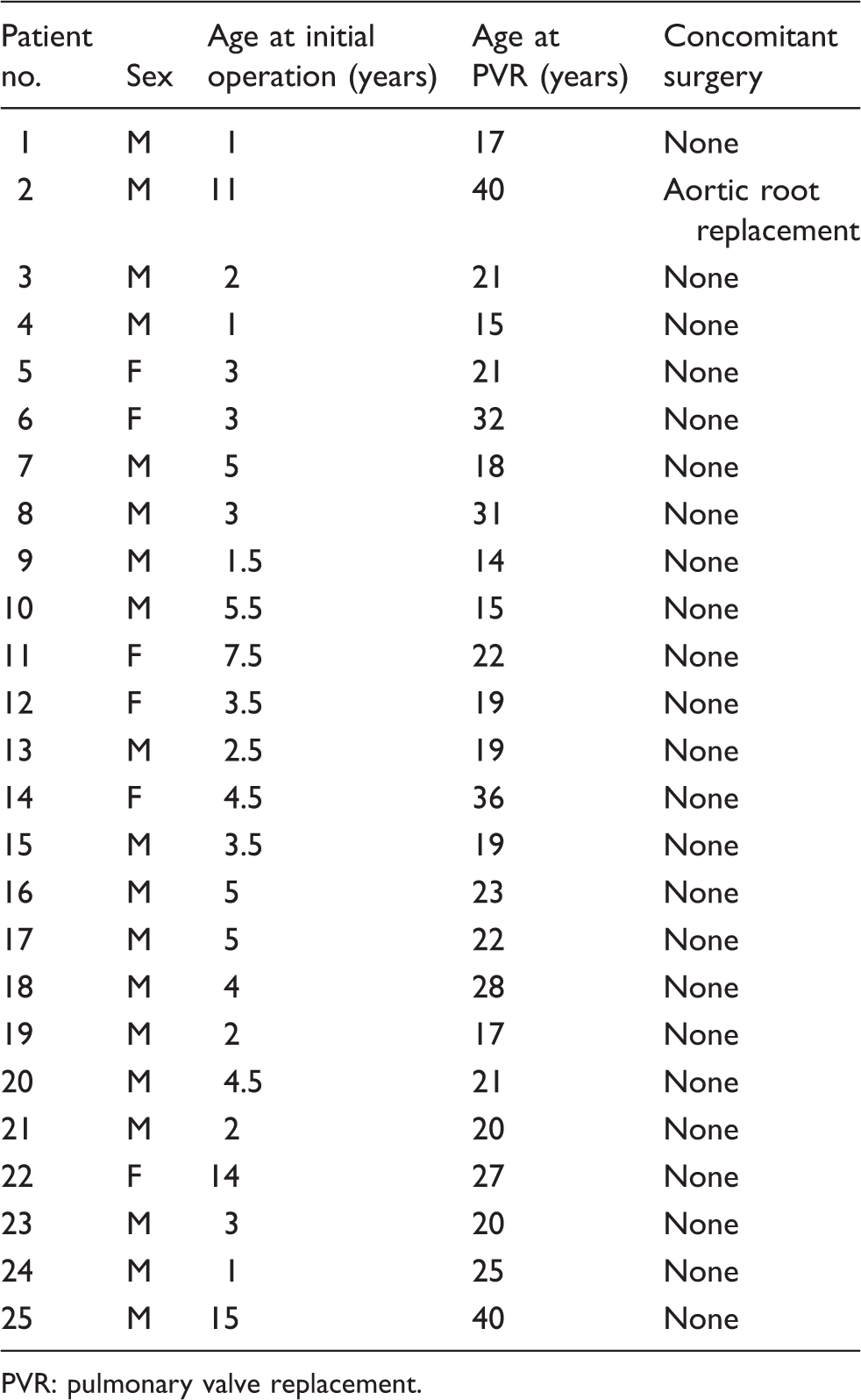
PVR: pulmonary valve replacement.
