
Abstract
Background
Surgical pulmonary thromboendarterectomy has been established as the treatment of choice for chronic thromboembolic pulmonary hypertension. We conducted a survey among Asia-Pacific cardiothoracic surgeons to examine their current practice demographics and reflect their views on the future prospects for pulmonary thromboendarterectomy surgery.
Methods
All cardiothoracic surgeons who were registered on the CTSNet.org website and based in the Asia-Pacific region were invited to participate in an online survey. The electronic questionnaire was completed by 172 (6.3%) surgeons. Responses were recorded anonymously and tabularized as absolute figures and fractions.
Results
Pulmonary thromboendarterectomy surgery has been performed by few Asia-Pacific surgeons and in small numbers of patients, but survival rates and functional outcomes were satisfactory in most experiences. Failures were thought to have resulted primarily from the difficulty in selecting suitable candidates for surgery. The need for greater clinical experience was clear, yet this might be hampered by the limited recognition of pulmonary thromboendarterectomy surgery as a potential cure for chronic thromboembolic pulmonary hypertension. Most surgeons considered that this procedure should be restricted to designated expert centers, and acknowledged the need to organize dedicated regional meetings where clinical practice guidelines can be established and updated as appropriate for regional healthcare facilities.
Conclusions
Although much effort is needed before pulmonary thromboendarterectomy surgery becomes widely adopted in the Asia-Pacific region, many surgeons and centers are already seeking its implementation. Designating expert centers, bringing together a regional working group on pulmonary thromboendarterectomy, and establishing clinical practice guidelines as appropriate for regional healthcare facilities were recommended.
Keywords
Introduction
Surgical pulmonary thromboendarterectomy (PEA) is presently considered the first choice of treatment for chronic thromboembolic pulmonary hypertension (CTEPH) due to its established efficacy in improving patient prognosis and the limited availability of alternative