
Abstract
Sometimes, patients scheduled for cardiac operations other than coronary artery bypass may be unsuitable for preoperative coronary angiography. We routinely use intraoperative high-resolution epicardial ultrasound to select the proper target for the graft and to check graft anastomosis integrity. We describe 3 patients who could not undergo preoperative coronary angiography for different reasons. In all cases, we discovered significant stenosis in the left anterior descending coronary artery, which required bypass grafting. Intraoperative verification by transit-time flow measurements confirmed the significant stenosis detected by imaging.
Introduction
The prevalence of coronary atherosclerosis in patients undergoing valve surgery is 35.6%–50%. 1 We routinely use high-resolution imaging (VeriQ C High-Resolution Epicardial Ultrasound Module; Medi-Stim AS, Oslo, Norway) to check anastomoses, scan the ascending aorta, and detect target sites for grafting. 2 Three patients underwent non-coronary cardiac surgery without preoperative coronary angiography. Their epicardial coronary arteries were scanned to detect stenosis. The first evaluation was a 2-dimensional analysis of the vessels, in cross-section and longitudinally, followed by color-flow mapping. Intraoperative offline post-processing was performed to evaluate the degree of stenosis.
Case reports
Case 1
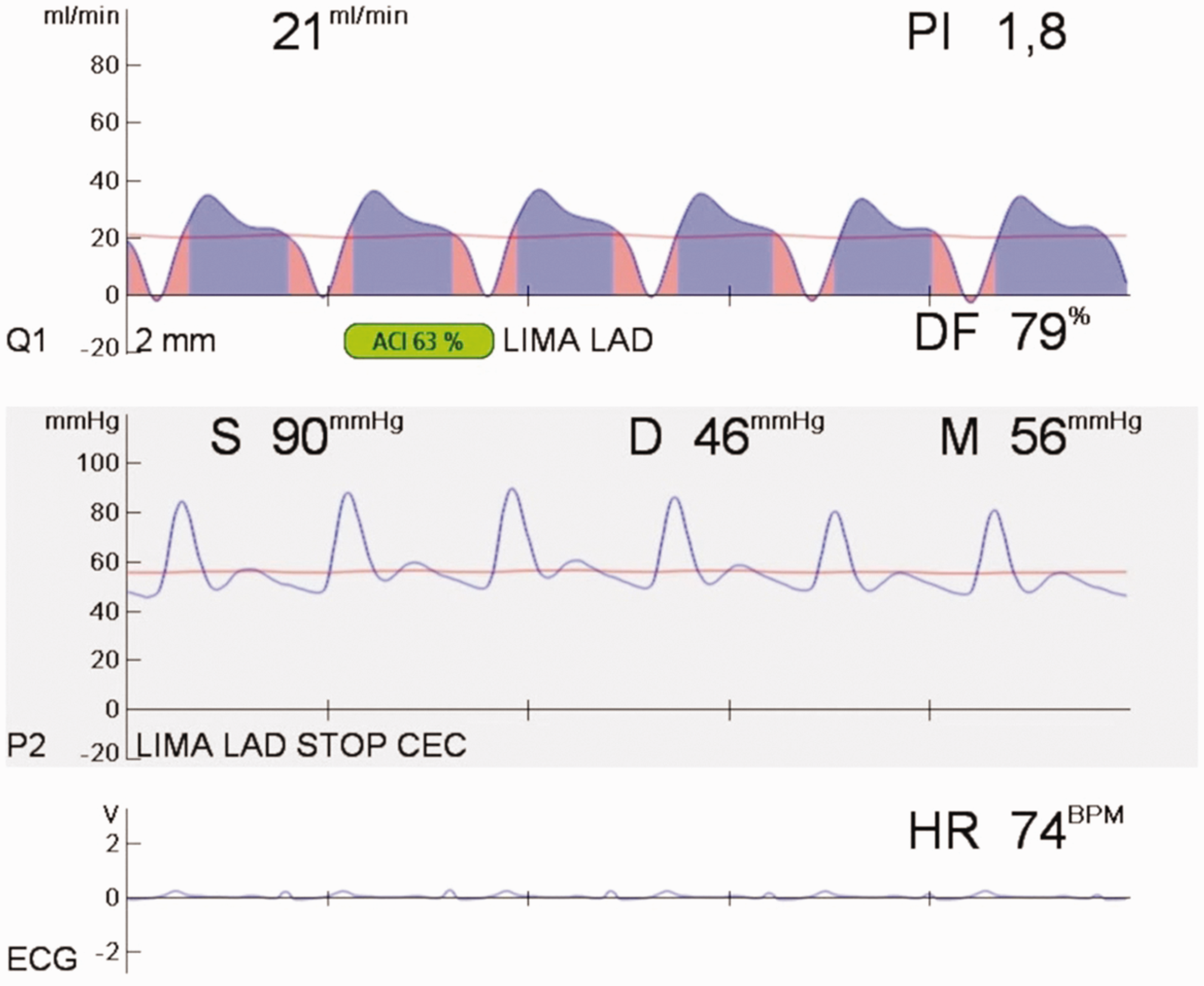
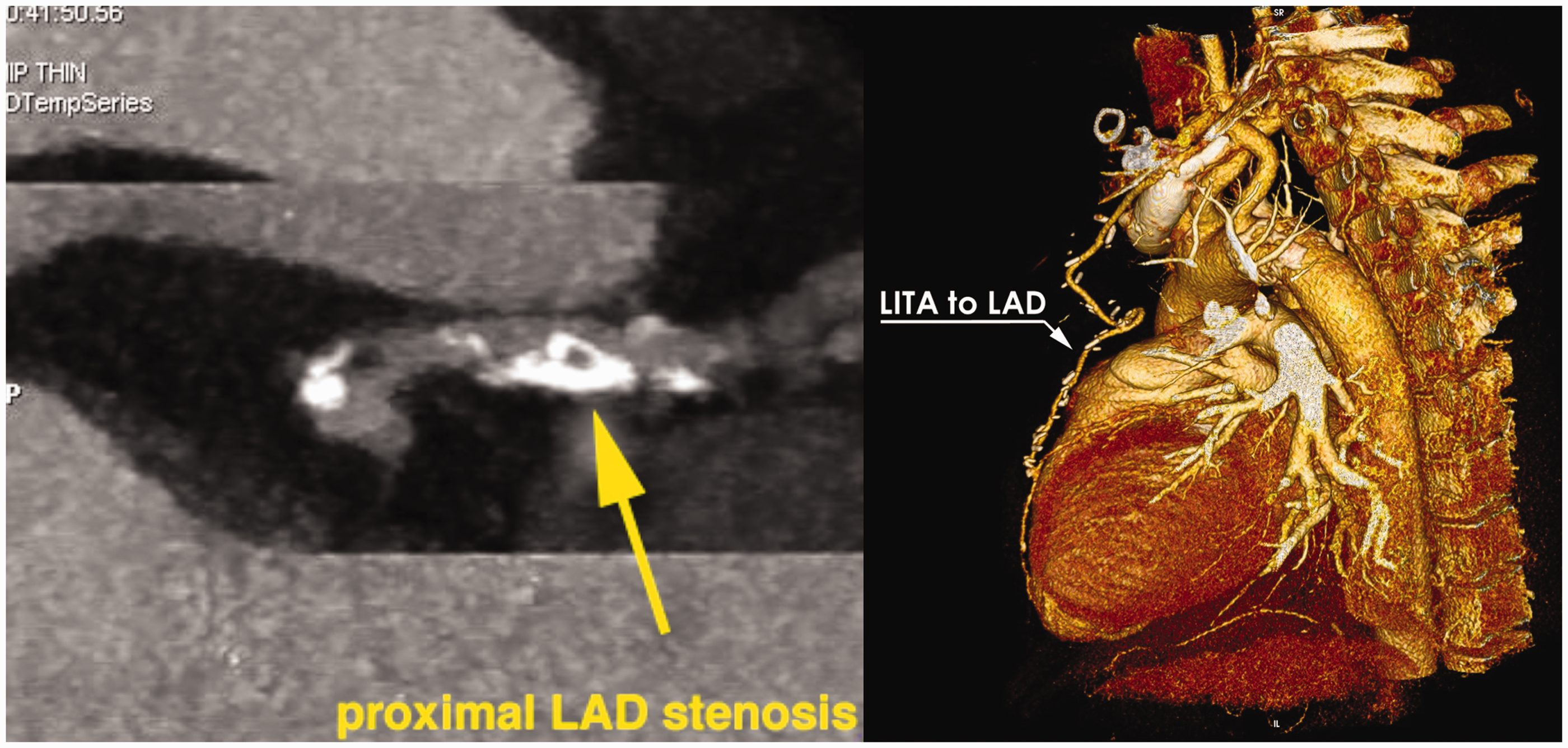
