
Abstract
Air leaks following thoracic surgery continue to be a significant cause of morbidity and mortality. In contemporary thoracic surgery, many aspects of post-surgical air leaks are still controversial. In developing countries like Colombia, state-of-the-art technology such as newer digital drainage systems are not always available, and surgeons rely primarily on water seal systems for air leak management. Although efforts are being made to increase the use of newer digital systems, being a third-world country has its challenges, and we emphasize the importance of following international guidelines as much as possible, especially when facing complex situations such as perioperative air leaks with limited resources.
Introduction
In developing countries like Colombia, special challenges exist. With a scarcity of state-of-the-art technology, thoracic surgeons must not only adapt to the resources available, but also balance treatment using limited contemporary technology. 1 Consequently, whether elective or emergency cases, postoperative air leaks result in prolonged hospital stay, complications, and increased hospital costs.2,3 Although treatment options have improved the way air leaks are managed, early detection and intervention still remain a clinical challenge. Nowadays, most North American and European hospitals have replaced traditional water seal systems with newer digital chest drainage systems that represent a new era in air leak monitoring and allow superior detection and treatment of air leaks. Although water seal system use is declining, many developing countries including Colombia still depend on these “primitive” systems, with few institutions having digital systems available.4–8 When surgeons approach perioperative air leaks using water seal systems, knowledge of fluid kinetics and pressure dynamics is crucial in understanding water seal manifestations of air leaks, demanding more from thoracic surgeons. It is therefore fundamental to understand the role water seal drainage characteristics play in defining immediate and directed intervention for air leaks. Despite many advances in general thoracic surgery, the first digital drainage systems were brought to Colombia in 2009 (Thopaz, Medela AG, Baar, Switzerland) and to date, most hospitals still use water seal systems only; electronic devices are used exclusively in selected cases. The more common chest drainage systems used in Colombia are the Thorametrix (Chest Drainage Systems), and the Ocean and Oasis water seal systems (Atrium Medical). In Colombia, armed conflict continues to be a significant cause of trauma, as well as an important socioeconomic and health problem. 1 The history of cardiothoracic trauma goes back centuries, and the first reported surgical intervention for a penetrating cardiac injury was in 1914. 1 Since then, the way thoracic trauma is approached in Colombia has advanced significantly, including post-traumatic air-leak management. Compared to other Latin American countries, Colombia continues to have one of the highest penetrating thoracic injury rates, as well as incidences of gun-shot wounds. 9 Consequently, thoracic surgeons need to maintain a working knowledge of fluid and air leak physiology, especially in scenarios involving trauma. Although management of air leaks resulting from trauma does not differ significantly from that of an air leak after elective pulmonary resection, the context of trauma results in a more critical and complex patient.
Air leak definitions and water seal characteristics
Because air leaks are managed differently depending on their individual classification, it is imperative to distinguish each type of leak in order to understand the distinct treatment indications and provide an algorithmic approach. Depending on the degree of air leakage, treatment options range from conservative through bronchoscopic to surgical. Anatomically, air leaks result from either bronchopleural fistulas (BPF) or alveolar-pleural fistulas, generating two completely different pathologies, and therefore treatment approaches.9–13 BPF are pathologic communications between the main stem, lobar, segmental, or sometimes sub-segmental bronchi and the pleural space; whereas alveolar-pleural fistulas are communications between the pulmonary parenchyme distal to the sub-segmental bronchi and the pleural space.
