
Abstract
The patient was a 56-year-old woman with Kommerell’s diverticulum associated with a right-sided aortic arch with mirror-image branching. No other congenital heart anomalies or vascular rings were observed. Descending aortic replacement through a right posterolateral thoracotomy was performed to eliminate the risk of diverticular rupture. The patient’s postoperative course was uneventful. This was a rare adult case of right-sided aortic arch with Kommerell’s diverticulum associated with no other congenital heart disease.
Keywords
Introduction
Kommerell’s diverticulum (KD) in an adult with right-sided aortic arch, without an associated aberrant left subclavian artery, is considered rare.1–5 KD is known to be a predisposing factor for diverticular rupture.1–4 Surgical management of such patients requires specific considerations because of the anatomical anomalies and obscured diverticular location through the surgical field.
Case report
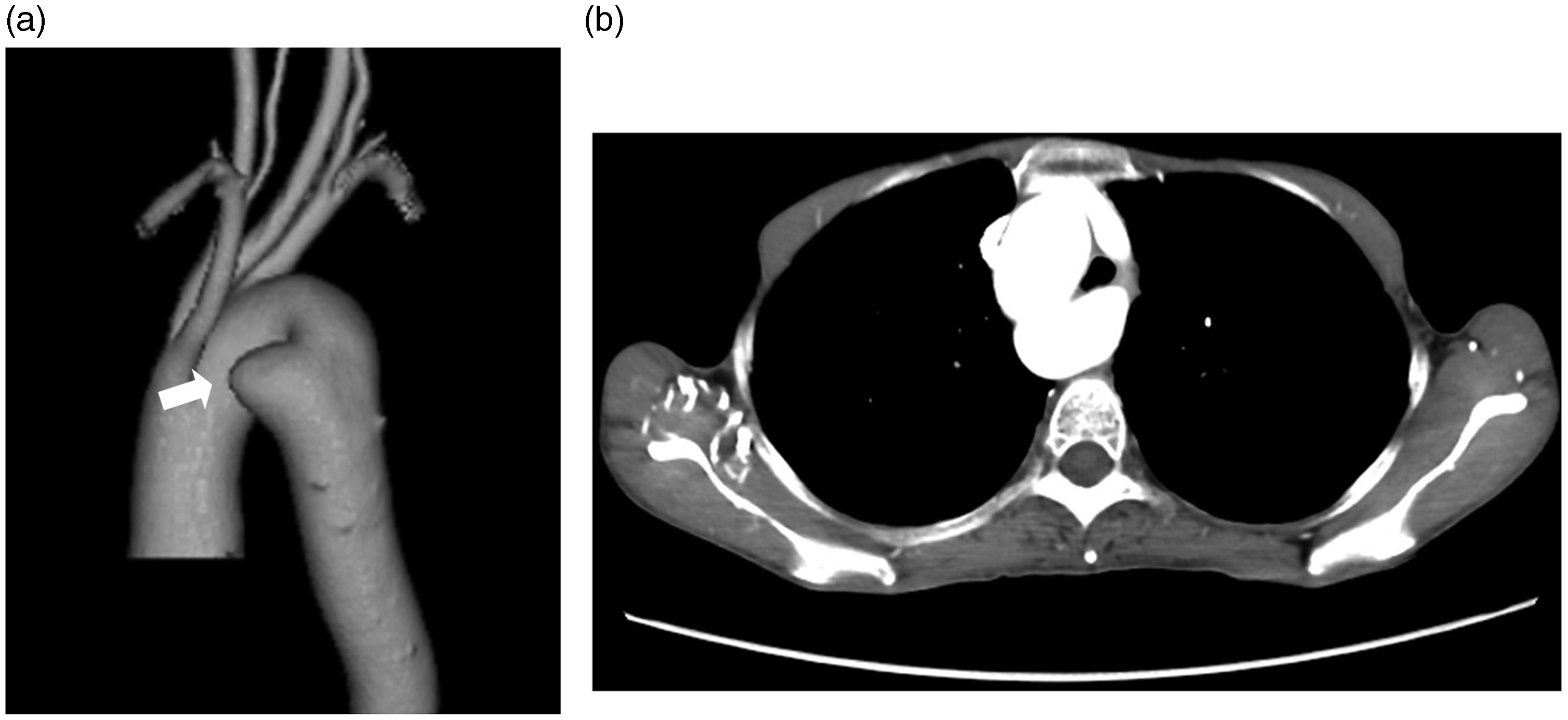
A 56-year-old woman with an abnormal chest radiograph was referred to our department. Contrast-enhanced computed tomography demonstrated a right-sided aortic arch with mirror-image branching (Figure 1). The left subclavian artery was morphologically normal, without an aberrant course. A KD (maximum diameter 35 mm) was demonstrated in the proximal descending aorta below the right subclavian artery origin (Figure 2a), extending between the vertebral column and esophagus (Figure 2b). Echocardiography showed normal cardiac function and no other valvular or congenital heart diseases or vascular rings. Coronary angiography was normal. Surgery was performed via a right posterolateral thoracotomy in the fourth intercostal space. Superficially, the KD could not be identified. The right recurrent and phrenic nerves were located. The azygos vein was ligated and divided. The descending aorta was dissected approximately 10 cm distal from the right subclavian artery origin. Then, as Figure 1 suggested, the aortic arch was carefully dissected between the origins of the right common carotid and right subclavian arteries. The right subclavian artery was dissected separately. Partial right femorofemoral bypass