All patients with chronic severe PR were offered PVR if they were symptomatic, defined as having decreased exercise tolerance or heart failure symptoms (New York Heart Association > class II), or if they were asymptomatic with a high risk of sudden death, 11 including those with RV enlargement or dysfunction (RV diastolic volume index ≥ 170 mL m−2), arrhythmias, and prolonged QRS duration (>180 ms). PVR was performed via a secondary median sternotomy incision and under cardiopulmonary bypass. Cardioplegic arrest was applied when deemed necessary. An incision was made in the RV outflow tract at the previous transannular patch site. The native pulmonary valve was resected and valve replacement was performed with a bioprosthesis or homograft. RV outflow tract reconstruction was carried out as necessary with bovine pericardium or a Gore-Tex patch. After meticulous hemostasis, the wound was closed and the patient was sent to the cardiac surgery intensive care unit for postoperative monitoring and further management.
All recruited patients underwent magnetic resonance imaging before surgery and within 1 year after PVR. Spin-echo T1-weighted sequence axial magnetic resonance imaging of the heart was performed with a FastCINE phase contrast scan or a FIESTA scan of the heart in the axial plane and/or short axis to retrieve the RV end-diastolic volume, RV end-systolic volume, and RV ejection fraction. Flow analysis of the pulmonary artery was also performed.
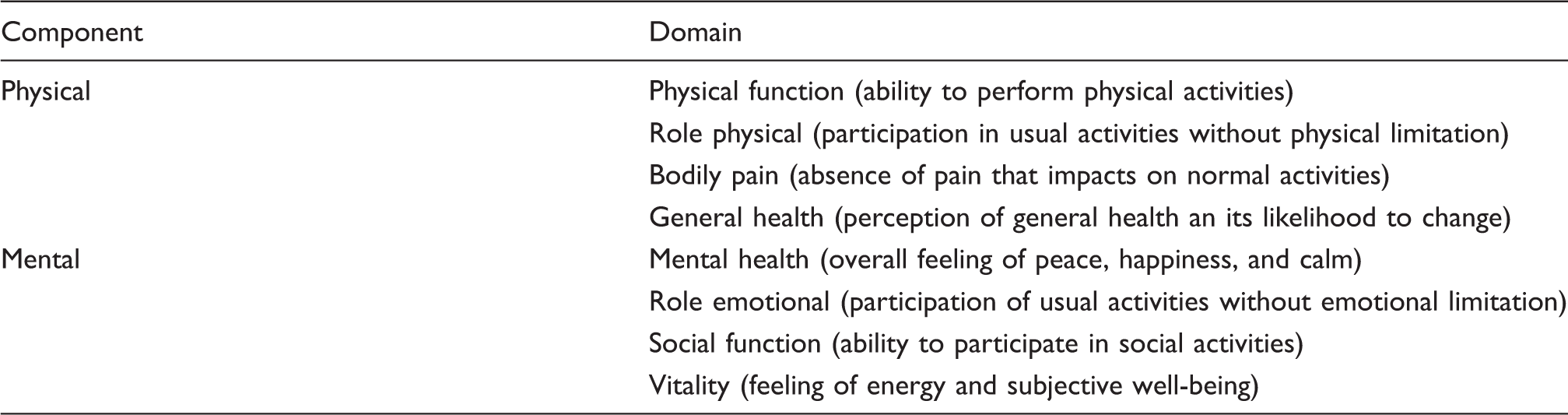
Components of the SF-36v2 questionnaire.
Statistical analysis was performed using SPSS 20.0 software (SPSS, Inc., Chicago, IL, USA). Data are expressed as mean ± standard deviation. The chi-square test or Fisher’s exact test were used for comparison of categorical variables. Student’s t test or Wilcoxon’s signed rank tests were used as appropriate for comparison of parametric and nonparametric variables, respectively. Results were considered significant at p < 0.05.