Air leak anatomy is indicated by the respiratory cycle in which air leaks appear. Expiratory and forced expiratory air leaks are generally alveolar-pleural in origin. These fistulas are mostly secondary to small sublobar resections and trauma; they usually do not require surgery and resolve spontaneously on water seal and suction. Inspiratory and continuous leaks are either bronchopleural or large and deep parenchymal in origin; these are secondary to larger lung resections such as pneumonectomies and lobectomies. Other causes of BPF are tuberculosis (TB), pneumonia, and trauma. These fistulas may not resolve on water seal alone, thus bronchoscopic and surgical interventions are required.10–17 In the context of trauma, alveolar-pleural fistulas are referred to as minor leaks and correspond to grade II-III lung injuries. These generally result from tractotomies, pneumorrhaphies, sublobar resections, or the trauma itself. BPF are referred to as major leaks, corresponding to grade IV lung injuries; these include deep parenchymal tissue and central airway trauma as well.17–22 Tracheal (central airway) injuries are generally approached similarly to BPF, with some minor leaks requiring temporary bronchoscopic stent placement (Table 1).
Anatomy of air leaks.
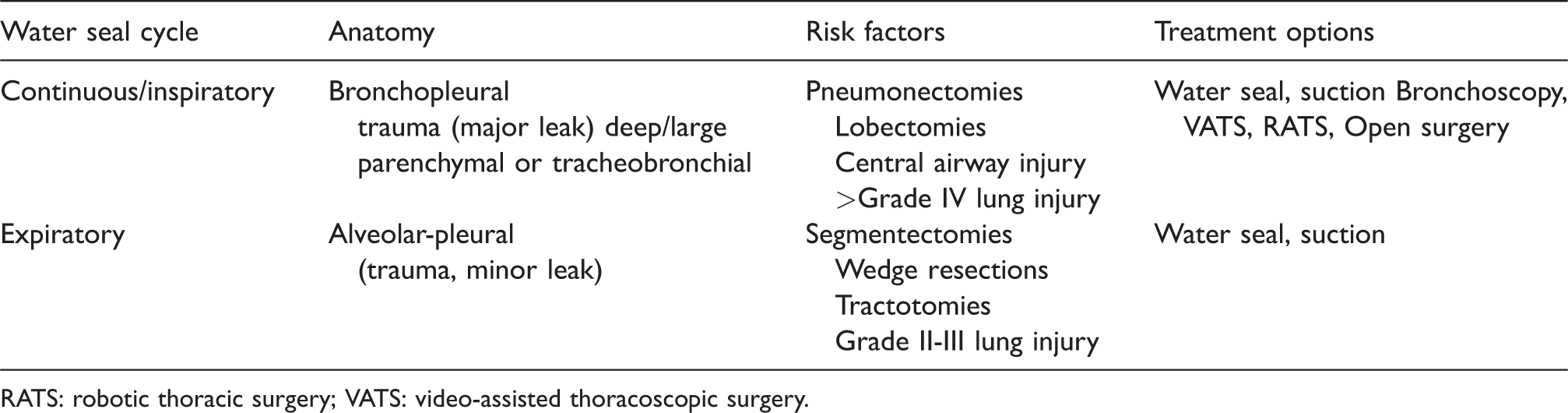
RATS: robotic thoracic surgery; VATS: video-assisted thoracoscopic surgery.
