
Abstract
Good’s syndrome or thymoma-associated immunodeficiency is a rare clinical entity that is often presumed to be common variable immunodeficiency, due to lack of awareness and recognition of this syndrome. This syndrome more often goes unrecognized if a thymoma is not detected. An appropriate immunological work-up that aids timely diagnosis and adequate therapy with antimicrobials and intravenous immunoglobulins are mandatory to prevent the long-term complications and mortality associated with this syndrome. We present the clinical and immunological profile of a young man with Good’s syndrome that was initially presumed to be common variable immunodeficiency.
Keywords
Introduction
Good’s syndrome (GS) was first described by Robert Good in 1954. 1 It is an extremely rare, adult-onset, primary immunodeficiency state associated with thymoma. GS is characterized by increased susceptibility to infections with evidence of hypogammaglobulinemia, absent or reduced B cells with variable defects in cellular immunity such as CD4 T-cell lymphopenia, an abnormal or inverted CD4:CD8+ T-cell ratio, and impaired T cell proliferation in response to mitogen and antigens in the presence of thymoma. 2 Sino-pulmonary infections are the hallmark of GS, and opportunistic fungal and viral infections occur due to B cell deficiency and defects in cell-mediated immunity. 3 Mycobacterial infection is rarely observed in patients with GS, for reasons unknown, and few cases of pulmonary tuberculosis have been reported in world literature. 3 We present a case of GS with spinal tuberculosis.
