
Abstract
Background
Small-cell lung cancer is a highly aggressive and metastatic epithelial lung malignancy. A small percentage of these tumors can be detected at an early stage and may be appropriate for surgical treatment. We analyzed the data of patients with early-stage small-cell lung cancer who underwent lobectomy and mediastinal lymph node dissection.
Methods
Between January 2011 and December 2016, 26 patients with early-stage small-cell lung cancer underwent lobectomy and mediastinal lymph node dissection and were included the study. The mean age was 60.9 years and 18 (69.2%) were male. Patients with increased uptake of 18 F-fludeoxyglucose in mediastinal or distant organs on positron-emission tomography computed tomography, or lung resections other than lobectomy, were not included in the study.
Results
The most common tumor location was the right upper lobe. The diagnoses were achieved by intraoperative frozen section study in almost all patients (92.3%). Mean overall survival was 58.5 ± 6.7 months (range 45–71 months) and the 5-year survival rate was 53%. We found that a statistically significant correlation between lymph node metastasis in N1 or N2 stations and survival. There was also a significant relationship between N2 nodal metastasis and recurrence.
Conclusion
As stated in the current guidelines, lung lobectomy and mediastinal lymph node resection should be considered in early-stage small-cell lung cancers. Survival outcomes of surgery for early-stage small-cell lung cancer are similar to the results in non-small-cell lung cancer.
Keywords
Introduction
Small-cell lung cancer (SCLC) is distinguished from other epithelial lung malignancies by feature such as rapid progression, early metastasis, and chemosensitivity. 1 SCLC constitutes 15%–20% of lung cancers, and distant metastasis is detected in approximately 60% of patients at the time of diagnosis. 2 Patients with SCLC have been treated with nonsurgical options for years because they were in a late stage when diagnosed. 3 Diagnostic procedures include thoracoabdominal computed tomography (CT), cranial magnetic resonance imaging, positron-emission tomography computed tomography (PET/CT), hemogram, serum electrolytes, liver function tests, and thoracentesis and cytopathology in the presence of pleural effusion (Figure 1). 4 Median survival for SCLC without treatment is reported to be 2–4 months. 5 In only 4%–12% of patients, can SCLC be detected in an early-stage as a solitary pulmonary nodule, and surgical resection may be possible. 6 Nowadays, lung lobectomy and mediastinal lymph node dissection is recommended in worldwide accepted guidelines, such as the American Society of Clinical Oncology, the European Society for Medical Oncology, and the National Comprehensive Cancer Network, for patients with early-stage SCLC without mediastinal lymph node metastasis, as surgical experience increases.4,7,8 In this study, we aimed to retrospectively review the data of patients with SCLC who were diagnosed early and treated with lobectomy and mediastinal lymph node dissection in our department.

A solitary nodule is seen in the right upper lobe on thorax computed tomography. The diagnosis was only made by a frozen section study intraoperatively.