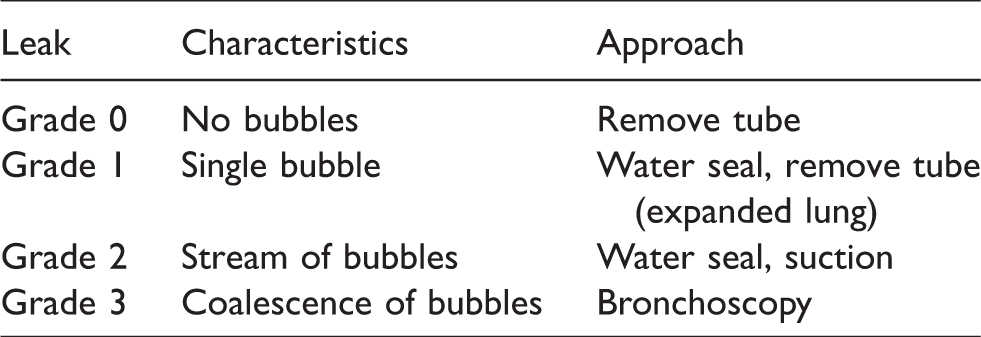
Another critical water seal characteristic is air leak severity. Leak severity can be determined by the number of bubbles escaping the water seal chamber. Traditional water seal-based systems have labeled columns allowing the clinician to visually observe the amount and size of bubbles escaping the chamber with every breath. Grade 0 indicates no leak, grade 1 corresponds to a single bubble escaping the water seal, grade 2 corresponds to a stream of bubbles, and grade 3 corresponds to a group or coalescence of bubbles.10–17 This helps to determine which patients may remain on water seal or merit bronchoscopic evaluation (Table 2). Other physiological factors that may influence bubble escape, such as end-expiratory pressure, lung expansion, and the patient’s respiratory strength should be taken into consideration. Although the clinical impact of this classification may be minimal, it provides clinicians with a general idea of the pleural fistula defect and status.13–17
Severity of air leaks.
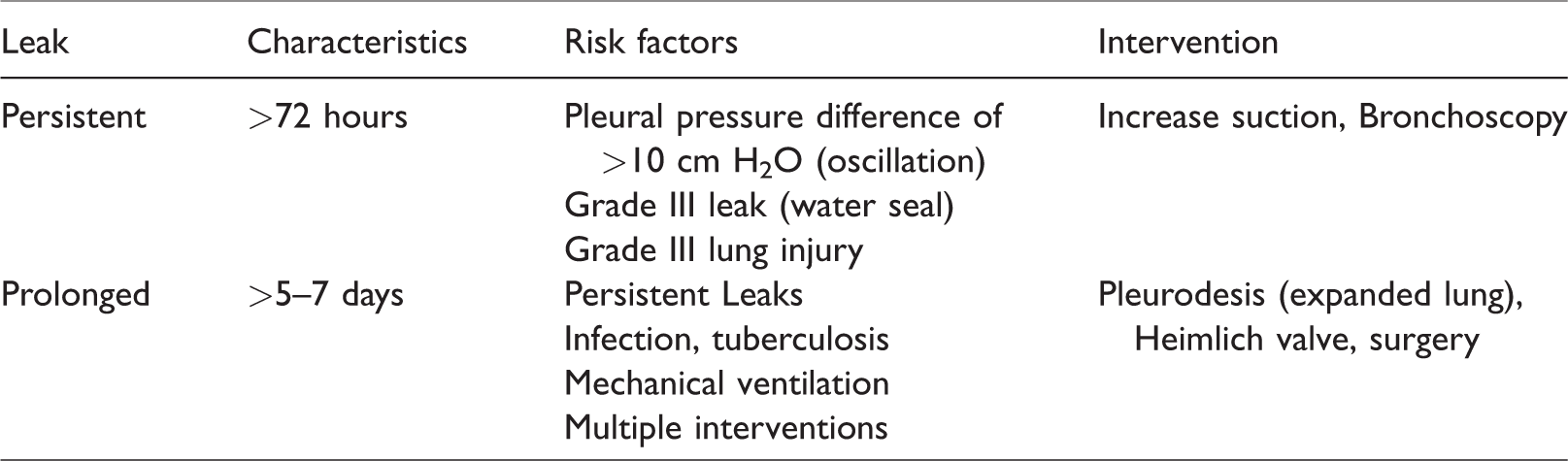
Although some authors use the terms persistent and prolonged leaks interchangeably, in general, air leaks that do not resolve at 72 h are known as persistent air leaks. Predicting persistent air leaks is a matter of observation. During the first 24 h following surgery, a grade III leak on water seal or an intrapleural pressure difference >10 cm H2O seen on water seal oscillation, predict a developing persistent air leak. When air leaks progress beyond 5–7 days, they are defined as prolonged (Table 3).12–16
Duration of air leaks.