Results
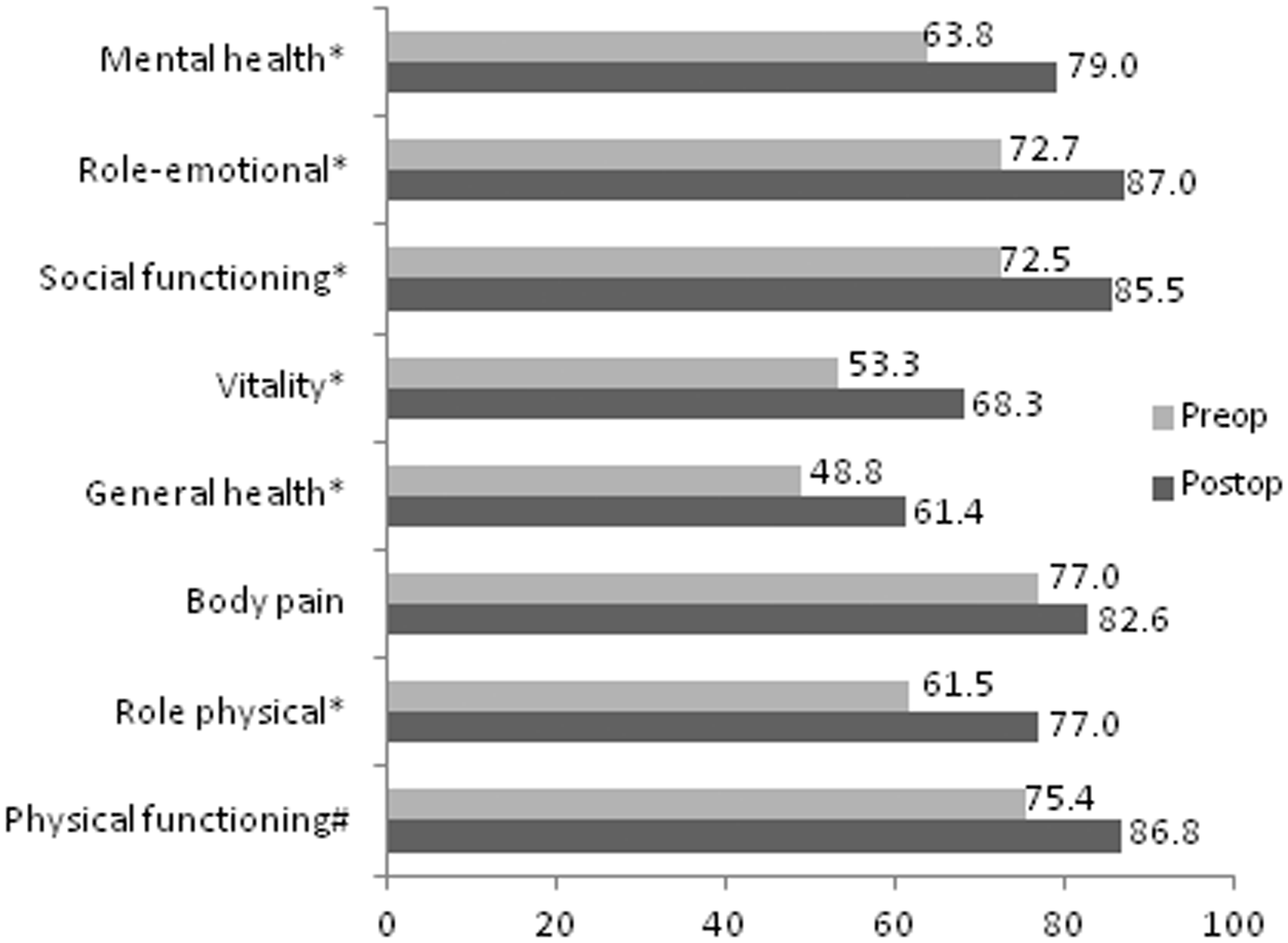
Two patients were in atrial fibrillation before PVR, and the others were in sinus rhythm. These 2 patients were given antiarrhythmic and anticoagulation medications before the operation and were maintained on these medications afterwards. Concomitant arrhythmia surgery was not performed in view of the chronicity of the arrhythmia. The other patients remained in their preoperative cardiac rhythm after the operation, without the need for medication adjustments. There were no other significant morbidities identified in our patient cohort. One patient had a concomitant operation during PVR. No patient underwent concomitant tricuspid valve repair or replacement during PVR. All patients, despite being asymptomatic and in New York Heart Association class I preoperatively, reported subjective improvements in exercise tolerance after the operation. The pre- and postoperative magnetic resonance imaging data are shown in Figure 1. All patients had an overall reduction in RV end-diastolic volume index (from 193.1 ± 47.3 to 105.6 ± 29.6 mL m−2, p < 0.001) and RV end-systolic volume index (108.5 ± 32.9 to 61.1 ± 23 mL m−2, p < 0.01) after PVR. There were no significant changes in RV ejection fraction. Figure 2 shows the pre- and postoperative scores of the SF-36v2 QOL assessment. The response rate for both pre- and postoperative questionnaires were 100% because all questionnaires were distributed and collected by a single interviewer either in-hospital or during out-patient follow-up. The patients demonstrated an overall improvement in all 8 domains of the SF-36v2 assessment and also in the physical and mental component summary scores after PVR (Figure 3). According to the Medical Outcome Studies,
16
