
Abstract

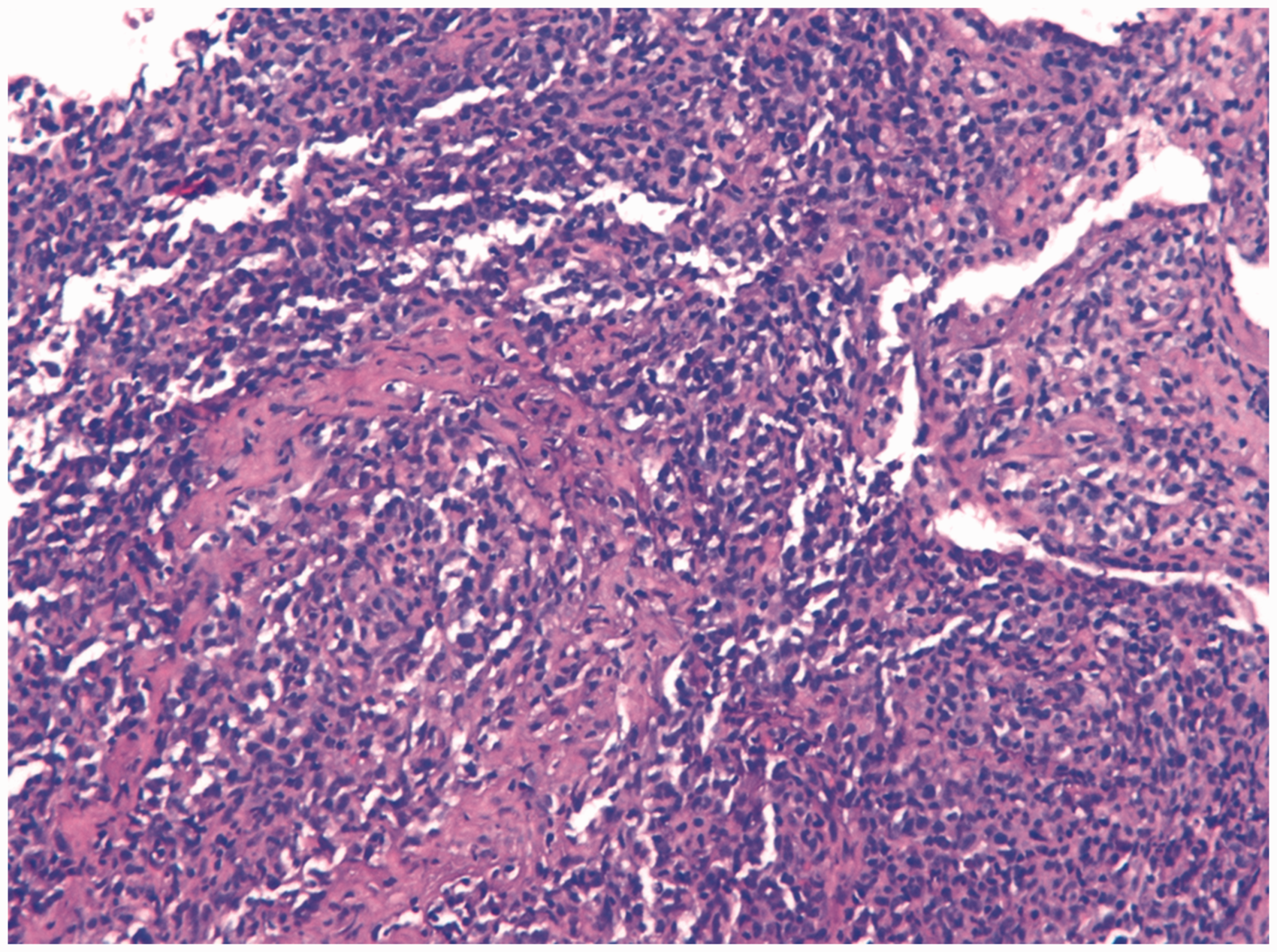
Chest radiography in an 84-year-old woman with shortness of breath showed multiple pulmonary opacities (Figure 1A). Computed tomography confirmed bilateral pulmonary nodules and masses, the majority of which had air bronchogram, as well as a small right pleural effusion (Figure 1B). A transbronchial biopsy did not demonstrate malignant cells, and a right thoracentesis revealed only a lymphocyte-rich exudate with benign-appearing polyclonal lymphocytes. One of the larger opacities was biopsied percutaneously with a 16G coaxial core needle biopsy system under computed tomography guidance (Figure 1C). The 3 samples obtained showed diffuse infiltration by CD20-positive atypical B-cells (Figure 2), which were strongly positivity for Epstein-Barr virus encoded RNA. The diagnosis was grade 3 lymphomatoid granulomatosis (LG). The patient responded favorably to chemotherapy (cyclophosphamide, vincristine, and prednisone plus rituximab). LG is a rare Epstein-Barr virus-associated angioinvasive B-cell lymphoproliferative disorder (seen in various immunodeficiency states) that involves the lungs in most cases. Symptoms include cough, fever, malaise, and weight loss. In recent reports, a definitive histological diagnosis of pulmonary LG was made by surgical biopsy or after several attempts at transbronchial or percutaneous biopsies. Our case is interesting because the diagnosis of pulmonary LG was made by computed tomography-guided percutaneous lung core needle biopsy.