Approach to air leaks in Colombia
Water seal and suction
Most alveolar-pleural leaks will resolve spontaneously on water seal because of the siphon effect and air release system. The patient’s own breathing mechanics also release residual pleural air.22–26 The use of suction in pleural fistulas remains controversial and to date, a global consensus does not exist. In Colombia, the use of suction is reserved for the first 12 h following decortication, pleurectomy, trauma, persistent air leaks, and an unexpanded lung after resection. The minimum amount of suction necessary to maintain pleural apposition should be used and lowered progressively, creating a transition period when weaning patients off suction to water seal before removing chest tubes.22–26 When the lungs are collapsed, suction may be applied for up to 5–7 days. If air leaks persist after 5–7 days, patients undergo pleurodesis (expanded lung), or are discharged on a Heimlich valve (stable nonexpanding leak), or require surgery (unstable, expanding leak). Figure 1 describes the general approach to air leaks by Colombian thoracic surgeons using water seal.
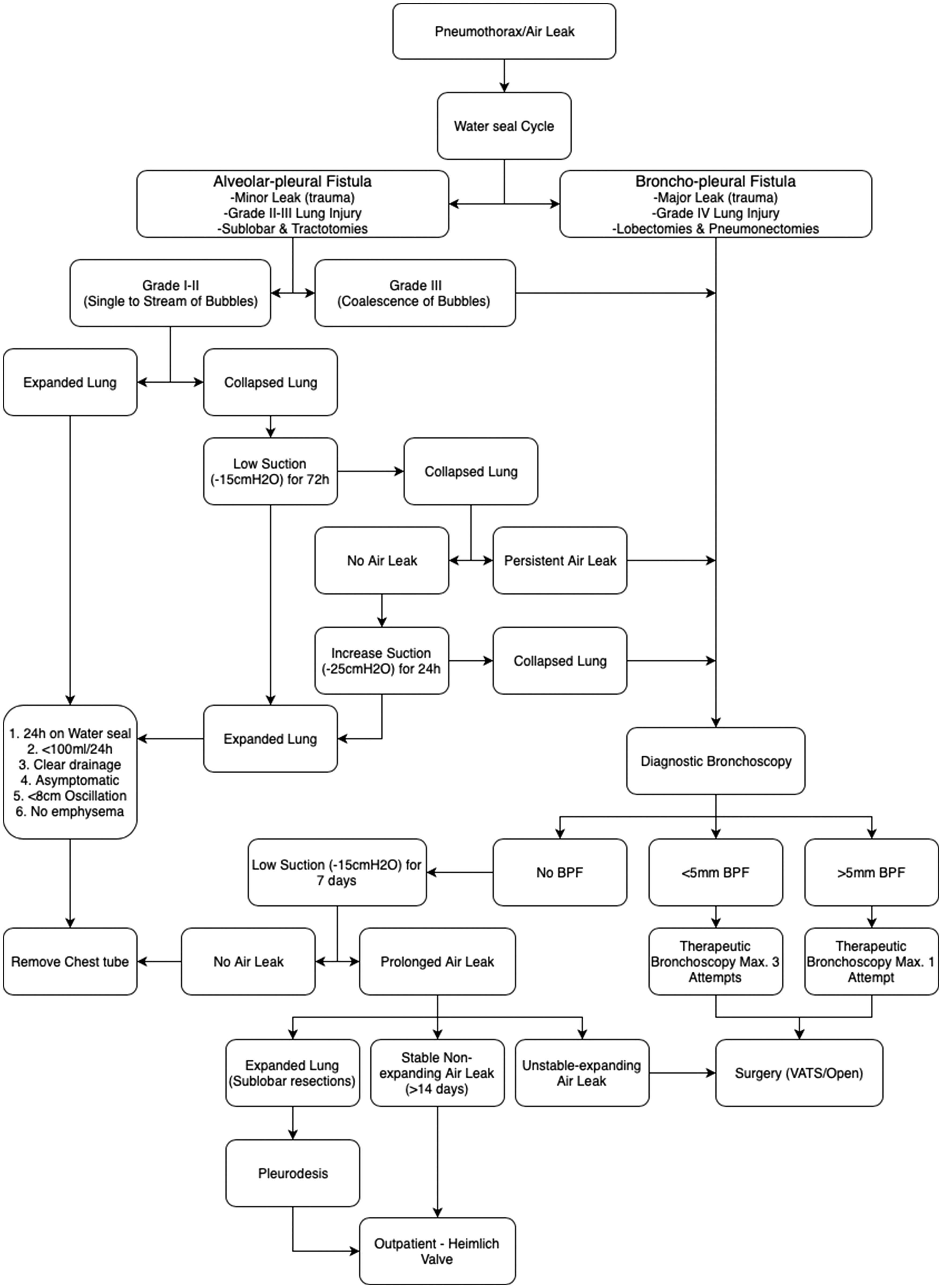
General approach to air leaks using water seal by Colombian thoracic surgeons.