Patients and methods
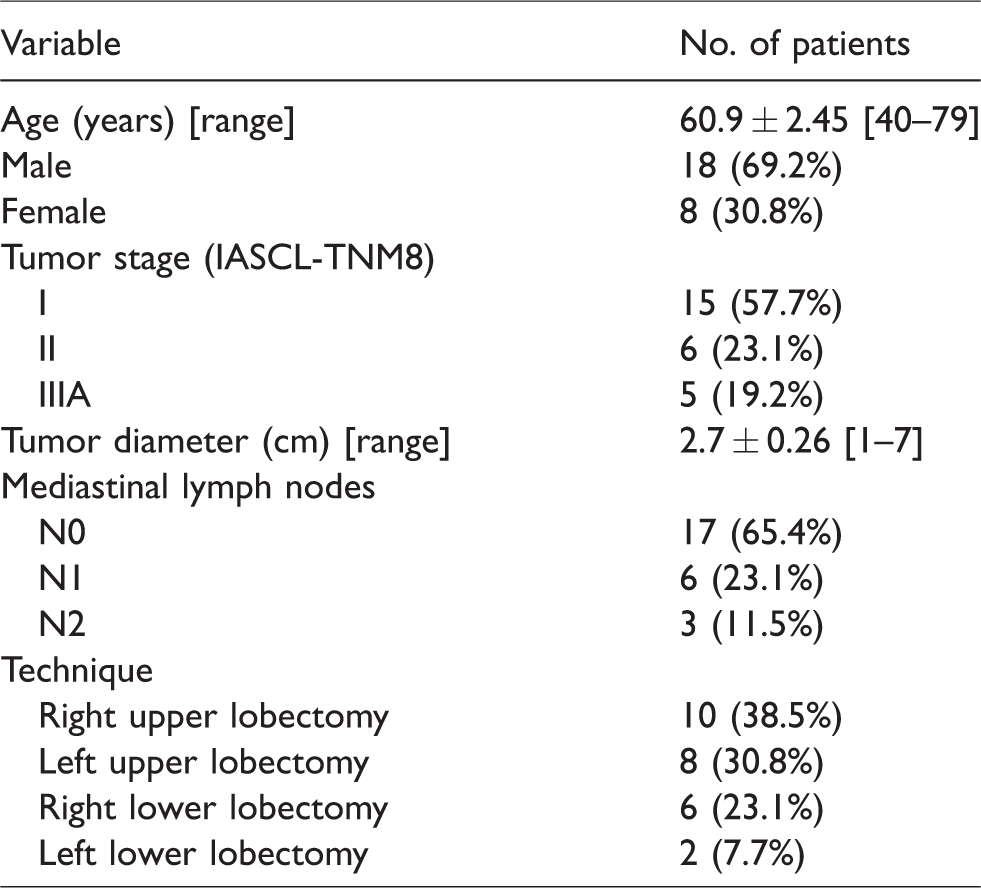
After approval of the local ethics committee, we retrospectively reviewed the data of 26 patients who underwent lobectomy and mediastinal lymph node dissection for SCLC in our department between January 2011 and April 2018. Patients with suspected mediastinal lymph node involvement or distant metastasis based on increased uptake of 18 F-fludeoxyglucose on preoperative PET/CT or those with more advanced than TNM stage 1 or who underwent lung resection other than lobectomy were not included in this study. Patients were analyzed according to age, sex, smoking habits, site of resection, number of mediastinal lymph nodes removed, clinical stage, pathological stage, general survival, 5-year survival, and mediastinal lymph node involvement. The clinicopathologic characteristics of the patients are given in Table 1.
Clinicopathologic characteristics of 26 patients with early-stage small-cell lung cancer.
SPSS for Windows version 20. 0 software (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The logrank (Mantel-Cox) test, Pearson’s chi-square test, and the Breslow (generalized Wilcoxon) test were used for comparisons. The Kaplan-Meier method was used for survival analysis.
Results
The most common location of the tumor was the right upper lobe (10 patients, 38.5%). The mean number of lymph nodes removed was 7.0 ± 0.4 (range 4–13) at N1 stations and 13.04 ± 0.6 (range 6–20) at N2 stations. The SCLC diagnosis was obtained from intraoperative frozen section analysis in 24 (92.3%) patients. Histopathological findings revealed mediastinal lymph node metastasis in 3 (11.5%) patients in N2 stations and in 6 (23.1%) in N1 stations. According to the IASLC-TNM 8 staging system, 15 (57.7%) patients were in stage 1, 6 (23.1%) were in stage 2, and 5 (19.2%) were in stage 3A. Overall survival was 58.5 ± 6.7 months (range 45–71 months), and the 5-year survival rate was 53% (Figure 2). There was a statistically significant difference in survival between patients with mediastinal lymph node metastasis (N1 or N2) and those without lymph node involvement (p < 0.05, Figure 3). Recurrence was similar in the N0 and N1 groups, but there was a significant relationship between N2 invasion and recurrence (p < 0.05, Figure 4). Furthermore, mediastinal lymph node metastasis was detected in 9 patients whose PET/CT scans showed normal activity in the mediastinal region.