Case report
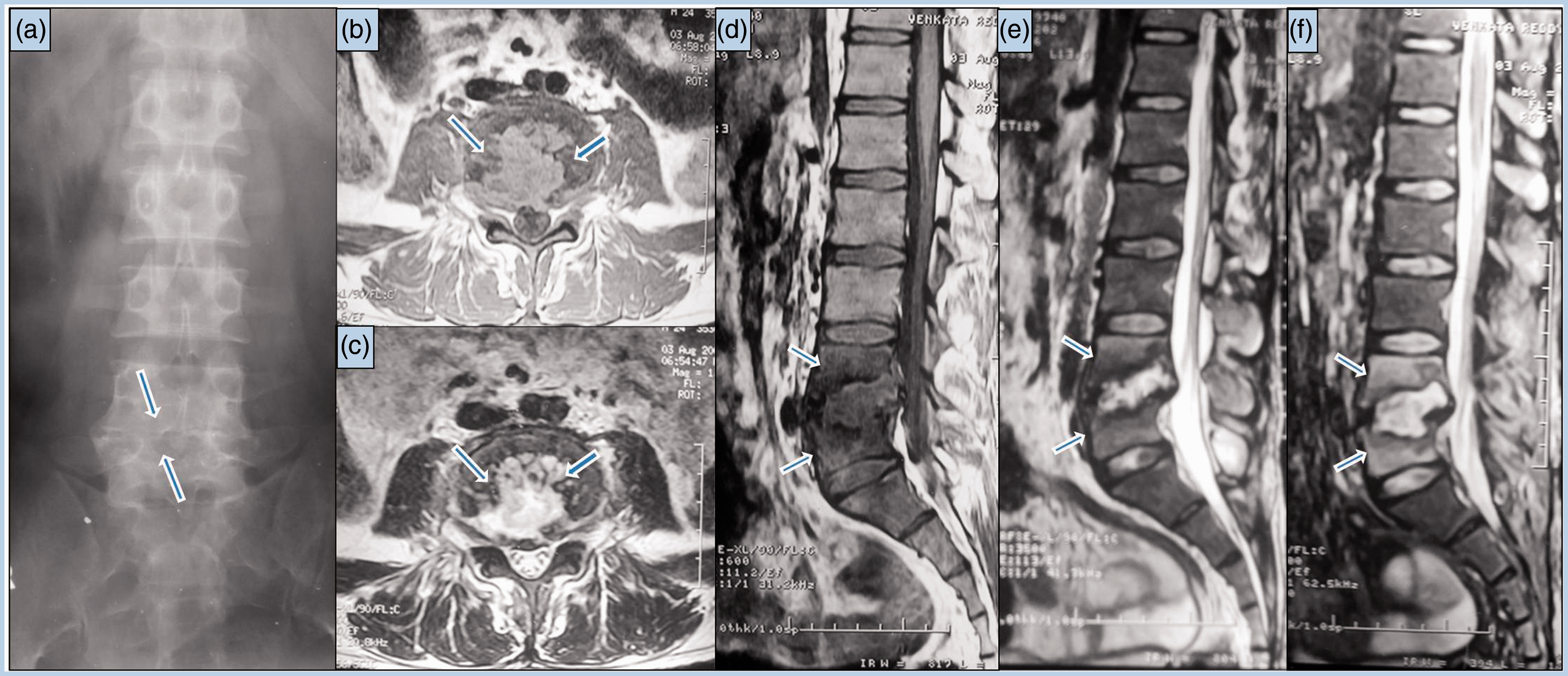
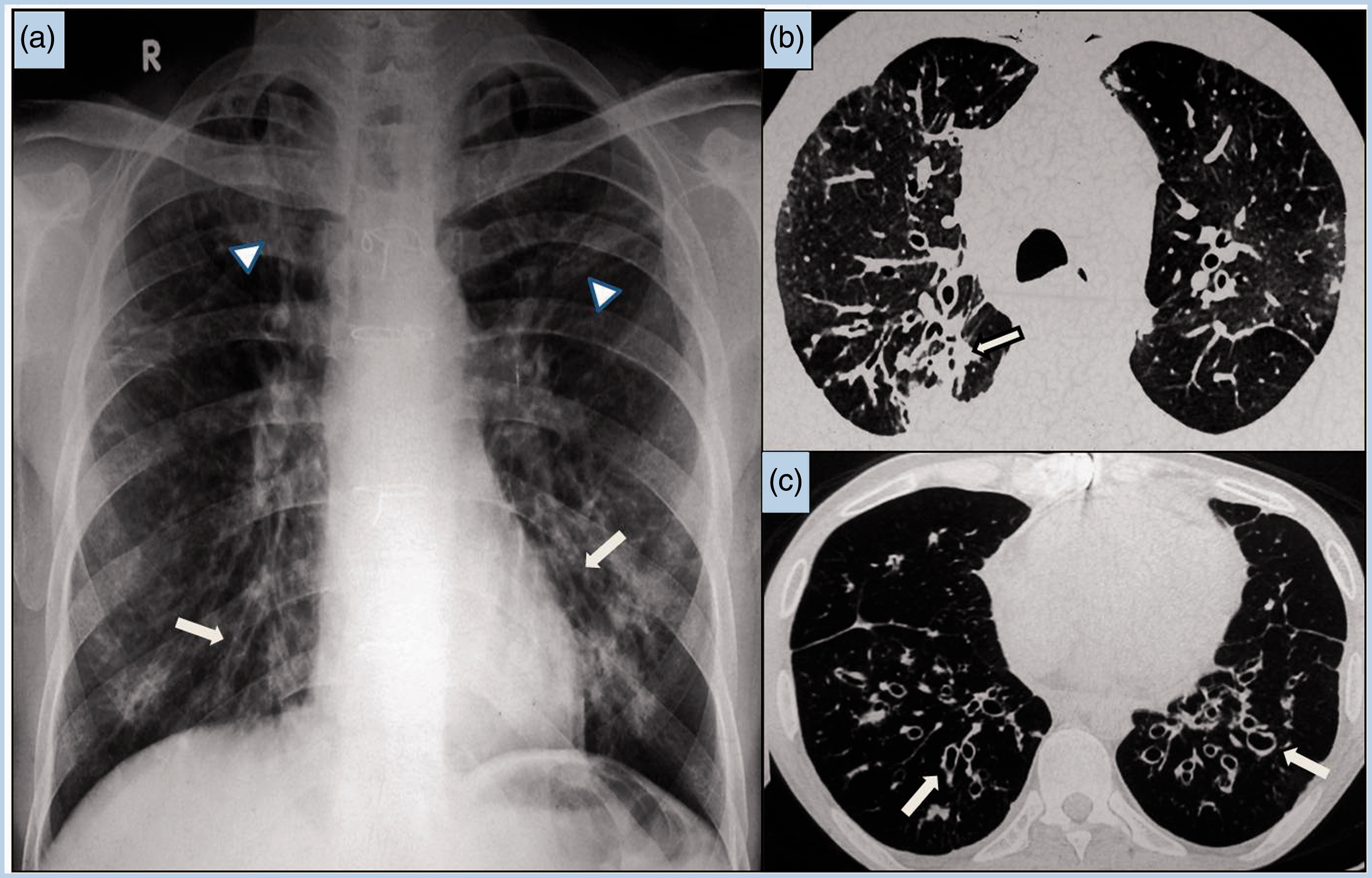
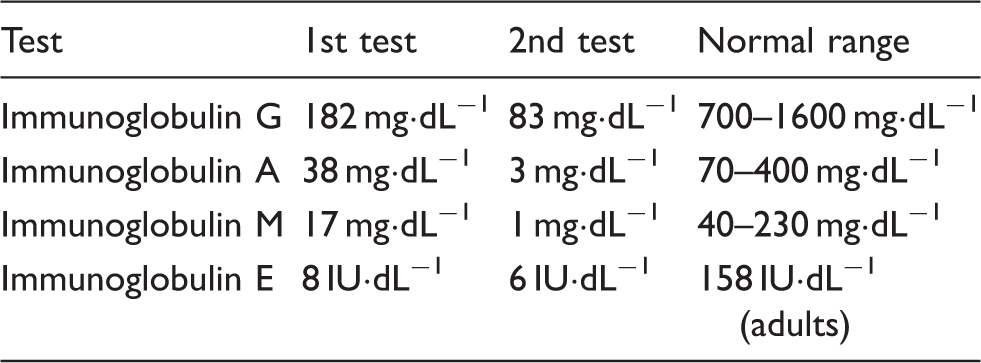
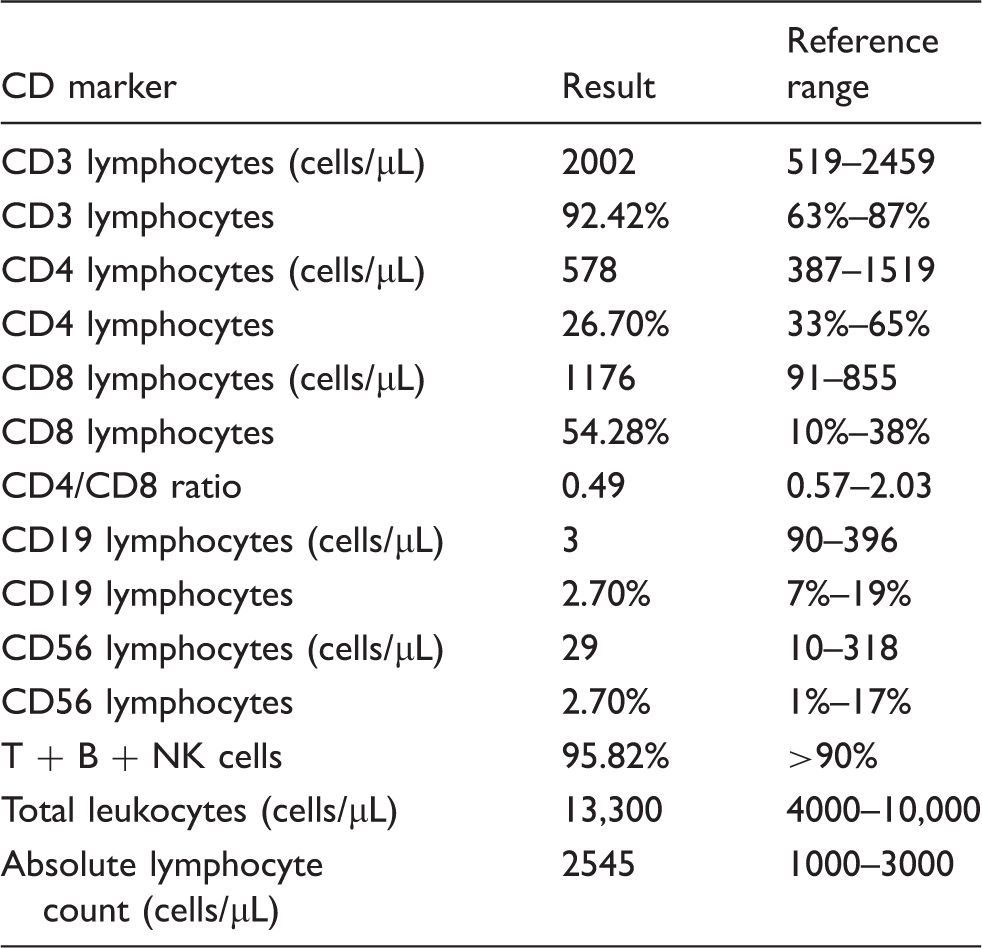
A 35-year-old man presented to our institute with shortness of breath, low-grade fever, and cough with foul smelling expectoration of 15 days’ duration. He had a significant history of similar complaints recurring for the past 15 years. He was not known to be diabetic or hypertensive, and his serology was negative for HIV and hepatitis B surface antigen. Thirteen years earlier, he had been assessed for dry cough of 2 years’ duration and found to have an anterior mediastinal mass on chest radiography (Figure 1), suggestive of thymoma. He underwent a thymectomy and histopathology confirmed a lymphocyte-rich variant of thymoma. Two years later, he presented with a lower respiratory tract infection and loose watery stools (10–15 episodes daily). A duodenal biopsy showed marked villous atrophy. He responded well to antibiotics and was discharged. Later in the same year, he developed low backache and weakness of both lower limbs. Magnetic resonance imaging of the lumbar spine (Figure 2) showed irregular destruction involving contiguous endplates of the L4 and L5 vertebral bodies with reduced disc space and an intradiscal abscess suggestive of infectious spondylodiscitis, considered to be tubercular in etiology. He was treated with antitubercular therapy for 18 months and responded well. Three years