A 67-year-old man with severe aortic regurgitation due to a huge mobile vegetation was considered to have a high risk of embolization, precluding preoperative angiography. During surgery, high-resolution epicardial ultrasound identified significant (70%) proximal left anterior descending artery (LAD) stenosis (Figure 1a). Color-flow mapping showed an area of aliasing corresponding to flow acceleration at the level of the most severe reduction in caliber (Figure 1b). The LAD was bypassed using the left internal thoracic artery. Transit-time flow measurement showed mean graft flow of 21 mL min−1 and a pulsatility index of 1.8 (Figure 2). The postoperative course was uneventful. High-sensitivity peak troponin I was 4.93 ng mL−1. Two weeks after the operation, computed tomography showed a fully patent internal thoracic artery-to-LAD graft (Figure 3); however, it would not have been able to quantify the degree of LAD stenosis due to the heavily calcified vessel wall.
(a) Intraoperative 2-dimensional imaging (long-axis view). (b) Color-flow mapping showing aliasing as a sign of severe stenosis. LAD: left anterior descending artery. Transit-time flow measurement in the left internal thoracic artery (LITA)-to-left anterior descending artery (LAD) graft. Postoperative coronary computed tomography. LAD: left anterior descending artery; LITA: left internal thoracic artery.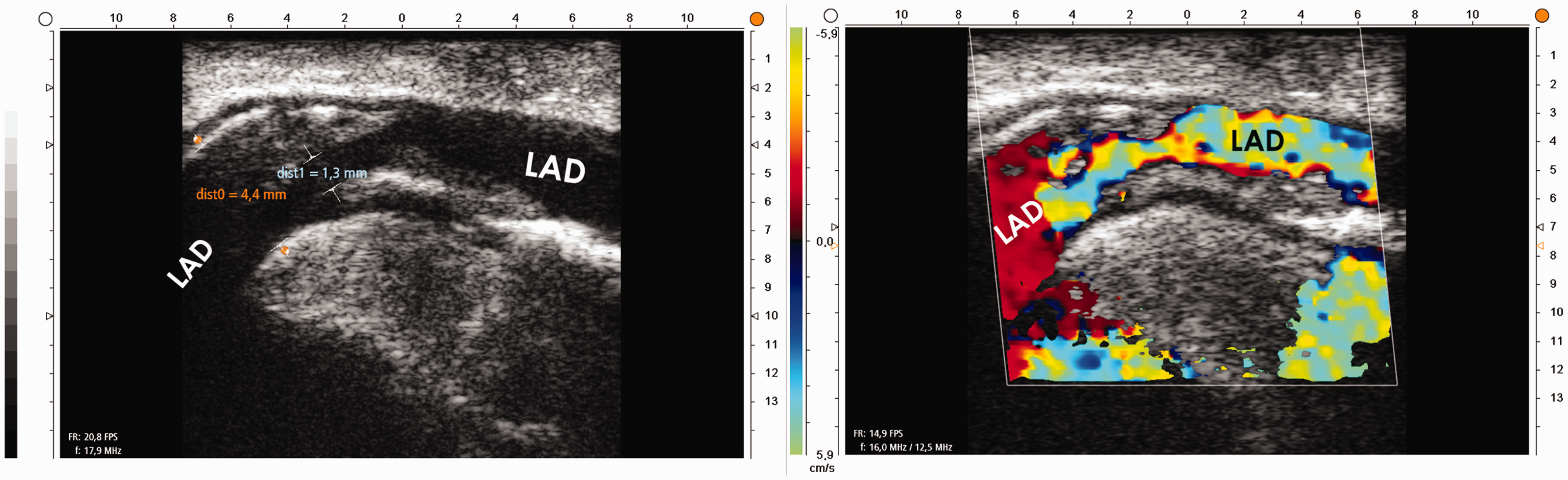
Case 2
An 84-year-old woman was admitted for excision of a 2.7-cm left atrial mass protruding into the left ventricle. She had moderate to severe chronic renal failure, thus preoperative angiography was contraindicated. High-resolution epicardial ultrasound revealed 67% LAD stenosis. After excision of the mass, saphenous vein was grafted to the LAD. Transit-time flow measurement confirmed good function of the graft with mean graft flow 27 mL min−1 and a pulsatility index of 1.1. Postoperative peak troponin I was 1.38 ng mL−1.
