
Abstract
Objectives
Pulmonary dysfunction is a recognized postoperative complication that may be linked to use of cardiopulmonary bypass. The off-pump technique of coronary artery bypass aims to avoid some of the complications that may be related to cardiopulmonary bypass. In this study, we compared the influence of on-pump or off-pump coronary artery bypass on pulmonary gas exchange following routine surgery.
Methods
Fifty patients (mean age 60.4 ± 8.4 years) with no preexisting lung disease and good left ventricular function undergoing primary coronary artery bypass grafting were prospectively randomized to undergo surgery with or without cardiopulmonary bypass. Alveolar/arterial oxygen pressure gradients were calculated prior to induction of anesthesia while the patients were breathing room air, and repeated postoperatively during mechanical ventilation and after extubation while inspiring 3 specific fractions of oxygen.
Results
Baseline preoperative arterial blood gases and alveolar/arterial oxygen pressure gradients were similar in both groups. At both postoperative stages, the partial pressure of arterial oxygen and alveolar/arterial oxygen pressure gradients increased with increasing fraction of inspired oxygen, but there were no statistically significant differences between patients who underwent surgery with or without cardiopulmonary bypass, either during ventilation or after extubation.
Conclusions
Off-pump surgery is not associated with superior pulmonary gas exchange in the early postoperative period following routine coronary artery bypass grafting in patients with good left ventricular function and no preexisting lung disease.
Keywords
Introduction
Pulmonary dysfunction is a recognized complication that can be encountered early after open heart surgery and is associated with increased mortality rates. Impaired pulmonary function may manifest as decreased arterial oxygen partial pressure, atelectasis, pulmonary edema, or adult respiratory distress syndrome. Potential causes of this complication are the effects of sternotomy, internal mammary artery harvesting, pulmonary ischemia with subsequent reperfusion, 1 as well as the inflammatory reaction caused by cardiopulmonary bypass (CPB). 2 The off-pump of technique of coronary artery bypass grafting (CABG) aims to avoid some of the perioperative complications that may be related to the use of CPB. A few previous trials have compared pulmonary dysfunction following on-pump or off-pump CABG and have claimed limited improvement in patients with the off-pump technique.3–5 We compared the effects of on-pump and off-pump CABG on pulmonary gas exchange, using controlled assessments of alveolar/arterial oxygen gradients [P(A-a)O2] following routine surgery.
Patients and methods
Between January and July 2016, 50 consecutive patients (39 men, mean age 60.4 ± 8.4 years) undergoing primary CABG were prospectively assigned by random number table to undergo surgery with (group A) or without (group B) CPB. Patients with acute or chronic lung disease and those who had smoked in the preceding 6 months were excluded, as were those with depressed left ventricular function (ejection fraction <40%). Informed consent was obtained from all patients, and the study was approved by the hospital ethics committee.
In all patients, a standardized anesthesia technique was used, 6 and surgery was carried out through a median sternotomy. The skeletonized left internal mammary artery was harvested without entering the left pleural cavity, and the long saphenous vein was harvested endoscopically. All operations were performed by one surgeon (MBI). In group A, CABG was carried out using CPB with aortic crossclamping and cardioplegic arrest, according to our established routine. 6 In group B, CABG was carried out using commercially available coronary stabilizers and intracoronary shunts, as described previously. 2
Baseline arterial blood samples (2–3 mL) were taken for blood gas analyses (Stat Profile analyzer; Nova Biomedical, Waltham, MA, USA) while the subjects were breathing room air spontaneously prior to induction of anesthesia. Formal studies of pulmonary gas exchange were carried out postoperatively in the intensive care unit once the patients had stable hemodynamics with no inotropic support, as described previously. 6 Briefly, arterial blood gas analyses were performed during artificial ventilation with 3 pre-set oxygen fractions (FiO2; 30%, 40%, and 60%; stage 1), and were repeated one hour after extubation while the patients were spontaneously breathing the same 3 FiO2 (stage 2). The partial pressure of alveolar oxygen (PAO2) was calculated using the alveolar gas equation, 6 and the alveolar/arterial oxygen pressure gradient [P(A-a)O2] was calculated as: P(A-a)O2 = PAO2–PaO2, where PaO2 is the partial pressure of arterial oxygen.
