
Abstract
Cardiac myxomas are rare tumors. Esophageal adenocarcinomas are common tumors of the gastrointestinal tract. Simultaneous occurrence of these tumors has not been reported. A 52-year-old gentleman presented to our hospital with dysphagia and was diagnosed with esophageal adenocarcinoma. Routine echocardiography discovered a cardiac tumor in the left atrium. The cardiac tumor was surgically removed and biopsy confirmed a myxoma. We removed the cardiac tumor as the first step and then initiated neoadjuvant chemotherapy. It is ideal to constitute a multidisciplinary team to decide on the course of treatment in such cases.
Introduction
Primary cardiac tumors are extremely rare, with an incidence of 0.3% to 0.7% of all cardiac tumors. 1 Most primary cardiac tumors are benign, and nearly half are myxomas. 2 Cardiac myxomas have been reported with lung and colorectal carcinoma.3,4 We report a case of gastroesophageal junction adenocarcinoma with left atrial myxoma.
Case report
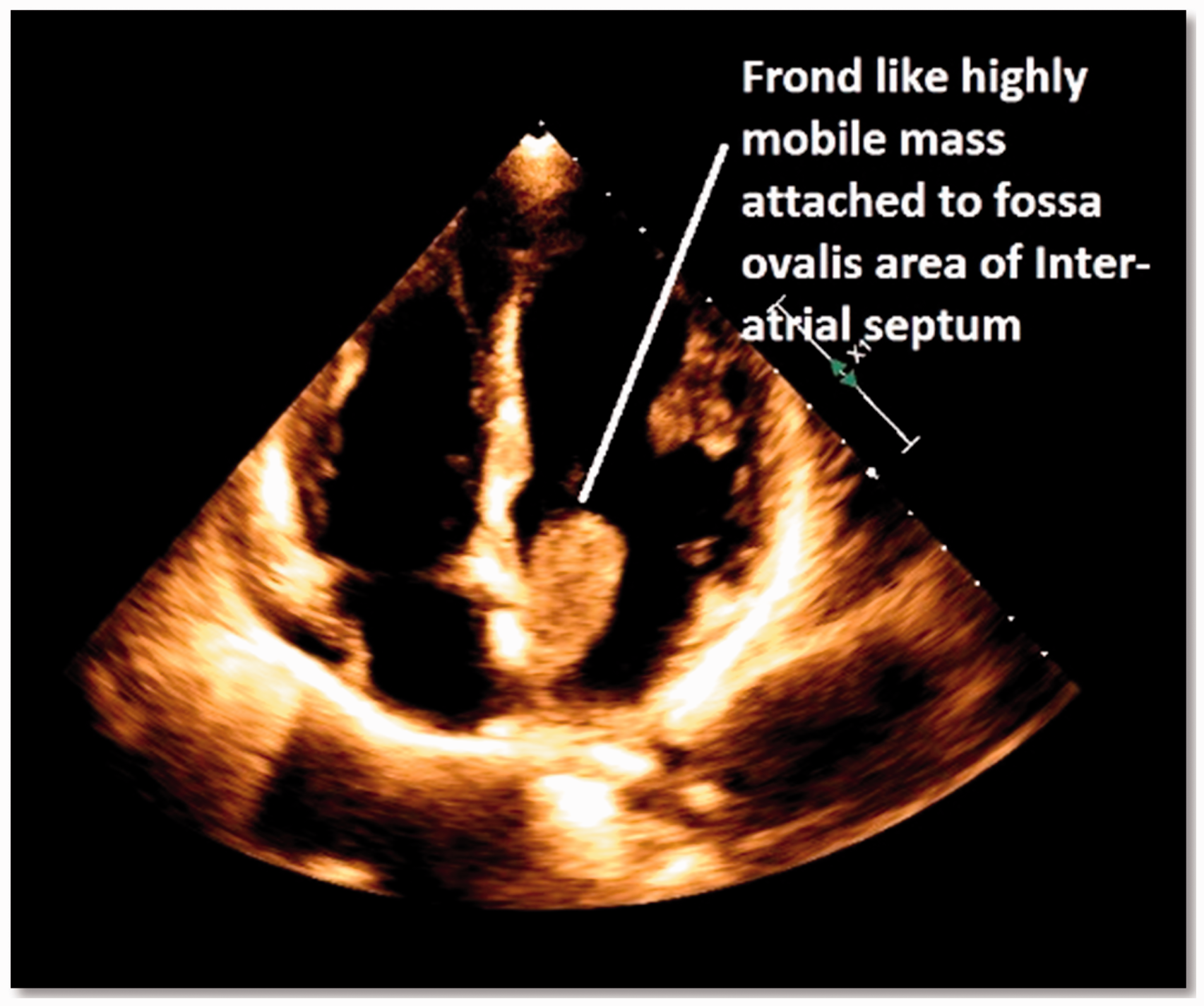
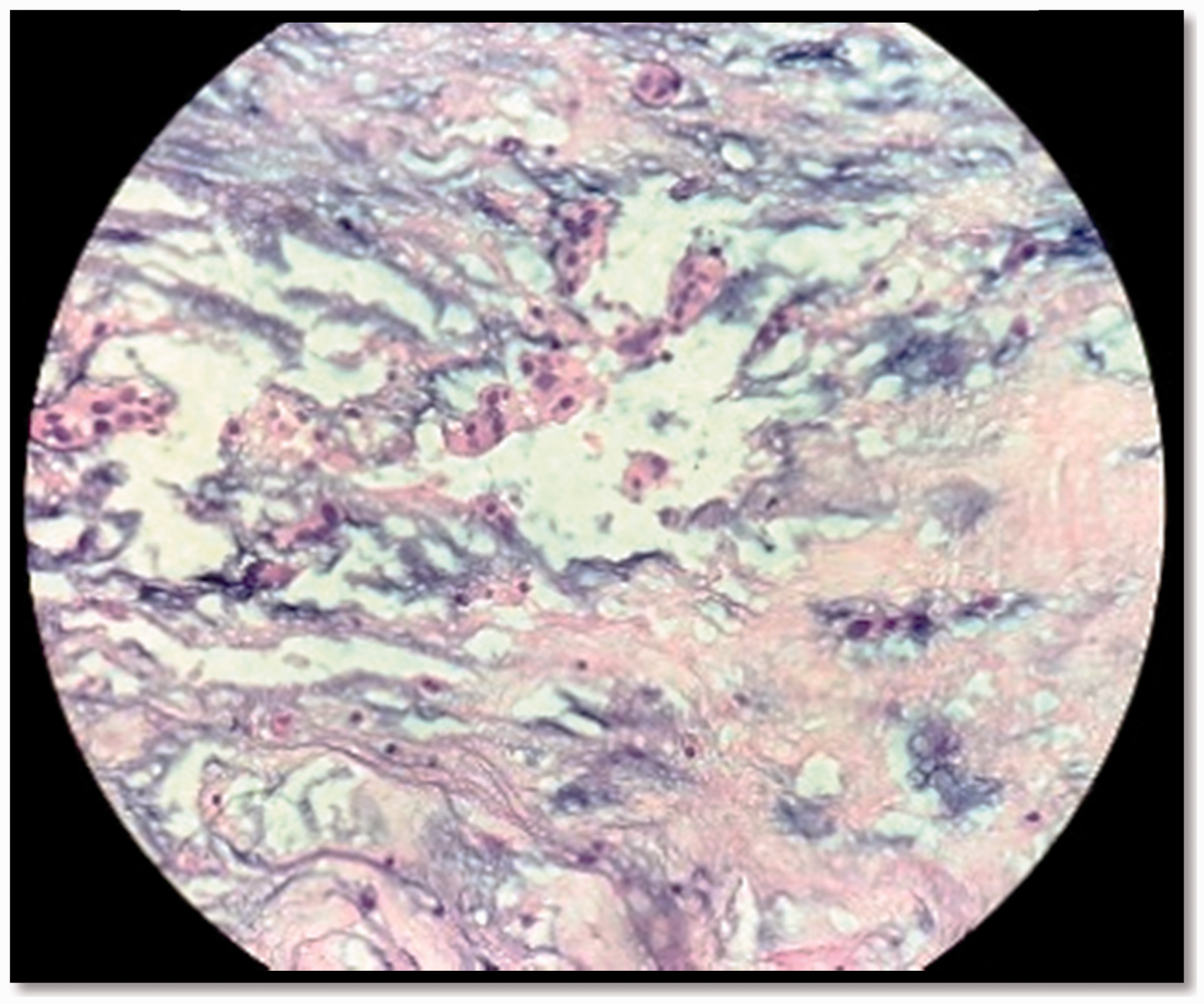
A 52-year-old gentleman with no comorbidities presented with progressive dysphagia for 6 months and odynophagia for 8 days. He had never smoked, and consumed alcohol occasionally. Examination was unremarkable except for temporal wasting. Contrast-enhanced computed tomography of the abdomen was reported as circumferential mural thickening involving the gastroesophageal junction with extension along