
Abstract
Acute massive pulmonary embolism is known to be associated with high mortality, and treatment options may be limited if systemic fibrinolysis is contraindicated. We report the exciting results of a novel mechanical-pharmacological hybrid approach in 3 patients with life-threatening massive pulmonary embolism, in whom systemic fibrinolysis was contraindicated.
Keywords
Introduction
Acute massive pulmonary embolism is known to incur high mortality, and treatment options may be limited if systemic fibrinolysis is contraindicated. Local thrombolysis may still confer a risk of hemorrhage, with a particularly higher risk of hemorrhagic complications in the Asian population. We successfully treated 3 patients with massive pulmonary embolism in whom systemic fibrinolysis was contraindicated, using a hybrid technique of mechanical thrombectomy and ultrasound-accelerated thrombolysis with a low dose of a thrombolytic agent.
Case reports
Case 1
A 68-year old Chinese woman with metastatic corpus cancer suffered loss of consciousness at home. On admission, she was hypotensive and found to have a deep vein thrombosis in the left superficial femoral vein. Computed tomography (CT) confirmed massive bilateral pulmonary emboli (PE), but systemic fibrinolysis was contraindicated due to a decrease in hemoglobin (from 10.8 to 7.7 g dL−1 within a month) and concerns of bleeding in the bowel. She also had right heart strain on CT, with elevated troponin I (90.3 ng L−1). She was successfully treated by a hybrid technique (Figures 1 and 2). Pulmonary arterial pressures were 30/20 and 30/12 mm Hg pre- and post-procedure, respectively. She was monitored in the critical care unit for two days, and discharged after 1 month.
Pulmonary angiography revealing a large filling defect (thrombus) in the main pulmonary artery (arrow) and some of the left segmental pulmonary arterial branches, with significantly reduced perfusion, especially in the right lung. Repeat pulmonary angiogram 24 hours after the hybrid technique, showing a significant reduction in thrombus burden, with marked restoration of right pulmonary arterial blood flow.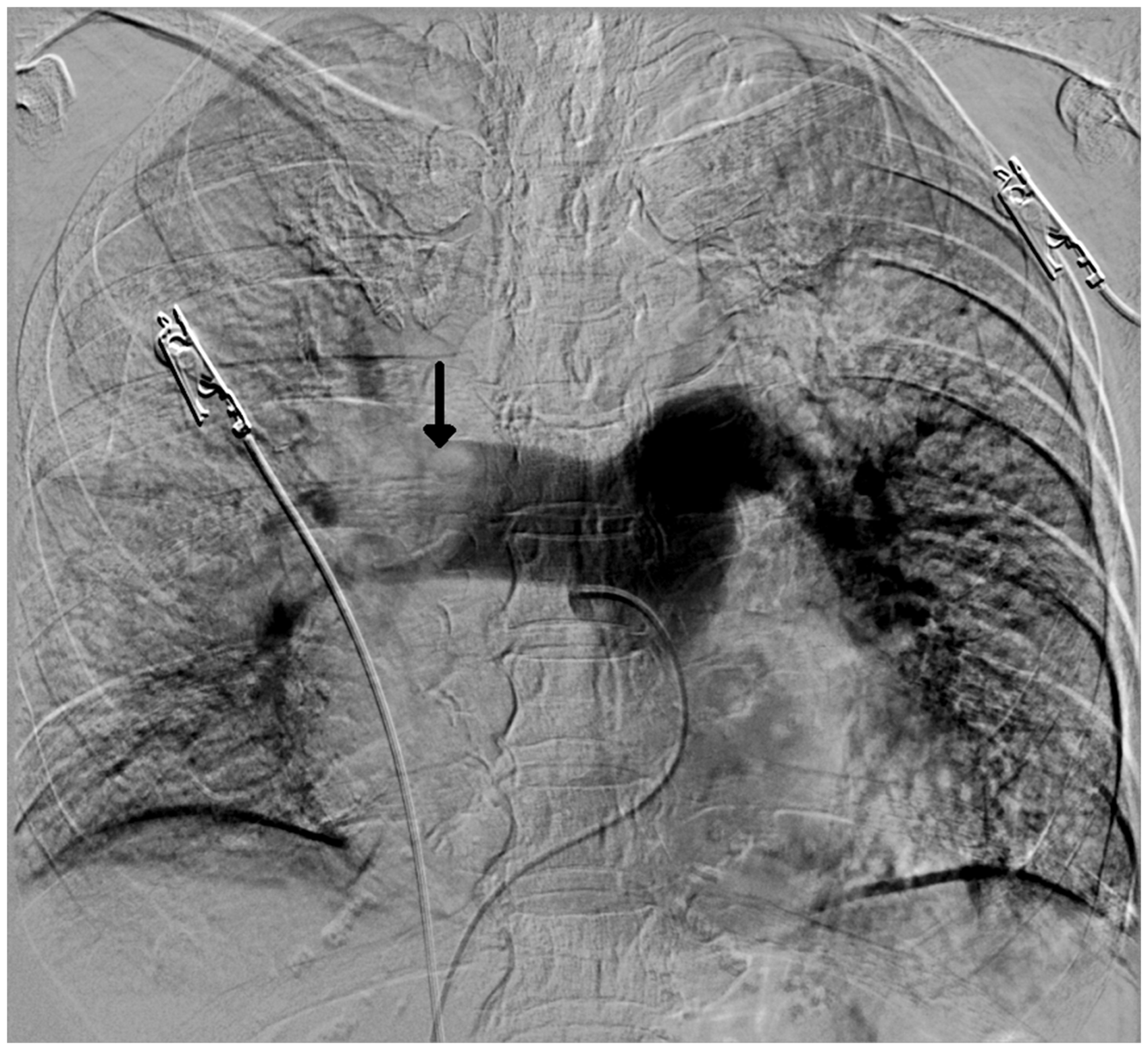

Case 2
A 51-year-old Chinese gentleman with intracranial bleeding after burr hole drainage and prolonged confinement to bed for two weeks, had sudden desaturation in the ward. Massive bilateral PE was confirmed by CT pulmonary arteriography, which was attributed to a left leg deep vein thrombosis. Right heart strain was associated with elevated troponin I (95.7 ng L−1). The patient was effectively treated with the hybrid technique, and discharged from the critical care unit 1 week later.
Case 3
A 70-year-old Chinese gentleman suffered cardiac arrest at home, with pulseless electrical activity for 16 and 5 min. He was successfully resuscitated. Subsequent CT confirmed massive PE. Systemic thrombolysis was contraindicated due to traumatic acute subdural hemorrhage after the arrest and loss of consciousness. The patient was treated by the hybrid technique uneventfully, extubated, and discharged from the critical care unit 1 week later.
