
Abstract
Extranodal natural killer/T-cell lymphoma is a rare non-Hodgkin lymphoma that is divided into nasal, non-nasal, and aggressive/leukemia subtypes, according to anatomic origin and clinical manifestations, with each subtype carrying a different prognosis. We present a case of primary cardiac natural killer/T-cell lymphoma with extension to other organs in a 38-year-old man, to highlight the role of imaging in categorizing nasal versus non-nasal types. This distinction has relevant implications for patient care because the non-nasal type has a much lower survival rate.
Keywords
Introduction
Primary cardiac natural killer (NK)/T-cell lymphoma is a rare form of extranodal lymphoma. While cardiac involvement in lymphoma is frequent, primary cardiac lymphoma is unusual and often associated with diffuse large B-cell lymphoma, 1 although extranodal NK/T cell lymphoma (ENKTL) is rarely present in the heart. Here, we present an exceptionally rare case of primary cardiac ENKTL with metastatic involvement of the lungs, kidneys, and gallbladder, as well as nasal area spared.
Case report
A 38-year-old Asian male presented to the emergency room with fever and substernal chest pain for several days, and atrioventricular block on an electrocardiogram. Laboratory tests showed increased D-dimer. Due to the clinical suspicion of pulmonary embolism, a computed tomography (CT) angiogram was performed. Although filling defects were not identified on CT, a radiological diagnosis of septic embolism was proposed. The study was initially suboptimal for evaluation of the cardiac mass. On admission, a transesophageal echocardiogram revealed an ill-defined mass in the right atrium. Cardiac magnetic resonance imaging and CT with electrocardiogram-triggering were performed to further characterize the lesion. In both studies, the right atrium was seen to be invaded by an infiltrative lesion that extended superiorly to encase the aortic root and proximal right coronary artery, and to compress the superior vena cava at the cavoatrial junction (Figure 1). There was also nodular pericardial thickening