the lesser curvature of the body region. Mild proximal dilatation of the esophagus was noted, however, oral contrast was seen to pass distally. Mild contiguous extension of the soft tissue thickening was noted medially involving the left crus of the diaphragm with encasement of the left gastric artery (Figure 1). The patient underwent upper gastrointestinal endoscopy that revealed an ulcerated friable growth at the lower end of the esophagus, extending across the gastroesophageal junction to involve the fundus. Biopsy revealed a moderate to poorly differentiated adenocarcinoma. Positron-emission tomography-computed tomography reported no metastatic lesions. Routine 2-dimensional echocardiography showed a mobile 24.7 × 21.6-mm mass attached to the inter atrial septum, with no significant valvular pathology and a normal ejection fraction (Figure 2). The findings were suggestive of a left atrial myxoma. The case was discussed by a multidisciplinary tumor board (cardiac surgery, medical, and cardiology teams were included). The decision was to treat the atrial myxoma before the gastroesophageal junction adenocarcinoma because of the risk of embolism posed by the myxoma. Left atrial myxoma excision was performed under cardiopulmonary bypass and general anaesthesia. The pathology laboratory reported a friable mucoid tumor measuring 2.5 × 3 × 1 cm with an attached base measuring 1.5 × 1.2 cm. Microscopic examination showed features of a myxoma (Figure 3). The patient was discharged, followed up in the oncology out-patient department, and started on neoadjuvant chemotherapy.