Bronchoscopy
Throughout history, TB has been endemic in Colombia, and special attention to perioperative thoracic patients is crucial because concomitant TB infection is detrimental. Advances in pneumology have not only improved TB treatment but also broadened the pathologies treatable with bronchoscopy, including air leaks initially considered to be surgical. Therapeutic bronchoscopic techniques for air leak management include: submucosal sclerosing injections, fibrin gels, coils, unidirectional valves, BioGlue with albumin, bronchial blockers, and stents. With a high incidence of TB, pneumologists in Colombia have adapted to many difficult scenarios of perioperative management, especially in patients with respiratory infections which pose a great threat to patients with air leaks. In Colombia, water seal characteristics suggesting a bronchopleural leak, indicate the need for diagnostic bronchoscopy. Therapeutic bronchoscopy is generally attempted once in BPF >5 mm and up to three times in those <5 mm before surgical intervention is considered. If no bronchopleural leak is found on bronchoscopy, the air leak is treated as an alveolar-pleural leak. For alveolar-pleural fistulas, a grade III leak is considered a relative indication for bronchoscopic evaluation (Figure 1).
Pleurodesis
In Colombia, pleurodesis is performed mostly using talc and povidone-iodine. Before talc, tetracycline was the main chemical used for pleurodesis. In 1994, the first form of non-medical talc was brought to Colombia, however, it was not widely available. In 2002, povidone-iodine began replacing tetracycline as the main chemical used for benign conditions. The first medical form of talc was introduced to the country in the late 2000s, but due to national health regulations, it fell into disuse, and it was not until 2018 that the Colombian health ministry approved the first medical form of talc. Although different forms of talc have been available in Colombia through the years, its scarcity has resulted in it being used primarily for malignancy, and iodine and tetracycline for benign conditions. Mechanical pleurodesis is also used in specific cases, depending on concomitant pleural conditions. Other agents used in Colombia to a minor degree include bleomycin and silver nitrate. Agents such as interferon, corynebacterium parvum, and autologous blood have not been used in Colombia. Pleurodesis is generally reserved for prolonged air leaks with an expanded lung.
Surgery
Surgery is considered to be the treatment of last resort because mortality increases significantly when patients fail bronchoscopic approaches. The most minimally invasive approach should be performed first, in accordance to the surgeon’s expertise, thus video-assisted thoracoscopic surgery (VATS) should be attempted whenever possible. Since 2005, VATS has grown significantly in Colombia and today, most thoracic surgeons are well-trained in VATS and the use of thoracoscopic mechanical sutures. In 2012, robotic thoracic surgery was introduced, however, its growth has been slow. 1 Patients generally undergo surgery when bronchoscopic treatment fails, or when there is a prolonged air leak with a collapsed lung.