was used for distal perfusion. Normothermic half-flow bypass was maintained during aortic clamping. Vascular clamps were applied at all 3 dissected areas. A longitudinal aortotomy was used to enter the aortic lumen and expose the KD which arose from the left lateral aspect of the aorta. The internal aspect of the KD seemed to be normal without calcification. The KD was transected just distal to the origin of the right subclavian artery. The resected area was reconstructed with a 22-mm J-graft vascular prosthesis (Japan Lifeline, Inc., Tokyo, Japan) in an end-to-end fashion. The operation time was 256 min and the duration of bypass was 45 min. Postoperatively, the patient had an uneventful recovery without right recurrent nerve palsy, and computed tomography showed no residual aneurysm in the aortic arch (Figure 3). She has been doing well with regular outpatient follow-up.
Reconstructed contrast-enhanced computed tomography showing the front view of the right-sided aortic arch and its mirror-image branches. From the proximal side of the arch bifurcation, the left brachiocephalic artery (arrow), right common carotid, and right subclavian artery can be observed. The dotted line shows the proximal side of the dissection point on the aortic arch. Reconstructed contrast-enhanced computed tomography: (a) the rear view shows the right-sided aortic arch and Kommerell’s diverticulum (arrow), and (b) the axial view shows the Kommerell’s diverticulum (arrow) in the proximal descending aorta just below the aortic arch, extending between the vertebral column and esophagus. Postoperative contrast-enhanced computed tomography in axial view, showing that the Kommerell’s diverticulum had been completely resected and replaced with a prosthetic graft.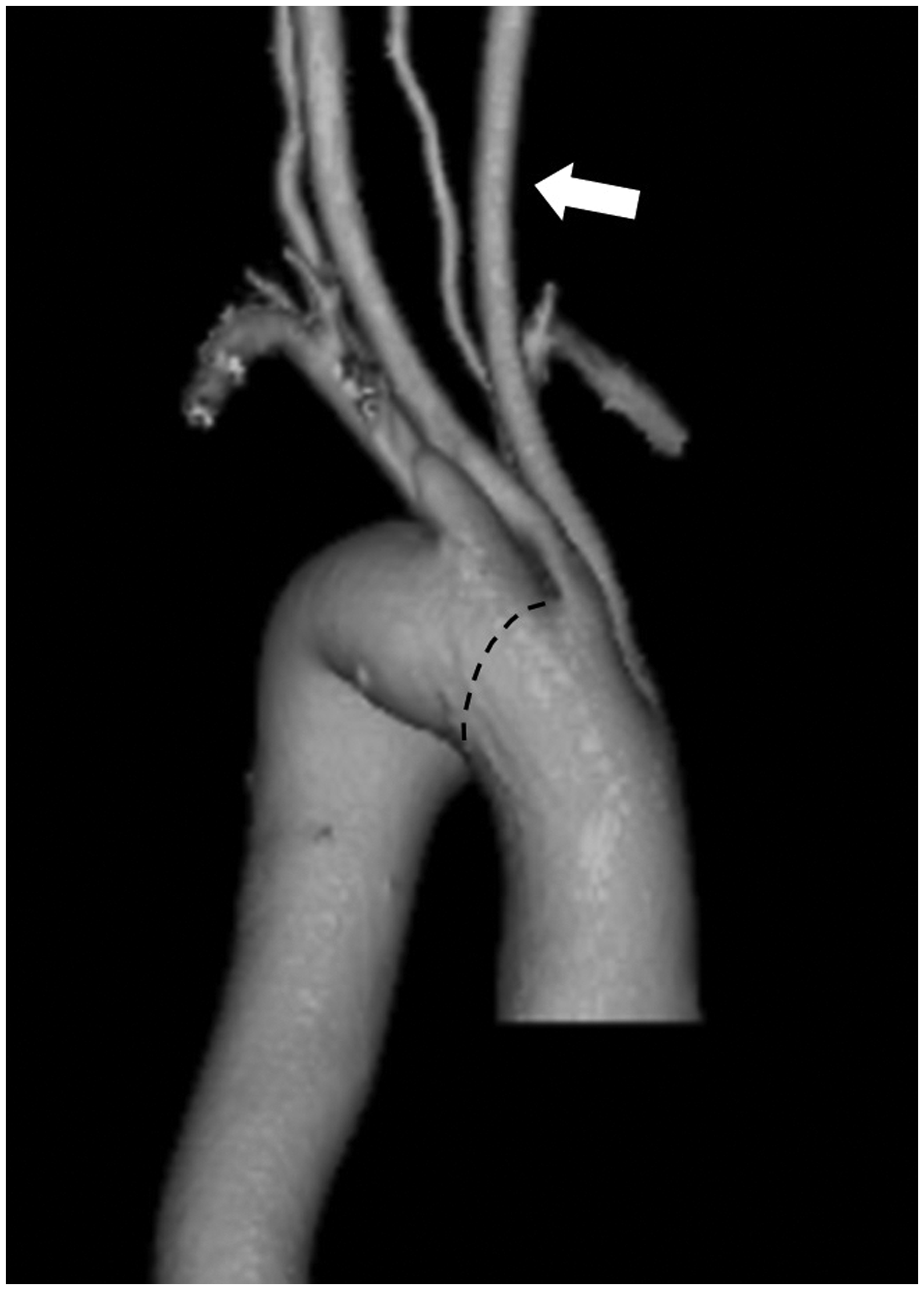

Discussion
Right-sided aortic arch with mirror-image branching occurs frequently with congenital heart anomalies such as tetralogy of Fallot;1–4 it is rare in the setting of an otherwise normal heart.1,4 A right-sided aortic arch, which may or may not be associated with branching abnormalities, results from a number of anomalies in development of the primitive aortic arch system during the embryonic period. 