treatment modalities.1–4 Wider implementation of PEA surgery in regions such as the Asia-Pacific is likely to have a significant medical and economic impact, given that around 60% of the entire world population reside in this region, and that the incidence of new CTEPH cases in the Asia-Pacific region is likely to exceed 50,000 per year.5,6 We sought to examine and poll, directly and anonymously, Asia-Pacific cardiothoracic surgeons who are interested in PEA surgery to determine their current demographics and practice and to reflect their opinions on future practice and how wider adoption of this operation might be enhanced.
Methods
Summary of survey questions.

Results
Participating countries.
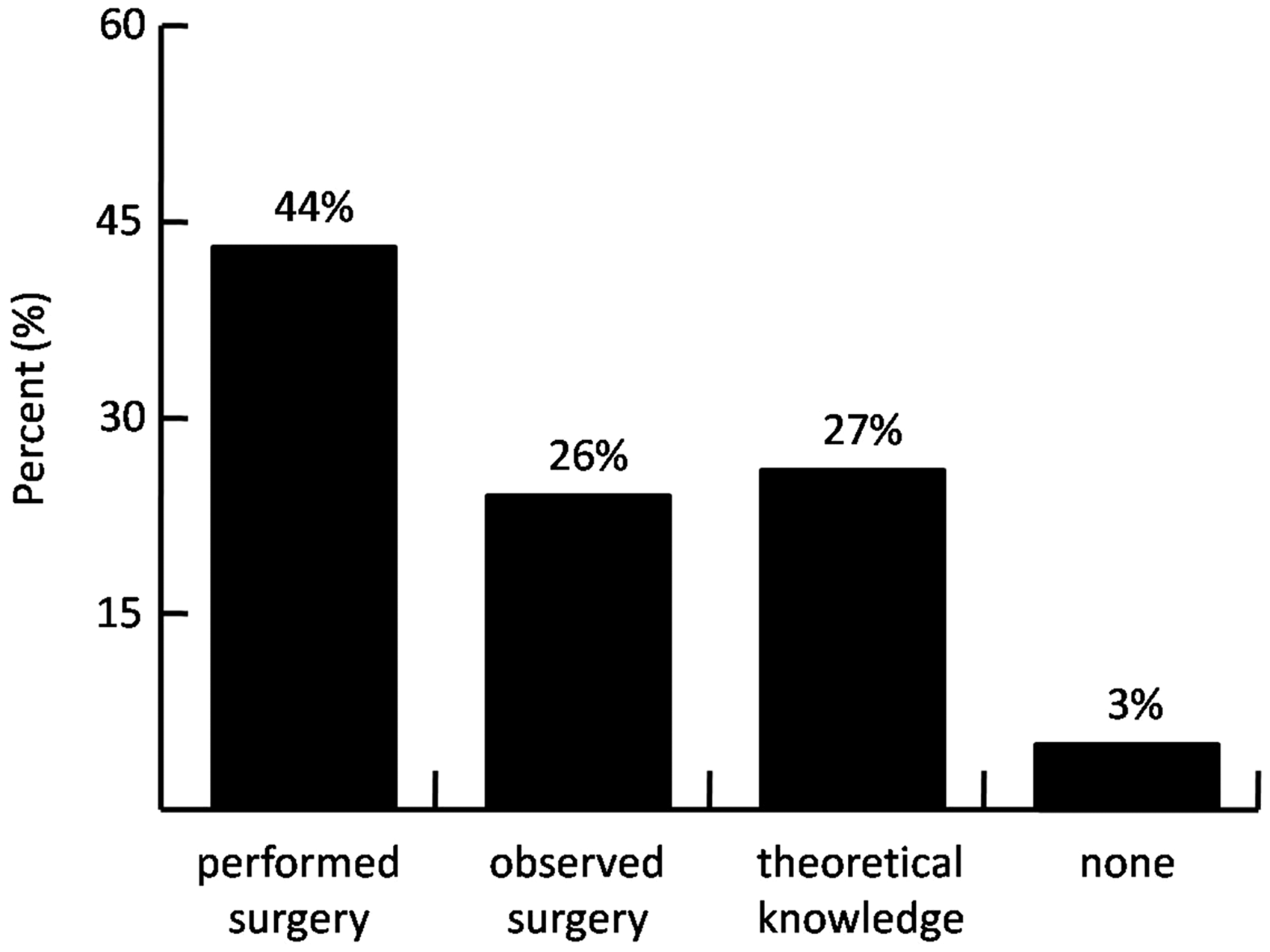
Present familiarity with pulmonary thromboendarterectomy surgery amongst respondents.
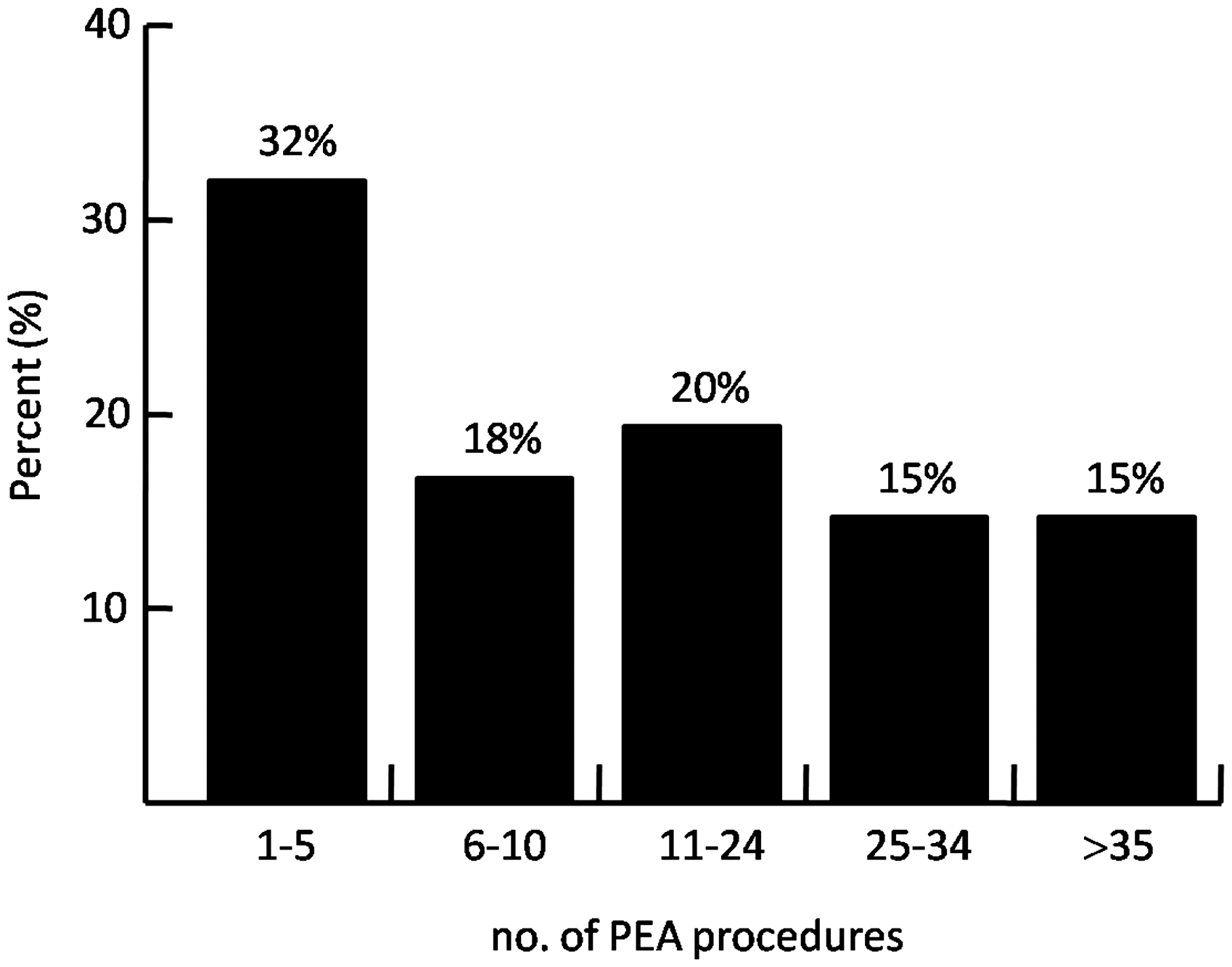
Number of pulmonary thromboendarterectomy (PEA) procedures performed by individual participants.
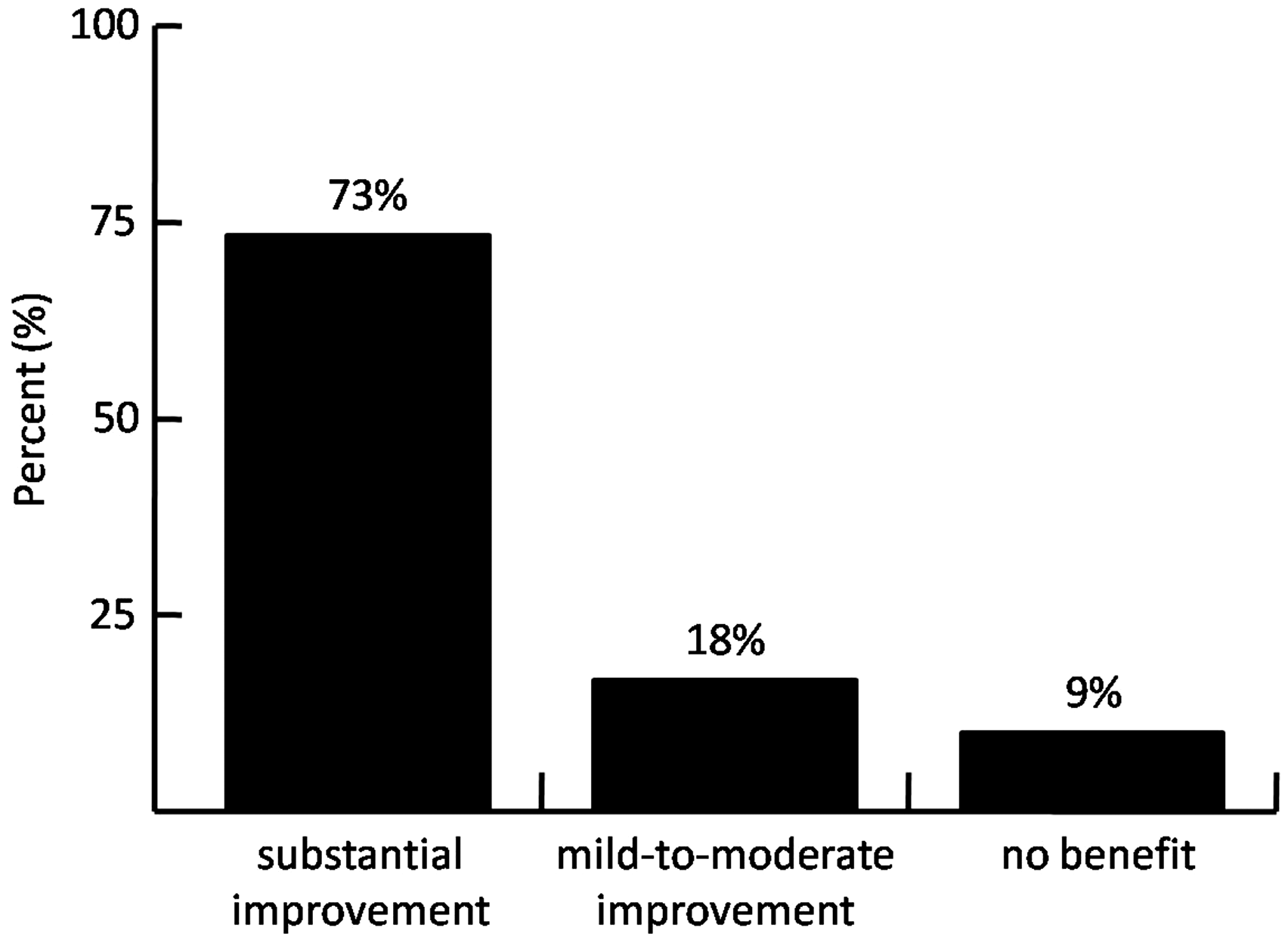
Reported functional outcome of pulmonary thromboendarterectomy operations performed by respondents.