scores of 0–24 are poor, 25–60 are fair, 61–83 are good, 84–99 are very good, and a score of 100 is excellent. Our patients, despite asymptomatic chronic PR, scored good preoperatively in all domains except for vitality (energy and fatigue) and general health, where the scores were fair. General improvements were seen in all categories, especially in vitality and general health where the scores improved from fair to good after the operation (53.3 ± 22.5 to 68.3 ± 17.7, p = 0.001; and 48.8 ± 14.4 to 61.4 ± 16.5, p = 0.003). Despite asymptomatic chronic PR, our patients attained relatively low scores before PVR for mental component summary, physical component summary, vitality, and general health (43.7 ± 7.8, 46.5 ± 6.6, 53.3 ± 22.5, and 48.8 ± 14.4, respectively). According to the Medical Outcome Studies, these scores were in the fair category. Significant improvements were observed after PVR in all domains of the QOL assessment, especially in the above-mentioned categories. The scores improved from fair to good in the vitality and general health categories after the operation. Moreover, there were no significant correlations between the percentage change in RV end-diastolic volume index or RV end-systolic volume index and the percentage improvement in the scores in each of the 8 domains in the SF36v2 QOL assessment (p > 0.05).
Mean pre- and postoperative right ventricular magnetic resonance imaging data in patients with asymptomatic chronic pulmonary regurgitation. RVEDVI: right ventricular end-diastolic volume index; RVEF: right ventricular ejection fraction; RVESVI: right ventricular end-systolic volume index. Mean pre- and postoperative SF-36v2 scores in patients undergoing pulmonary valve replacement for asymptomatic chronic pulmonary regurgitation. #p < 0.05. *p < 0.01. Mean pre- and postoperative SF-36v2 mental and physical component summary scores in patients undergoing pulmonary valve replacement for asymptomatic chronic pulmonary regurgitation. #p < 0.05. *p < 0.01.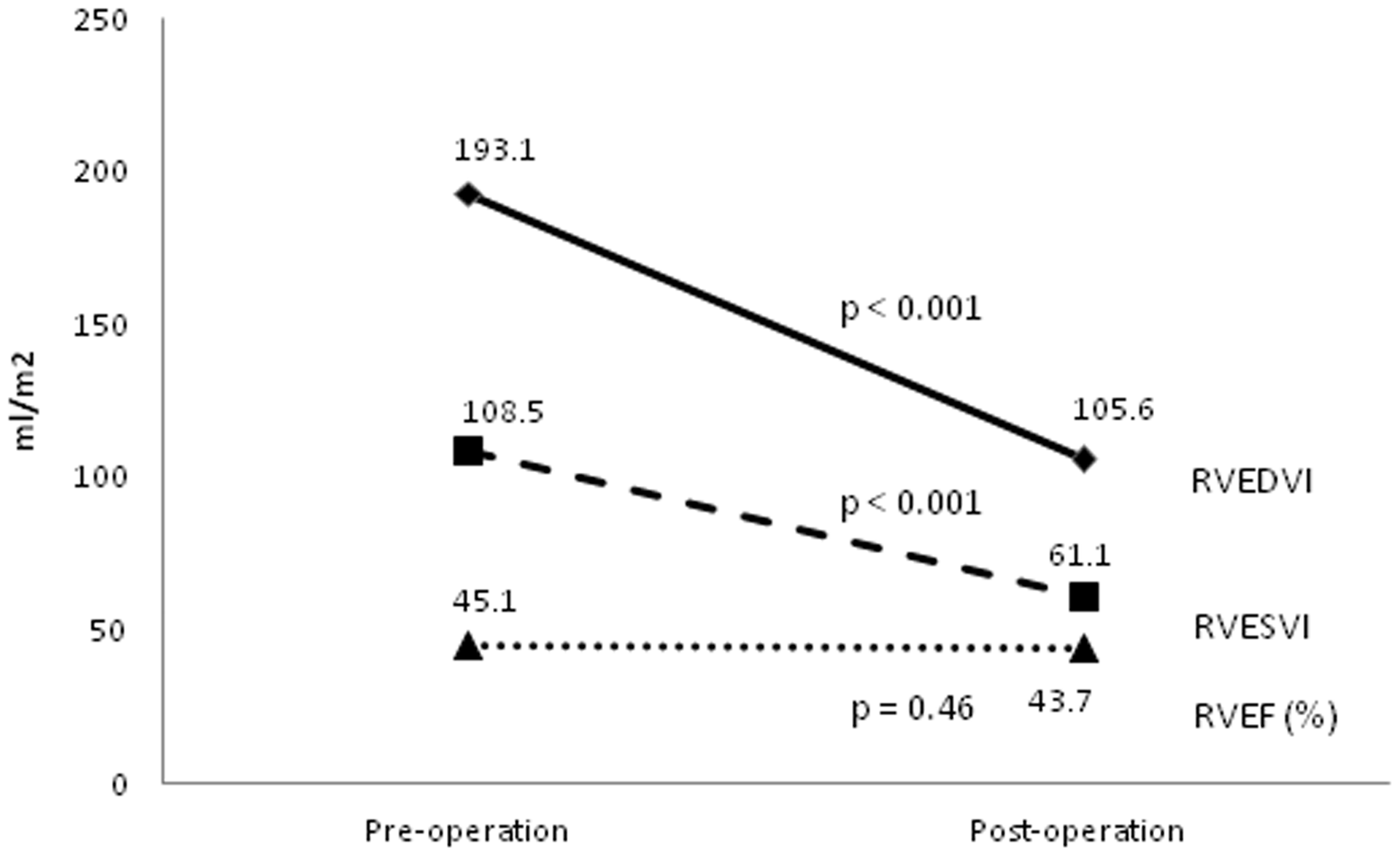
Discussion