later, he again presented with episodes of diarrhea and a respiratory tract infection. Chest radiography and high-resolution computed tomography showed bilateral bronchiectasis with superadded infection (Figure 3). A serum immunoglobulin test revealed panhypogammaglobulinemia (Table 1); he was diagnosed as having common variable immunodeficiency and treated with intravenous immunoglobulin 400 mg kg−1 along with antibiotics. He responded well to the treatment and was discharged. He was lost to follow-up for 6 years and then presented again with chronic diarrhea. A repeat immunoglobulin profile reconfirmed panhypogammaglobulinemia (Table 1), and flow cytometry showed markedly reduced CD19 cells (Table 2), which prompted the diagnosis of GS. The patient was treated with intravenous immunoglobulin along with appropriate antibiotics. He responded well and his diarrhea subsided. He has been on regular treatment and follow-up for 2 years and is doing well.
Chest radiograph demonstrating a fairly large well-defined mediastinal mass (arrows). This proved to be a benign thymoma for which thymectomy was performed. (a) Anteroposterior radiograph of the lumbar spine, demonstrating reduced L4/L5 disc space with irregularity of the vertebral endplates. Magnetic resonance images of the lumbar spine: (b) axial T1-weighted, (c) axial T2-weighted, and (d) sagittal T1-weighted, (e) inversion recovery, and (f) T2-weighted images demonstrating vertebral marrow edema with destruction of the endplates of L4 and L5 vertebral bodies and an intradiscal