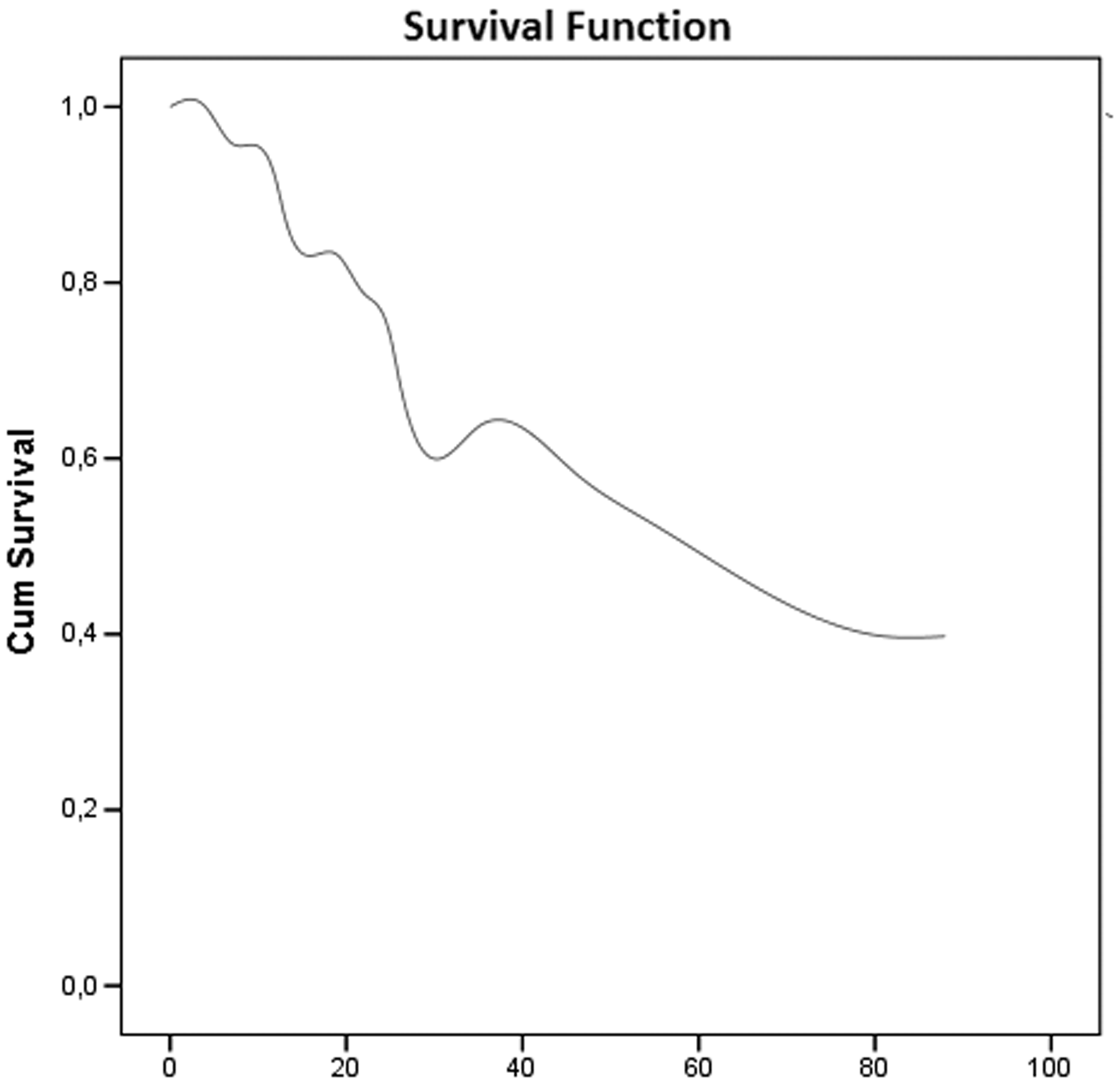
Overall survival.