Data analyses were performed using PASW Statistics 18 software (SPSS Inc., Chicago, IL, USA), and the results are presented as mean ± standard deviation. Student’s t test was used to analyze differences in PaO2, PaCO2, and P(A-a)O2 between the two groups. Pearson’s correlation was used to explore relationships between P(A-a)O2 and 6 quantitative variables: age, no. of grafts, ejection fraction, intubation time, blood transfusion, and baseline P(A-a)O2. A p value <0.05 was selected to indicate significance.
Results
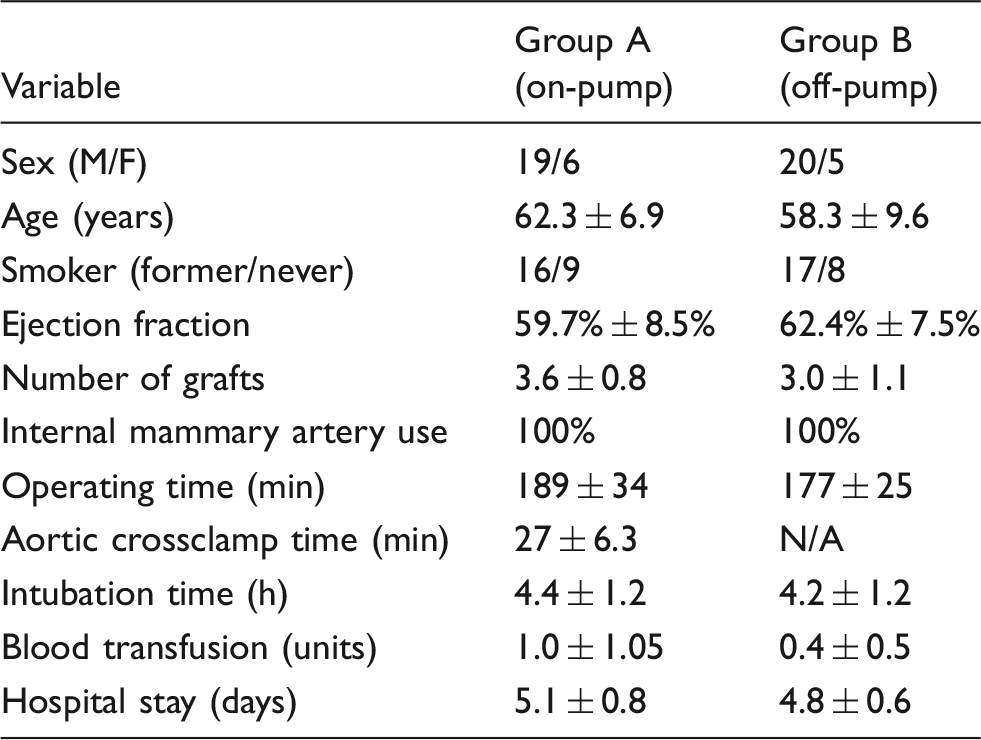
Demographic data of 50 patients undergoing coronary artery bypass grafting with or without cardiopulmonary bypass.
Arterial blood gas analyses and alveolar/arterial oxygen pressure gradients.