(A) Chest radiograph showing multiple opacities in both hemithoraces (arrows). (B) Axial thoracic computed tomography showing multiple bilateral nodules and masses (asterisks) with air bronchogram (arrows). Note the presence of a right pleural effusion. (C) Axial thoracic computed tomography demonstrating the biopsy procedure (arrows). Lung biopsy specimen revealing massive infiltration of the lung parenchyma by medium to large atypical monotonous lymphocytes with an angiocentric distribution. Hematoxylin and eosin stain, original magnification ×200.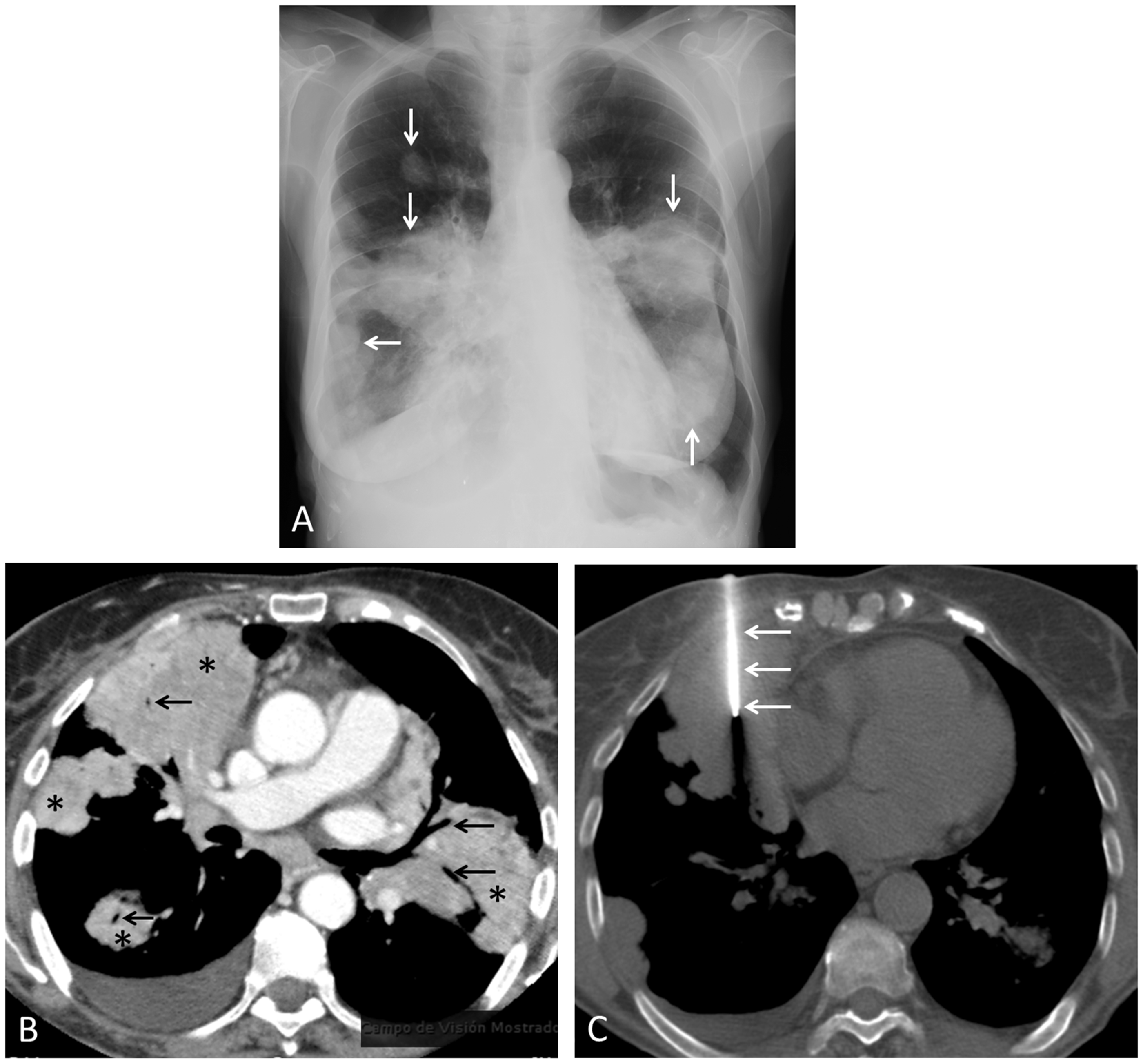
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.