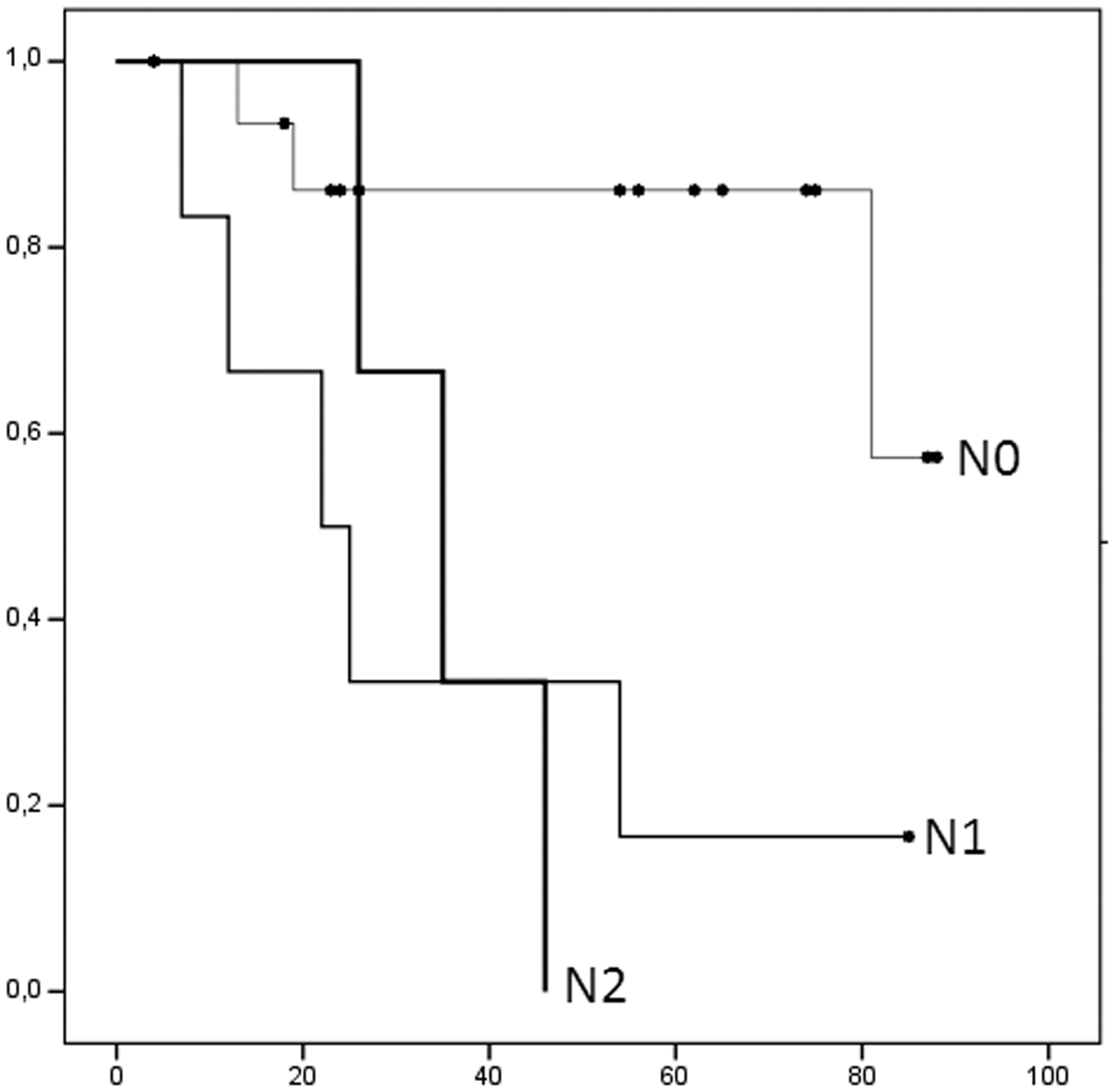
Comparison of survival according to mediastinal lymph node metastasis.