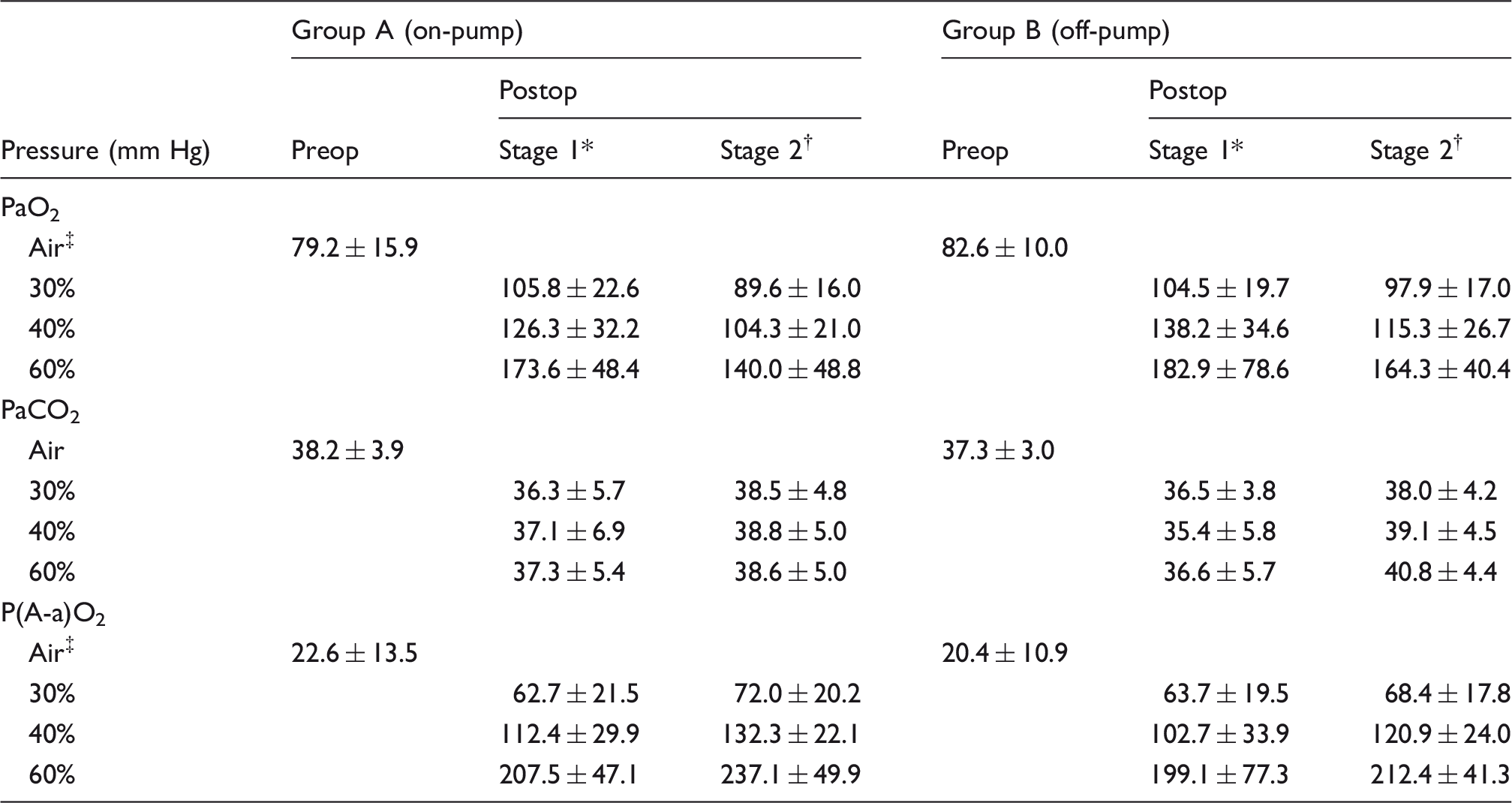
Stage 1 is 2–4 h postoperatively with the patient on artificial ventilation. †Stage 2 is 1 h after extubation with the patient breathing spontaneously. ‡Air is the preoperative sampling period with the patient breathing room air. P(A-a)O2: alveolar/arterial oxygen pressure gradient; PaCO2: partial pressure of arterial carbon dioxide; PaO2: partial pressure of arterial oxygen; Preop: preoperative; Postop: postoperative.
