
Abstract
Despite the high frequency of gastrointestinal complications and opportunistic infections in HIV-1 infected patients, tracheoesophageal (TEF) and bronchoesophageal (BEF) fístulas are rare. Our objective is to comunicate an additional and unusual case of TEF in an HIV-1-infected patient whose immunologic status was good with complete suppression of viral replication, so although uncommon, TEF/BEF of an infectious origen should be considered in AIDS. Endoscopic treatment with tracheal/esophageal stents is not without morbidity and mortality. As long as the patient can undergo reconstructive surgery, this should be the technique of choice.
Introduction
Acquired tracheoesophageal fistulas (TEF) and bronchoesophageal fistulas (BEF) are uncommon and mainly caused by malignant neoplasms, complications related to mechanical ventilation, and trauma in immunocompetent adults. 1 In immunocompromised individuals infected with human immunodeficiency virus type 1 (HIV-1), infection can also play a role in the development of these fistulas. In this context, fistulas have been reported since the early years of the epidemic, 2 although they are very rare today. We describe a case of esophagitis caused by cytomegalovirus (CMV) in an HIV-1-infected patient, whose condition was complicated by a fistula in the tracheal membranous wall.
Case report
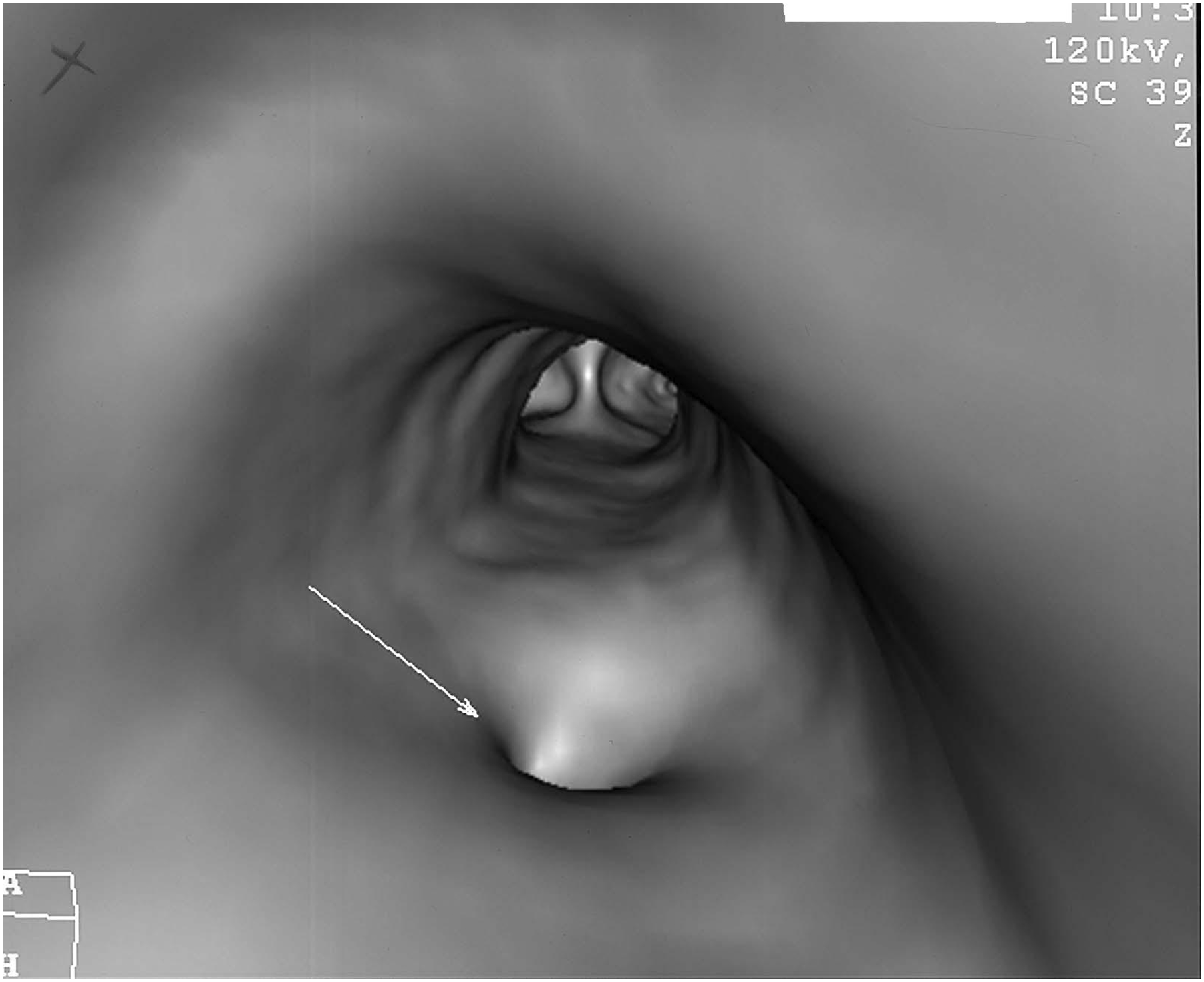
A 42-year-old man was admitted with dysphagia for liquids and solids, worsening cough, and increased sputum production. He was addicted to intravenous drugs (currently on replacement therapy with buprenorphine) with occasional inhaled cocaine. He had chronic liver disease caused by hepatitis C virus and HIV-1 infection (stage C2, after diagnosis of pulmonary tuberculosis 12 years earlier). He had been taking a fixed combination of zidovudine, lamivudine, and abacavir for 11 years and his adherence was good. Laboratory tests one month before admission revealed a CD4+ T-cell count of 695/mm3 (38.6%) and RNA HIV-1 < 1.7 log10 copies/mL. Oral panendoscopy revealed an ulcer on the upper third of the esophagus, measuring 2–3 mm with thickened but regular edges. Histology of biopsy samples from the edge of the ulcer showed extensive necrosis, acute inflammatory infiltration, vascular alterations, and multinucleated CMV inclusion bodies. The diagnosis was esophageal ulcer caused by CMV, and treatment was started with intravenous ganciclovir 5 mg/kg 12-hourly for 2 weeks, later replaced by oral valganciclovir 900 mg 12-hourly for 3 weeks. The patient’s dysphagia gradually improved, but 5 weeks after admission, coinciding with the end of his antiviral therapy, he began coughing on ingesting food. Oral endoscopy revealed a fistulous orifice towards the membranous wall of the trachea. Fiberoptic bronchoscopy showed a fistula (approximately 4 mm) in the posterior tracheal wall 5-cm above the carina. High-resolution computed tomography confirmed a fistula in the upper third of the esophagus and the posterior wall of the trachea (Figure 1, Figure 2). With a preoperative diagnosis of TEF secondary to CMV esophagitis, surgery was the preferred option. After a low collar incision and resection of 2 tracheal rings, a 4.7-mm fistula was identified. The esophagus was sutured directly on 2 planes and the trachea was repaired by end-to-end anastomosis. The sternohyoid muscle was then placed between the trachea and the esophagus. The postoperative period was unremarkable. Twenty-seven months later, the patient is asymptomatic and adhering to his antiretroviral regimen. The latest tests showed a CD4+ T-cell count of 812 cells/mm3 (37.9%) and RNA HIV-1 < 1.7 log10 copies/mL.