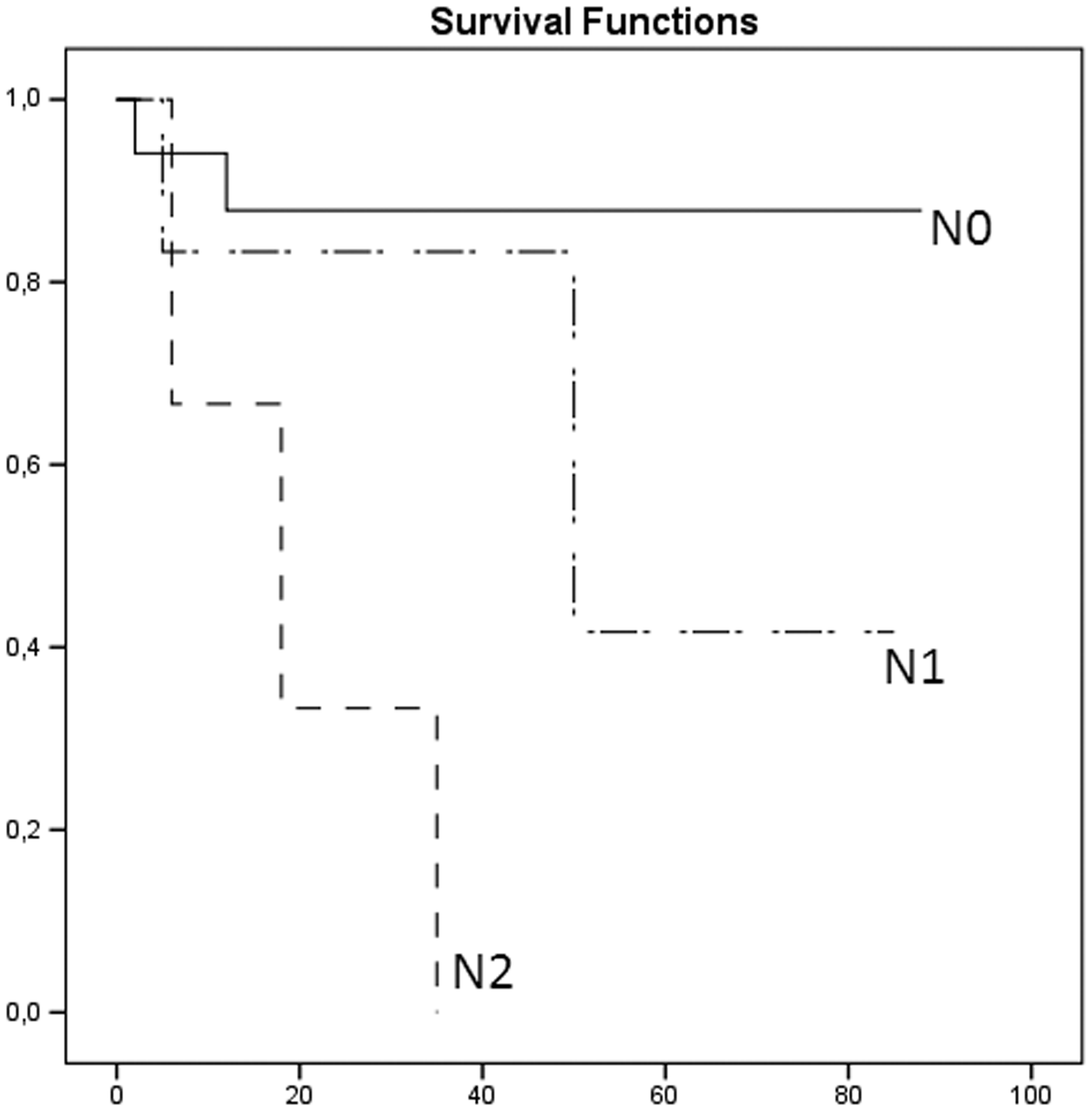
Recurrence rates based on mediastinal lymph node metastasis.
Discussion
SCLC is highly aggressive tumor and it has a poor mean survival time of 2–4 months without treatment. It accounts for approximately 15% of all bronchogenic carcinomas.1,5,9 A small proportion (4%–12%) of SCLC patients may be detected with a solitary pulmonary nodule that is suitable for surgical treatment. 5 The preferred treatment for SCLC patients in an early tumor stage without mediastinal lymph node involvement is a combination of surgery (lobectomy and mediastinal lymph node dissection) and adjuvant chemotherapy.4,7,8 Gaspar and colleagues 10 reported that surgery provides improved survival in patients with early-stage SCLC; patient in an early tumor stage and without mediastinal lymph node metastasis on thorax CT and PET/CT were included in our study. Almost all cases were diagnosed intraoperatively by a frozen section study. There is a close association between smoking and SCLC. Nearly all patients in our study had a smoking history, some were ex-smokers.