collection causing thecal compression, suggestive of spondylodiscitis of infectious etiology. (a) Chest radiograph and (b, c) representative axial computed tomography images showing bilateral bronchiectasis (arrows) with thick-walled bronchi and patchy areas of consolidation as well as fibrosis (arrowheads) in the upper lobes, resulting from recurrent chest infections. Immunoglobulin profile of the patient. Quantitative flow cytometry results of lymphocyte subsets.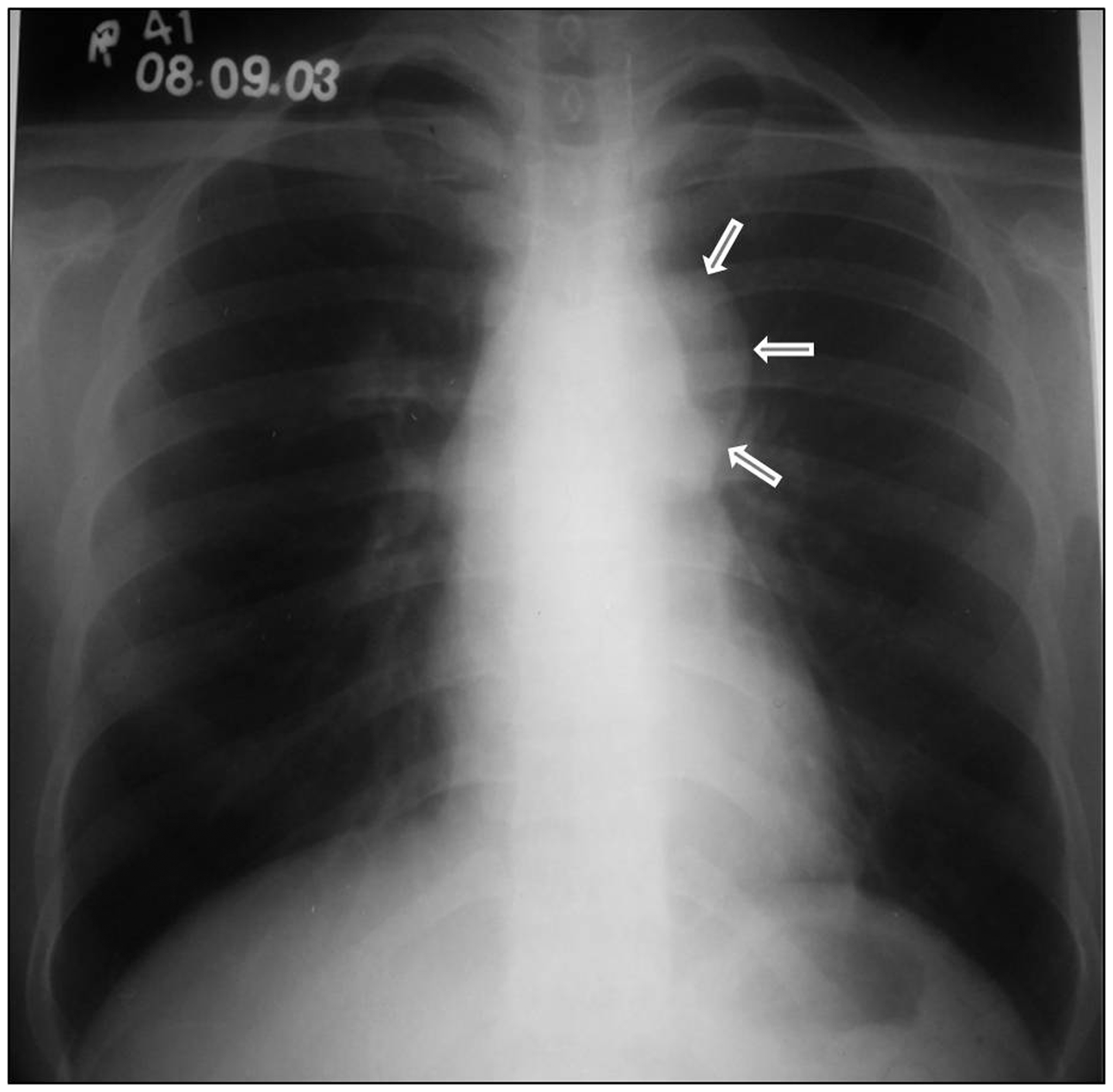
Discussion
The etiopathogenesis of GS remains unknown. Evidence in the literature suggests that the basic defect lies in the bone marrow, and an autoimmune phenomenon and a T-cell defect play key roles in disease manifestation. 2 The immunodeficiency in GS may precede or follow the diagnosis of thymoma. In our patient, thymoma preceded hypogammaglobulinemia and the clinical manifestations. He continued to have symptoms of immunodeficiency even 13 years after thymectomy. He had chronic diarrhea and recurrent respiratory infections progressing to bronchiectasis. Diarrhea is commonly seen in GS in one-third of patients. 3 In our patient, the diarrhea subsided after initiation of intravenous immunoglobulin therapy, thereby supporting the conclusion that hypogammaglobulinemia was the underlying cause. He was also diagnosed with spinal tuberculosis that responded well to antitubercular therapy. Three cases of GS have been reported to date from India; one of these had associated pulmonary tuberculosis.4–6 To the best of our knowledge, only 3 cases of pulmonary tuberculosis in patients with GS have been reported in the world literature.3,4
GS carries a high mortality rate (46%) with infection being the most common cause of death (60%). 3 Noninfectious complications such as autoimmune manifestations and interstitial lung disease are known to occur in GS, which are of major concern because of the associated mortality and morbidity. 5 GS is often misdiagnosed as common variable immunodeficiency during the diagnostic workup, because of associated humoral and cellular immune deficiency. Absent or reduced numbers of peripheral B cells, opportunistic infections due to defects in cell-mediated immunity, old age, and the association with thymoma differentiates GS from common variable immunodeficiency.7,8 GS carries a worse prognosis than its counterparts common variable immunodeficiency and X-linked agammaglobulinemia. 7 Treatment of GS involves thymectomy, intravenous immunoglobulin, and aggressive antimicrobial therapy to combat infections. 7 Immunoglobulin replacement is recommended as the mainstay of therapy for GS because it has been found to decrease infection and hospitalization rates, and improve clinical outcomes.3,7
Footnotes
Acknowledgement
The authors sincerely acknowledge Dr. Anu Kapoor, Department of Radiology and Imaging, Nizams Institute of Medical Sciences, Hyderabad, Telangana, India, for her wholehearted cooperation and timely help rendered during the preparation of this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.