4 Given the rarity of KD, its management has not been established. KD is usually asymptomatic but is known to be a predisposing factor for aneurysmal formation, dilatation with compression of the trachea or esophagus, dissection, and rupture.1–5 Therefore, we believe that surgical treatment is necessary. However, such patients have specific serious problems, including anatomical abnormalities, KD location not visible in the operative field, or concomitant cardiovascular abnormalities. Careful preoperative evaluation is needed to identify these problems.
Various options have been considered for surgical management.1–6 The primary modality of treatment is open surgery. Recently, endovascular stent graft repair has emerged as an option. 5 In our patient, endovascular repair was considered initially. However, she was relatively young and the radius of curvature of the distal aortic arch around the KD was too small to apply endovascular therapy. 6 Therefore, open surgery was selected. A posterolateral thoracotomy through the fourth intercostal space with removal of the fourth rib provided excellent exposure of the aortic arch through the descending aorta. The KD could not be identified directly until the diseased area was opened. Therefore, it is important in deciding the dissection area to maintain sufficient distance from the expected location of the KD, especially on the proximal side. Careful dissection of the proximal side of the aortic arch is also important. The right recurrent and phrenic nerves were in mirror-image locations. These nerves pass over the aortic arch between the origins of the right common carotid and right subclavian arteries. These nerves were moved to the right side to avoid injury. Depending on the condition of the KD and the proximal or distal side of the aorta, deep hypothermia is not always necessary. Deep hypothermia in the setting of a posterolateral thoracotomy causes serious intrinsic problems such as hemorrhagic diathesis. Careful preparation of an appropriate cardiac support system for the management of unexpected intraoperative findings or bleeding due to anomalous anatomy is important.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.