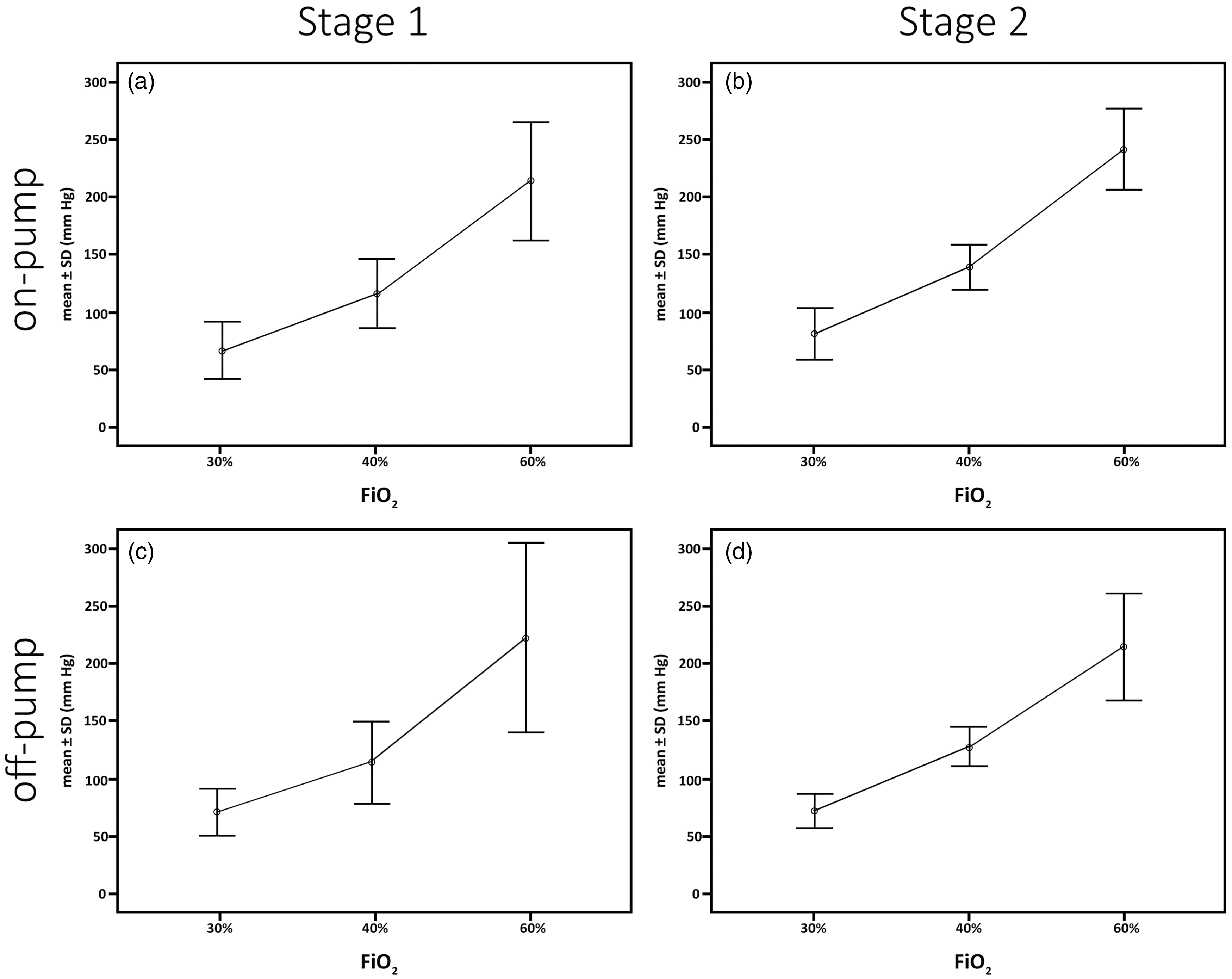
Postoperative alveolar/arterial oxygen pressure gradients in (a, b) the on-pump and (c, d) off-pump groups; a and c show results in stage 1, and b and d show results in stage 2. FiO2: fraction of inspired oxygen.