Case 3
Angiography was avoided in an 83-year-old woman with severe aortic stenosis and recent severe acute renal failure, because of the high-risk of renal failure recurrence due to contrast dye injection. High-resolution epicardial ultrasound showed severe LAD stenosis. She underwent aortic valve replacement and saphenous vein grafting to the LAD. Transit-time flow measurement confirmed good graft function at the LAD site, with mean graft flow of 55 mL min−1 and a pulsatility index of 1.2. The peak postoperative troponin I level was 0.46 ng mL−1. The postoperative course was uneventful.
Discussion
Preoperative coronary angiography is mandatory in cardiac surgery, however, there are some conditions in which it is not only unsuitable but even potentially dangerous. The European Society of Cardiology suggests avoiding preoperative angiography when the related risks overweigh the benefits, as in the case of a large vegetation. 3 Our first patient had a huge vegetation that was extremely prone to embolize. In the second case, the presence of a large left atrial myxoma required an urgent operation but the patient had moderate to severe chronic renal failure. In the 3rd case, the occurrence of severe acute renal failure some days before surgery was considered to be a relative contraindication to angiography, and the patient’s hemodynamics were unstable but she needed an urgent operation. It is well-known that contrast-induced nephropathy is the third most common cause of hospital-acquired renal insufficiency, with a high rate of morbidity and mortality. 4 Computed tomography-angiography is not performed for preoperative coronary evaluation because of a high rate of false positive results (81%) and a very low positive predictive value (40.4%), especially in cases of severe calcification. 5
High-resolution epicardial ultrasound is a useful tool for assessing coronary stenosis, which shows a good correlation with angiography and pathological findings. 2 High-resolution epicardial ultrasound allowed us to identify coronary stenosis, characterize plaque morphology, assess the degree of lumen reduction, evaluate flow acceleration with color-flow mapping, and check the quality of all anastomoses.6,7 The indications for revascularization following detection of coronary stenosis by imaging are the same as those based on coronary angiography. We calculate the percentage of lumen reduction in long-axis view. In addition, there is the chance to calculate the residual area by scanning the vessel in short-axis view at the level of the stenosis. The small size of the probe is the key factor in left main trunk evaluation, even if stenosis is not easy to detect in all cases; the chance to visualize its bifurcation depends on the length of the main trunk. The circumflex artery is easy to scan in short-axis view along the atrioventricular groove. High-resolution epicardial ultrasound is an easy means to check coronary circulation intraoperatively, without a significant increase in procedural time, when preoperative coronary angiography is inappropriate or dangerous.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.