with a small pericardial effusion. Given these findings, a working diagnosis of cardiac lymphoma was proposed. A whole body CT scan revealed a short interval increase in the number and size of the pulmonary nodules, as well as multiple hypodense lesions within the bilateral kidneys, and a nodular thickening of the gallbladder wall, suspicious for metastatic spread of the disease. The patient underwent pulmonary wedge resections of the left upper lobe and lingula. Pathology revealed nodular areas with neoplastic cellularity compatible with multifocal pulmonary involvement by ENKTL. Positron-emission tomography/CT (PET/CT) confirmed the findings of magnetic resonance imaging and CT, showing 18F-fluorodeoxyglucose accumulation in the cardiac mass, with a maximum standardized uptake value of up to 15.6 and slightly less in the pericardial and pulmonary nodules, gallbladder, and renal lesions (Figure 2). Otherwise, no evidence of hypermetabolic alterations suggesting lymphomatous involvement was found in the paranasal sinuses.
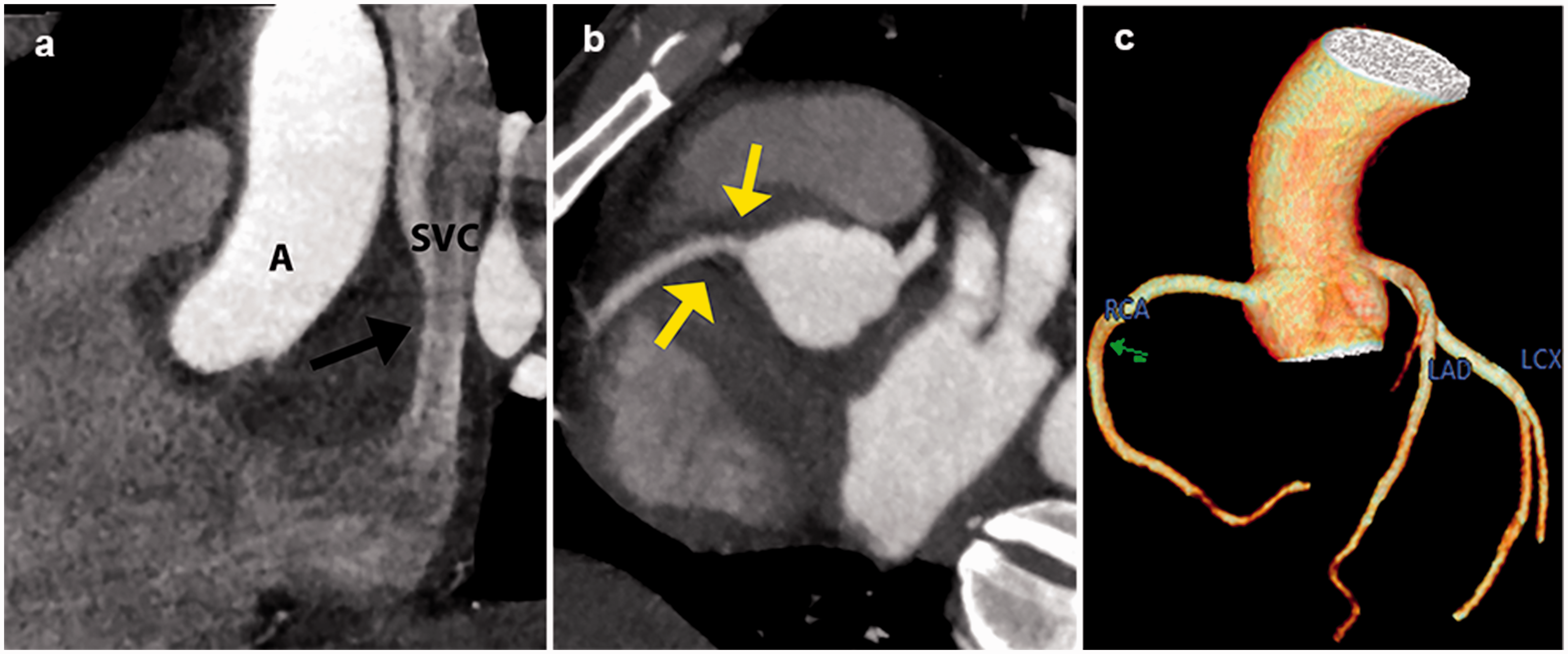
Cardiac computed tomography to assess the cardiac mass. (a) Oblique sagittal plane demonstrating a mass in the right atrium, spreading along the aortic root, and producing mild stenosis of the superior vena cava (arrow). (b) Maximum intensity projection of the coronary artery take-off where the mass encases the proximal right coronary artery (yellow arrows) without a real stenosis. (c) Volume-rendering confirming normal calibers of the coronary arteries.
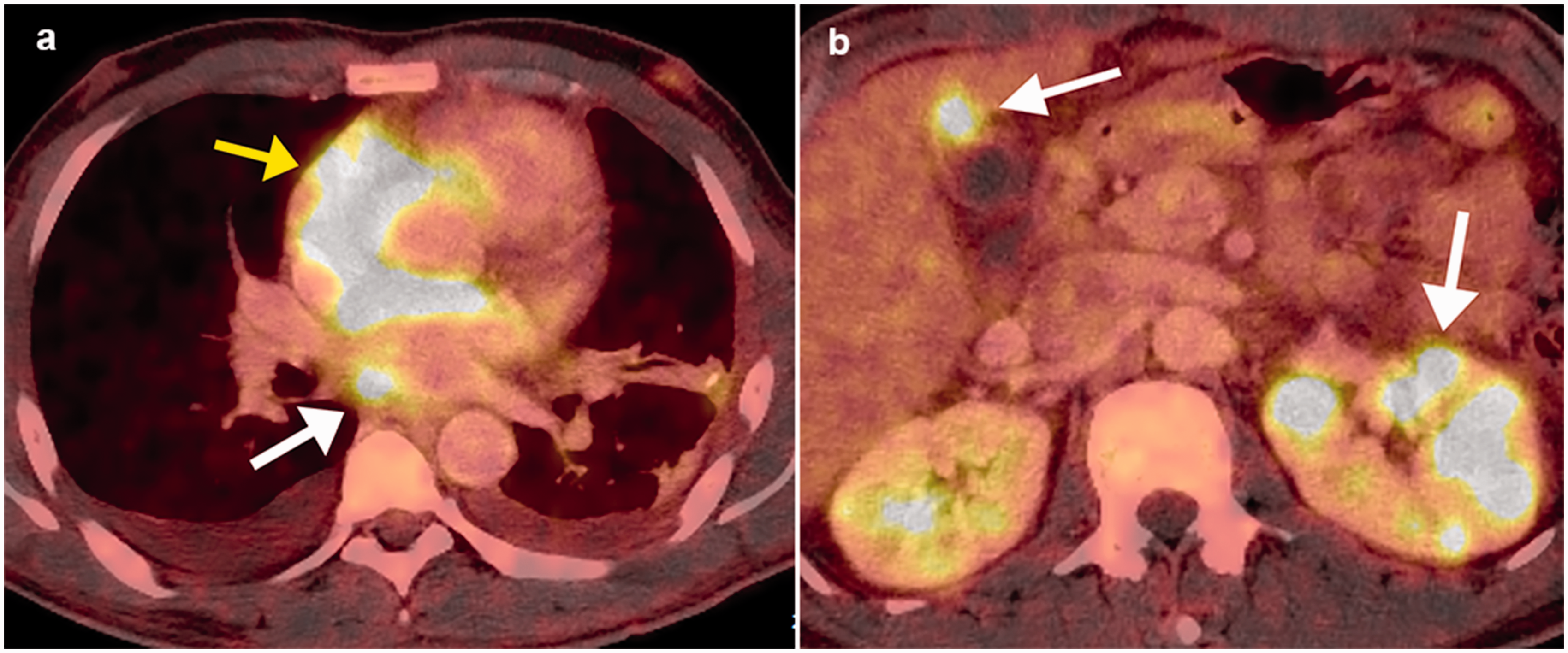
Whole-body contrast-enhanced positron-emission tomography computed tomography. (a) The cardiac mass (yellow arrow) and pericardial nodule (white arrow) with a maximum standardized uptake value of up to 15.6. (b) Transverse axis in a plane that includes lesions of the gallbladder and left kidney.
Discussion