This study shows that PVR can improve QOL in asymptomatic patients with chronic PR after previous transannular patch repair of TOF. A general health questionnaire (SF36v2) was chosen as the assessment tool. The SF36 questionnaire is one of the most commonly used health-related QOL assessment tools worldwide. 16 There is evidence supporting its validity and reliability in a variety of patient groups. Its validity in the Hong Kong Chinese population has been established, and the scoring algorithm for the eight SF-36 scales was found to be applicable to the Chinese in Hong Kong.14,15
Chronic PR is a common occurrence after repair of TOF, especially in patients requiring transannular patch repair for a small pulmonary annulus. Long-standing severe PR is associated with RV dysfunction and impaired exercise tolerance.1–3 These patients have a higher chance of sudden death, probably as a result of RV dysfunction and ventricular tachycardia. 1 PVR has been performed to improve symptoms and survival in these patients; however, studies have suggested that PVR does not improve survival in patients with chronic PR. 10 PVR may improve symptoms in patients with symptomatic chronic PR, but a consistent improvement in terms of exercise test parameters is lacking.5,6 Despite the deleterious effects of chronic PR on RV function, many repaired TOF patients remained asymptomatic. Although asymptomatic, these patients do not report a normal QOL. In fact, the patients in our study population reported low scores of 43.7 and 46.5 in the SF36v2 assessment for mental and physical component summaries, respectively, before PVR. This finding is not surprising because chronic PR is known to decrease RV function and exercise capacity.1–3 Daliento and colleagues 17 reported similar findings whereby patients had residual psychological and social problems after TOF repair. Pilla and colleagues 18 also reported that patients had worsening physical domain scores despite preserved psychosocial scores after TOF repair. The results of this study suggest that patients with chronic PR have a relatively low self-image. These patients considered themselves as lacking in energy and having inappropriate social functioning.