Discussion
This survey aimed to describe the present practice of PEA surgery in the Asia-Pacific region. Despite wide awareness, PEA surgery has been performed by only a few Asia-Pacific surgeons and in small numbers of patients. Nevertheless, this study shows a clear predisposition to perform more PEA procedures in the foreseeable future, thus exponentially increasing the overall number of PEA procedures undertaken in the region.
The primary factor that might limit wider implementation of PEA surgery in the Asia-Pacific region was believed to be the difficulty in attracting suitable candidates for surgery. There was a broad conviction that this is the consequence of limited recognition of PEA surgery as a potential cure for CTEPH. It was also believed that dissemination of PEA surgery may be held back by certain country-specific and center-specific issues, such as local medical practices and the availability of resources. Indeed, the challenge of attracting potential candidates for PEA surgery in a resource-limited setting was recently highlighted in the first report on the CTEPH experience in Mexico, where only one patient in fifty could undergo PEA surgery. 7 Of note, PEA surgery was already being performed in many centers that did not have heart/lung transplantation or ECMO capabilities, and this indicates a lack of agreement among Asia-Pacific surgeons regarding the necessity for such resources.
Despite the evident need for substantially wider implementation of PEA surgery in the region, this opinion poll among Asia-Pacific surgeons underscores their preference to restrict this procedure to designated “expert PEA centers” (already defined as institutions that perform ≥20 PEA surgeries per year with a mortality rate < 10%).5,8 In line with previous reviews,1,6,9,10 it was widely believed that expert PEA centers can carry out optimal patient selection and better perioperative management compared to less experienced centers. Considering the dissemination of the operative technique, the majority of respondents also recognized the importance of the early learning curve, and considered that a surgeon should be supported by a colleague with considerable earlier experience in PEA surgery before operating independently.
Finally, the opinion poll acknowledged the need to organize dedicated PEA regional meetings where live demonstrations and local outcomes can be presented. In addition, these conferences can serve as platforms where clinical practice guidelines can be established and updated as appropriate for regional healthcare facilities. Such efforts were expected to enhance wider acceptance of the PEA surgery in the region in the projected future, and were equally thought likely to translate into generalized benefits for local patients.
Several limitations of this study should be considered when interpreting these data. The voluntary and anonymous nature of any survey may possibly generate incomplete or even questionable records that can influence epidemiological data. However, we believed that anonymity was a positive feature of this survey because it encouraged the participation of surgeons with limited experience or poor outcomes, as was evident in the results of the survey. Moreover, a realistic number of surgeons took part in the study, and they were based in equal percentages in university, government, and private practice institutions. Hence, we believe that this survey represents the overall state of PEA surgery in the Asia-Pacific region fairly well, and reflects the opinions of the largest contemporary group of surgeons with an interest in PEA surgery. Even though differences between individual countries undoubtedly exist in parallel with discrepancies in the development of health services, 11 the anonymous nature of survey design did not permit per country analyses nor identification of existing expert PEA centers. Bringing attention to certain institutions was not the purpose of this survey. We concluded that although cardiothoracic surgeons in the Asia-Pacific region appreciate that a lot of work is needed before PEA surgery is widely adopted, it is clear that many surgeons and additional institutions are already planning to implement the PEA procedure. To this end, bringing together an international working group on PEA in the Asia-Pacific region is currently ongoing, and is specifically dedicated to share experiences and advance the understanding of the practice and results of PEA surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.