Computed tomography showing the gastroesophageal junction mass in longitudinal section. Echocardiography showing a friable mass in the left atrium, suggestive of atrial myxoma. Histopathology of the myxoma showing mesenchymal cells in a myxoid stroma.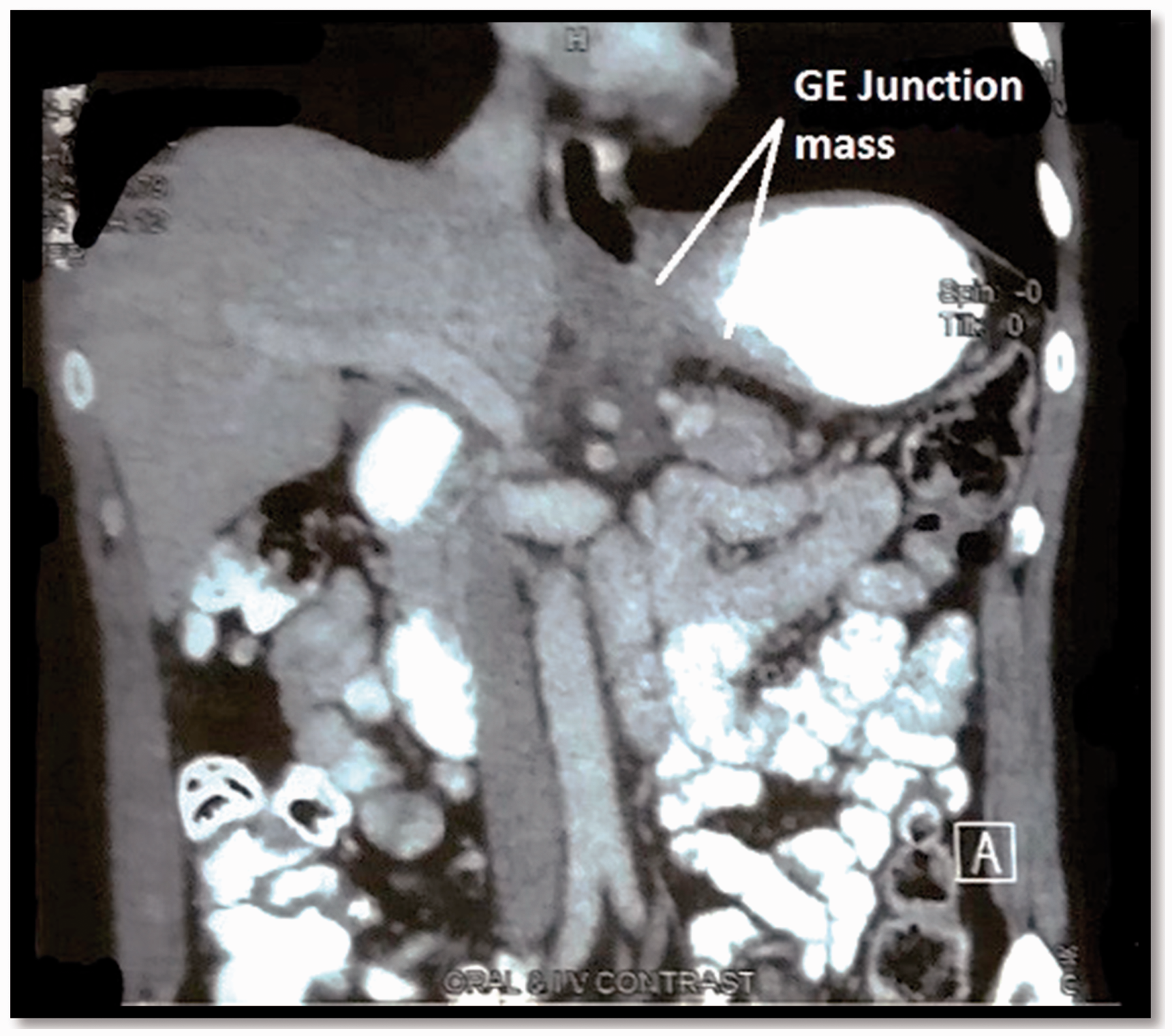
Discussion
There have been two cases of simultaneous occurrence of atrial myxoma and esophageal squamous cell carcinoma reported from China. 5 The patients underwent endoscopy and biopsy, which revealed squamous cell carcinoma. 5 Transthoracic echocardiography demonstrated a left atrial mass, confirmed to be a myxoma after excision. 5 The surgical approach used in both these cases consisted of entering the chest through an anterolateral incision, removing the atrial mass by a transseptal approach followed by esophagectomy via a thoracoabdominal approach. 5 Thus both tumors were removed in a single sitting.
Our patient was diagnosed with synchronous occurrence of esophageal adenocarcinoma and left atrial myxoma. Our approach to management was different. A multispecialty tumor board discussion decided that neoadjuvant therapy should be used for the esophageal malignancy. However, cardiac surgeons apprised the board of risk of sudden embolic events, and it was decided to surgically remove the atrial myxoma, followed by initiation of multimodality management of esophageal cancer. The delay of approximately 3 weeks entailed by cardiac surgery was considered acceptable by the tumor board, allowing for post-surgical recovery. Removal of the atrial myxoma was successfully carried out via a median sternotomy under cardiopulmonary bypass and general anaesthesia, with a smooth postoperative recovery. Our patient has now been started on neoadjuvant chemotherapy without concomitant radiation. It was deemed that the cardiac tissue would be exposed to significant radiation due to the particular location of the esophageal tumor. Surgery is the intended next step in treatment.
Concomitant occurrence of esophageal cancer with atrial myxoma is very rare. Gastroesophageal junction adenocarcinoma with atrial myxoma has not been reported previously. Various approaches for management of these tumors have been described when they occur in isolation, but no guidelines for management are available in the case of simultaneous occurrence. A multidisciplinary team approach and a decision based on the individual patient’s condition is prudent.
Footnotes
Acknowledgements
The authors thank Dr. Vandana Arora (Department of Pathology) for sharing the histopathology image, Dr. Swapnadeep Roy (Department of Cardiac Surgery), Dr. Sanjay Goel (Department of Cardiac Anaesthesia) for sharing the details of the surgery, and Dr. Gaurav Aggarwal (Unit head) for his constant guidance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.