Some autopsy series have shown that approximately 30% of patients with non-Hodgkin lymphoma had cardiac involvement. However, primary cardiac involvement is extremely rare, accounting for only 1.3% of cardiac tumors and 0.5% of extranodal lymphomas.2,3 In a review issued by the WHO for the classification of lymphomas in 2016, NK cell lymphomas are divided into two groups: ENKTL, nasal type; and aggressive NK cell leukemia/lymphoma. Clinically, they are still divided into 3 variants according to their manifestations: nasal (68%), non-nasal (26%), and aggressive lymphoma/leukemia subtypes (6%). Many cases have been described in which ENKTL primarily affects extranasal regions such as the skin, gastrointestinal tract, lungs, soft tissue, testicles, and central nervous system. 4 On the other hand, involvement of distant organs in the primary nasal subtype is found in less than 10% of patients at the time of diagnosis. 5 Nevertheless, with the advent of PET/CT, many of the cases initially considered to be non-nasal have now been found to demonstrate hidden nasal involvement. Therefore, the ENKTL non-nasal type may represent systemic spread of the nasal type, which may explain the poor response to treatment of this subtype of lymphoma and the worse prognosis. Thus a strict definition of non-nasal NK/T-cell lymphoma requires exclusion of a hidden nasal primary lesion by PET/CT. 6
In our case, nasal involvement was ruled out by PET/CT, therefore, we can consider it to be a case of true non-nasal lymphoma with primary cardiac involvement, which is exceptionally interesting, taking into account that in the English-language literature reviewed thus far, only one case of ENKTL with cardiac origin has been reported. With regard to the imaging findings, it is not possible to differentiate whether lymphomatous involvement of the heart is due to the primary or secondary forms because their behavior may be identical. Currently, PET/CT has become necessary for the evaluation of lymphomas both at the time of diagnosis as well as in assessment of the response to treatment and early detection of relapse. In addition, PET/CT is crucial for the detection of metastatic disease when the disease is subclinical and not demonstrated on CT or magnetic resonance imaging.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.