In the literature, the overall survival time of patients with SCLC without treatment has been reported as 3–6 months; it is 1–2 months in the advanced stage. 11 The 5-year survival rate was reported to be 21% to 58.3% in various studies including patients with early-stage SCLC who underwent lobectomy.6,12–18 Yu and colleagues 19 found a 5-year survival rate of 49.1% in patients who had a lobectomy. Brock and colleagues 12 reported the overall survival rate in patients with early-stage SCLC who underwent lobectomy and mediastinal lymph node dissection was 58%, and they found that the prognostic factors for survival were lymph node involvement and adjuvant chemotherapy. Weksler and colleagues 18 indicated that the survival rate was significantly better in patients who underwent surgery compared to the nonsurgical group in stage 1–2 SCLC, and they proposed surgical treatment for early-stage SCLC patients. Combs and colleagues 13 found that the 5-year survival rate of stage 1A SCLC patients who underwent lobectomy was 50%, with a significant decrease in survival after sublobar resection. Takei and colleagues 16 reported a 5-year survival of 52.6% and specified that the good prognostic factors were young age, female sex, early-stage tumor, and complete resectability. Hermes and colleagues 2 reported that serum lactate dehydrogenase was an independent risk factor, while age and sex did not affect the prognosis. There was no statistically significant relationship between sex, serum lactate dehydrogenase level, and 5-year survival in our study. The mean survival time in our study was 58.5 ± 6.7 months (range 45–71 months) and the 5-year survival rate was 50.3%, which is compatible with previous studies.
Adjuvant chemotherapy for patients without lymph node involvement and adjuvant chemoradiotherapy for mediastinal lymph node metastasis are recommended for early-stage SCLC in the 2018 National Comprehensive Cancer Network guidelines. 4 Survival analyses and treatment protocols were performed according to these guidelines in our patient group. Mean survival times according to mediastinal lymph node involvement were 76, 35.6, and 34 months for N0, N1, and N2, respectively. The relationship between mediastinal lymph node involvement and survival was found to be statistically significant. Surgical treatment is not recommended for SCLC patients who have mediastinal lymph node metastasis. 15 This was also confirmed in our study, and mean survival time in nodal metastatic patients was significantly worse than in node-negative patients. Unsurprisingly, almost all related studies have identified mediastinal lymph node invasion as a poor prognostic factor in small-cell carcinomas.4,12,13,20 Distant organ metastasis, especially brain metastasis, is not rare in patients with SCLC. Some authors have suggested that brain metastasis develops in nearly half of SCLC patients who live for more than 2 years, and the risk of metastasis is increased when survival is prolonged.21,22 Low and Ben-Or 6 reported that disease-free survival time was 29 months in surgically treated patients with SCLC. Stish and colleagues 15 noted 3-year disease-free survival after lobectomy or pneumonectomy and wedge resection for SCLC was 70% and 16%, respectively. Ipsilateral or contralateral lung or distant organ metastases were detected in in 8 of the 26 patients in this study; mean disease-free survival was 62.0 ± 7.3 months. According to mediastinal lymph node metastasis, the disease-free interval in N0, N1, and N2 patients was 73.3, 57, and 19.6 months, respectively. Although there was no statistically significant difference between the N0 and N1 groups, the N2 and N0–N1 groups were significantly different; consequently, the results of lobectomy and mediastinal lymph node dissection in early-stage SCLC has outcomes in terms of overall survival and 5-year survival similar to those in non-small-cell lung cancer surgery. Lung lobectomy and mediastinal lymph node dissection should be performed in early-stage SCLC patients, as suggested in the current cancer guidelines, and SCLC should be kept in mind when encountering a solitary pulmonary nodule on radiologic examination. Another result of our study is that false-negativity can be detected in mediastinal lymph nodes on PET/CT in clinical early-stage SCLC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.