Discussion
CPB has long been perceived as the main source of pulmonary dysfunction after open heart surgery. 1 CPB is responsible for triggering an inflammatory reaction and for the generation of proinflammatory cytokines that can lead to attraction, sequestration, and activation of neutrophils within the pulmonary circulation. 2 Activation of the complement system may also lead to increased pulmonary vascular permeability with transit of fluid and macromolecules into the pulmonary interstitium, and ultimately the alveoli. 1 The effect of off-pump CABG on pulmonary function is not yet clear. There have been reports of improved static and dynamic lung compliance, reduced rates of respiratory complications, and shorter intubation times in off-pump CABG patients;3,7–12 better preservation of pulmonary function has been proposed as an explanation.8,10,13,14 In contrast, other studies found no significant differences in pulmonary gas exchange, time to extubation, or postoperative pulmonary function between on-pump and off-pump CABG patients.3,14–18 In this study, we used a noninvasive yet sensitive measure of pulmonary gas exchange to conduct a controlled comparison between the effects of on-pump and off-pump CABG. 6 In line with 2 earlier studies that explored changes in alveolar/arterial oxygen pressure gradients,3,19 our results confirmed that pulmonary gas exchange and arterial blood gases decreased comparably postoperatively in both on-pump and off-pump CABG groups.
The reliability of our results was further enhanced through calculating alveolar/arterial oxygen pressure gradients while utilizing 3 different FiO2 in 2 specific postoperative states. With this controlled protocol, it was possible to compare pulmonary gas exchange at 6 postoperative points. 6 Remarkably, alveolar/arterial oxygen pressure gradients in the 3 pre-set FiO2 were virtually superimposable both before and after the patients had been extubated (Figure 1), indicating confidently that there was no advantage of off-pump over on-pump CABG in terms of postoperative pulmonary gas exchange. The direct inference from this similarity between the 2 groups would be that CPB per se played a very limited or no part in the pathogenesis of postoperative pulmonary dysfunction, and that factors other than CPB were responsible for this process. Eliminating CPB did not materially influence the degree of pulmonary dysfunction, and this helps to explain the results of previous studies where variations in CPB perfusion temperature or use of biocompatible CPB circuits and leukocyte filters did not lead to a reduction in lung injury despite attenuation of the inflammatory response.6,20 A variety of factors other than CPB may account for the development of lung injury. General anesthesia by itself can alter surfactant function, and interstitial edema can contribute significantly to mechanical and gas exchange abnormalities;1,2 extravascular lung water accumulation and miliary atelectasis have been demonstrated in patients undergoing major non-cardiac operations. Other potential factors common both to on-pump and off-pump CABG include inappropriate positive-pressure ventilation, administration of colloidal solutions, use of protamine, and reduced cellular viability and impaired functional responses of the pulmonary arteries.2,21
The main limitation of this study was that the subjects were highly-selected to be free from preexisting acute or chronic lung illnesses, to have not smoked in the preceding 6 months, and to have normal left ventricular function. Furthermore, assessments of pulmonary gas exchange were carried out for a relatively short period, and within a few hours of the patient’s arrival in the intensive care unit. A more exacting study of the effects of on-pump and off-pump CABG on pulmonary gas exchange would necessitate inclusion of patients in more compromised pulmonary states, and assessments of pulmonary gas exchange over longer periods postoperatively. However, we concluded that despite the fact that CPB has long been held responsible for pulmonary dysfunction after open heart surgery, this detailed noninvasive study failed to demonstrate any benefit of off-pump over on-pump CABG in terms of early postoperative pulmonary gas exchange in patients with good left ventricular function and no preexisting lung disease.
Footnotes
Acknowledgment
The authors would like to thank Gazwan Jabasini, PhD, for his assistance in data analyses. The authors would also like to thank Drs. Jamil Abbas and Majd Ismail for their technical help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.