High-resolution computed tomography of the thorax (sagittal plane), showing the fistula between the esophagus and the posterior wall of the trachea. Computed tomography of the thorax. Three-dimensional reconstruction showing the origin of the fistula orifice in the posterior wall of the trachea, 5 cm from the carina.
Discussion
Despite the high frequency of gastrointestinal complications and opportunistic infections in HIV-1-infected patients, TEF and BEF are rare. The causative agents have been reported to be Mycobacterium. tuberculosis, Mycobacterium avium-intracellulare, Candida species, Nocardia species, CMV, and herpes simplex virus. A fistula between the gastrointestinal tract and the airway is a serious condition. Treatment is mandatory to avoid continuous aspiration, chronic sepsis, and pulmonary failure, mainly in immunocompromised patients. Some studies favored tracheal or esophageal stents as a corrective measure, although neither is free from complications, and they are palliative measures. The main complications are mucus plugging, granulation tissue formation, stent migration, and iatrogenic perforation;3–5 therefore, stenting should be restricted to cases of unresectable tumors or terminally ill patients.
Surgery always involves repair of the fistula by primary esophageal closure with possible resection of a tracheal fragment, according to the degree of involvement. In some cases, simple closure of the tracheal membranous wall is sufficient, but it is sometimes necessary to resect a segment of the trachea with end-to-end anastomosis. In large airway defects, closure using an AlloDerm parch has been described. 6,7 It is always necessary to place a muscle flap between the esophagus and trachea to protect the sutures and ensure that the area is completely sealed. When there is esophageal wall damage or a severe inflammatory process, esophagectomy should be considered. 8 Complications must be avoided by elevating the head of the bed, continuous aspiration of secretions, and improving the patient’s nutritional status. In this respect, a draining gastrostomy and a feeding jejunostomy are very useful. These measures usually obviate the need for esophageal diversion. In agreement with others, 1 we do not believe that nasogastric tubes are suitable for feeding, because of the continuous contact between the tube and the fistula. A review of the literature revealed no reported cases of TEF caused exclusively by CMV in an HIV-1-infected patient with a CD4+ count and RNA HIV-1 level similar to those we describe.
Footnotes
Acknowledgments
The authors are grateful to Dr. Henning A Gaissert for his help and constructive comments which improved the paper. We also wish to thank Thomas O’Boyle for his help with the preparation of the article and English syntax.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.