Discussion
The hybrid technique is a combination of mechanical thrombectomy and catheter-assisted intra-pulmonary artery thrombolysis. All 3 patients had right common femoral vein access. We confirmed the absence of thrombus in the inferior vena cava by CT or angiography before proceeding with right heart catheterization. A 0.035-inch Terumo guidewire was placed in the main pulmonary trunk, over which a 4F Simmons I catheter was fed. Pulmonary angiography was performed and mean pulmonary artery pressure was measured via this catheter. It was exchanged with a long 8F steerable guiding sheath (Destino Reach; Oscor, Inc. Palm Harbor, FL, USA) with the tip positioned in the main pulmonary artery or a right or left branch. The first two patients were treated with an Indigo Mechanical Thrombectomy System (Penumbra, Inc., Alameda, CA, USA), and the third was managed with an Aspirex Mechanical Thrombectomy Device (Straub Medical AG, Wangs, Switzerland). The aim was to create partial or total recanalization of the blocked pulmonary arterial segments. This procedure was considered successful when the subsegmental branches became visible behind recanalized pulmonary artery segments. All 3 patients were subsequently treated with an EkoSonic ultrasound-accelerated thrombolysis system (EKOS Corp., Bothell, WA, USA) with its tip located beyond the thrombus to infuse low-dose recombinant tissue-type plasminogen activator (alteplase 0.5 mg hourly for 24 h; total dose 12 mg). Pulmonary angiography was repeated 24 h post-procedure, inferior vena caval filters were inserted after reevaluation of the pulmonary angiogram, and the patients were put on long-term anticoagulation.
The overall mortality rate associated with massive PE is as high as 50%. 1 While catheter embolectomy and fragmentation are reasonable treatment options for massive PE, systematic thrombolytic therapy is contraindicated according to the 2011 American Heart Association guidelines. Our center follows this guideline, yet mortality in the last two years was 45.5% (5/11) in patients with massive PE who received catheter embolectomy exclusively. Thus mechanical thrombectomy alone may not be sufficient to treat these critical patients. Hybridized techniques of catheter-assisted thrombectomy with local thrombolysis have been described. 2 The purpose of mechanical thrombectomy is to canalize perfusion channels to the lung and ameliorate severe right heart strain while allowing time for thrombolysis to occur. Nevertheless, local thrombolysis may still confer a risk of hemorrhage in other organs, compounded further by the higher risk of hemorrhagic complications in the Asian population. 3 Therefore, we incorporated ultrasound-accelerated thrombolysis which allows a lower dose of fibrinolytics and shorter infusion time to achieve clinically effective outcomes while minimizing the risk of side-effects.4,5 No patient suffered a fibrinolysis-related hemorrhage, and all survived their massive PE.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.