
Abstract
Entrapment of a guidewire during coronary artery interventions is rare and requires prompt treatment. A 52-year-old man underwent a primary percutaneous transluminal coronary angioplasty to the left anterior descending artery. A fractured guidewire was retained in the distal left anterior descending artery, which caused left ventricular dysfunction and total occlusion of the left anterior descending artery. He underwent endarterectomy with removal of the guidewire and bypass grafting. He had a normal postoperative period. The modalities for management of an entrapped guidewire are discussed.
Introduction
Guidewire fracture and entrapment during coronary artery interventions are rare, but when they do occur they can lead to life-threatening complications such as cardiogenic shock, or they may be asymptomatic. Treatment modalities range from conservative to surgical management, depending on the symptoms, fractured segment, and the coronary artery involved. We describe the case of a patient who underwent percutaneous transluminal coronary angioplasty that resulted in a fractured guidewire entrapped in the left anterior descending artery (LAD), which later caused left ventricular dysfunction. He was treated successfully by surgery.
Case report
A 52-year-old man with a history of angina on exertion (New York Heart Association class II) was referred to our institute. He had undergone primary percutaneous transluminal coronary angioplasty of the LAD in a different institute 2 years earlier. An echocardiogram revealed left ventricular dysfunction with an ejection fraction of 48% and a regional wall motion abnormality of the anteroseptal wall with preserved ventricular thickness. Coronary angiography revealed total occlusion of the LAD with an intracoronary stent in the proximal segment and a fractured guidewire entrapped in the distal segment (Video 1). The circumflex and right coronary arteries also had significant lesions requiring surgical revascularization. Under moderate hypothermic cardiac arrest, LAD endarterectomy was performed, removing the plaque with the entrapped guidewire (Figure 1). A vein patch was used to reconstruct the LAD, and the left internal mammary artery was used to graft the coronary artery. A saphenous venous graft was used to graft the right coronary and the circumflex system. The patient had a normal postoperative recovery and was discharged on the 6th postoperative day. At the 6-month follow-up, he had improved left ventricular contractility with an ejection fraction of 54%.
(a) A long 8-cm segment of the left anterior descending coronary artery endarterectomy, with the entrapped guidewire in the plaque. (b) A closer view of the entrapped guidewire in the specimen.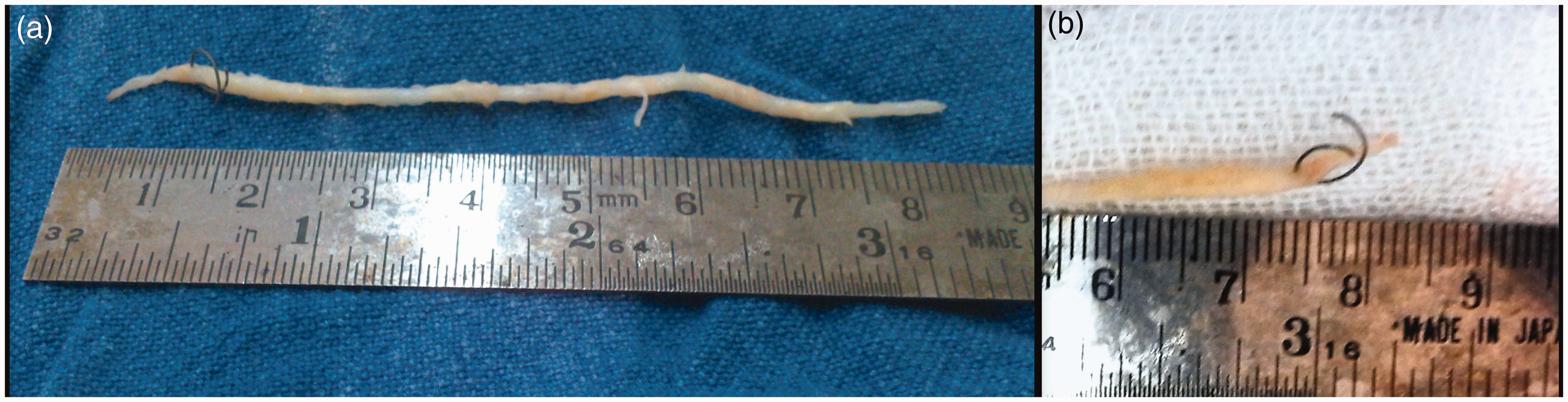
Discussion
Entrapment of catheter remnants in a coronary artery is a rare phenomenon, but when it occurs, it can prove to be fatal. The incidence of this complication is approximately 0.1%–0.2%.1,2 Entrapment or over-rotation of the distal tip of the angioplasty guidewire can lead to wire rupture. Nearly one-fifth of these patients are referred for emergency surgery, which carries a high perioperative risk.3,4 Mortality is nearly 40% in patients presenting in cardiogenic shock. If the patient has sustained preoperative myocardial ischemia, the risk of perioperative infarction is as high 70%, but the risk drops to 2% to 4% in patients without preoperative myocardial ischemia. 3 The guidewire needs to be rotated at times during negotiation across a stenotic lesion. When this rotation exceeds 180°, it leads to lateral stress caused by torquing and unravelling of the platinum coil, which precipitates rupture, especially when the free end is fixed. 5 If ruptured, the retained foreign body provides a nidus for endothelial injury and platelet aggregation, putting the artery at risk of acute thrombosis.
Treatment modalities for such retained fragments of a guidewire include conservative, percutaneous interventions (retrieval, stenting against the wall), or surgical removal, depending on the presentation of the patient and the coronary artery involved. Anecdotal reports concerning a technical difficulty or the anatomy suggest leaving the wire in situ and following the patient with systemic anticoagulation and antiplatelets agents. Retrieval of the entrapped wire can be attempted using two or more wires passed alongside the entrapped wire, torque is then applied and the twisting action results in these wires wrapping around the retained wire and trapping it. Zealous efforts to retrieve an entrapped guidewire may cause further endothelial injury. Therefore, it is often advocated to remove the wire fragment and preform downstream grafting of the coronary artery. Surgical extraction includes a direct coronary arteriotomy or aortotomy to retrieve the wire fragment. A surgical approach always warrants coronary artery bypass grafting. In our patient, the LAD was totally occluded by the wire in the distal segment of the artery. This necessitated endarterectomy of the coronary artery and bypass grafting. If there had been obstructed blood flow by a small fragment in the distal LAD, we might have chosen a conservative course of treatment. Preforming percutaneous retrieval could have caused more injury in this patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.