Our patients attained relatively low scores in all 8 domains before PVR. Their scores were markedly lower than the normal reference values for Chinese adults aged 18 to 40 years in Hong Kong. 14 Significant improvements were observed in terms of emotional status, social functioning, general health, and other physical aspects after surgery. There were statistically significant improvements in the 2 summary scores and in all 8 domains after surgery for chronic PR. These improvements were not found to correlate with the extent of RV size reduction after PVR. This finding of improvement in QOL after PVR in our Chinese population correlated well with that reported by others; Geva and colleagues 19 showed a significant improvement in physical and mental component scores using the SF-36 assessment tool in patients undergoing PVR for chronic PR at 6 months postoperatively. Studies have shown improvement in right and left ventricular function after PVR. 20 Improved right and left ventricular function may contribute to the improved QOL after surgery in patients with chronic PR. Furthermore, Ho and colleagues 3 showed that patients with severe PR after initial TOF repair had significantly diminished preoperative exercise time and peak oxygen consumption. They observed an age-related difference in terms of a better postoperative exercise time and peak oxygen consumption in patients <25 years old. In our study where the mean age at operation was <25 years, this may explain why our patients had improved exercise tolerance and thus QOL after PVR.
Studies have shown that PVR in patients with chronic symptomatic PR can improve symptoms as well as right and left ventricular function.4,20 However, neither a survival benefit nor an impact on arrhythmias have been found after PVR. 10 Thus the timing of PVR in asymptomatic patients is controversial. Suggested parameters for assessment for PVR in chronic asymptomatic PR include RV end-systolic and end-diastolic volume index, left ventricular diastolic volume index, RV ejection fraction, RV to left ventricular end-diastolic ratio, the presence of any residual hemodynamically significant lesions, and factors predisposing to sudden death such as arrhythmias and prolonged QRS duration. With the assistance of preoperative QOL assessment, it may be tempting to offer PVR for patients with asymptomatic chronic PR with QOL scores lower than the population norm. Moreover, postoperative QOL assessment may potentially become one of the parameters for outcome assessment of the impact of PVR on patients with asymptomatic chronic PR. The potential utilization QOL score in addition to parameters of ventricular function, severity of PR, and exercise capacity in evaluation of the need for PVR in repaired TOF patients should be an important topic in future studies.
The main limitation of this study is the small number of patients, making generalization of the study results difficult. Nevertheless, the improvement in postoperative QOL remains significant. In addition, postoperative QOL assessments were performed only at 6 months after the operation. Whether long-term improvement in QOL can be attained is uncertain. Further studies with longer follow-up is necessary to assess the long-term effects of PVR on QOL in patients with asymptomatic chronic PR. In the present study, we did not perform formal exercise testing before and after PVR. Nonetheless, improvement in exercise capacity has been documented after PVR.5,6 Correlation of the changes in QOL parameters with pre- and postoperative dynamic cardiac assessment and exercise testing will be an important aspect to explore in future studies. We concluded that PVR is associated with improvement in the QOL of patients with chronic asymptomatic PR after previous transannular patch repair of TOF. Further studies are warranted to explore the reasons for the observed improvements in QOL and the utilization of QOL in determining the time of PVR in this growing patient population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.