Tube removal
In general, asymptomatic patients with clear drainage <100 mL/24 h (some surgeons allow <100 mL/8 h), an expanded lung, and resolved air leak are considered candidates for tube removal, providing sufficient time has been allowed for pleural symphysis (usually 24 h).27,28 Tube oscillation, another important characteristic, represents intrapleural pressure differences. Oscillations of up to 4 cm are acceptable and indicate pleural apposition, whereas oscillations larger than 8 cm may indicate that the pleural sheets are still not approximated even in the absence of an air leak. Pneumonectomies and upper lobectomies leave residual space and thus >8 cm oscillations are expected and acceptable in these cases. In smaller sublobar resections where pleural apposition should be achieved, oscillations greater than 8–10 cm H2O may predict persistent air leaks, and tubes should be left in place. If chest tubes are removed prematurely, Laplace’s law kicks in (collapsing pressure = 2 × surface tension/alveolar radius) and the lung may collapse.13–18,28,30 Asymptomatic patients with stable prolonged air leaks unresolved within 14 days, without subcutaneous emphysema, and low drainage (<100 mL/24 h), are considered candidates for discharge on a Heimlich valve (Figure 1).
Discussion
Many aspects of post-resection chest tube management remain controversial among surgeons. Here, we will review some recommendations in the current practice of thoracic surgery. One area of controversy is drainage volume allowed for chest tube removal, however, a general consensus allows up to 300 mL/24 h of clear drainage in asymptomatic patients. Another subject is the use of multiple chest tubes. Although a second tube has been an accepted practice following lobectomies, it results in prolonged hospital stay and increased pain with no significant clinical benefits.30–37 Stripping chest tubes is also a practice that in recent studies has shown no benefit for patients and does not improve outcomes. In a comparative study by Allama and colleagues, 32 different forms of BioGlue used after thoracic resections resulted in a decreased duration and number of postoperative alveolar leaks. In a prospective study by Rivo and colleagues, 33 patients presenting with small BPF following thoracic resections underwent repeated flexible bronchoscopic injections of sclerosing agents with an 87.5% resolution of air leaks. Laperuta and colleagues 34 reported the case of a patient with a BPF treated successfully with vacuum-assisted closure and open thoracostomy. Advances in interventional pneumology have also improved the prognosis of pleural fistulas. In recent studies, bronchoscopic unidirectional valve placement and hydrogels with fibrin or platelets show an 85% resolution of leaks at 48 h and 96% complete resolution of air leaks.27,31,35
Since the introduction of digital drainage systems, various studies have determined whether electronic devices are superior to water seal devices in detecting air leaks and thus improving patient outcomes. In a randomized multicenter trial by Pompili and colleagues, 5 patients managed with digital devices had shorter air leak durations and hospital stays. On the other hand, a randomized trial by Lijkendijk and colleagues 6 reported no significant differences in air leak duration or length of hospital stay when a standardized and strict algorithm for chest tube removal was followed. In a meta-analysis by Wang and colleagues, 4 digital drainage systems showed a reduced risk of prolonged air leak, shorter chest tube duration, and hospital stay in patients undergoing lung resections. In a study conducted by Yeung and colleagues, 36 a statistical model was validated through data collected from digital drainage devices, which provided a forecasting system to determine which patients may have their chest tubes safely removed. Although newer electronic systems are continually giving thoracic surgeons more and more information about pleural physiology, these state-of-the-art systems are not available in all centers, thus strict algorithmic protocols should be followed.
Suction should be used discreetly depending on each patient’s needs; some authors support continuous suction, others alternating nocturnal suction, while others support low suction with a progressive increase or decrease. Care should be taken not to apply too much suction impairing gas exchange and in turn increasing the air leak through the fistula.10–14 One clear advantage with digital drainage systems is their ability to regulate suction, adapting to the specific needs of the pleural cavity and avoiding too much or too little suction. The postoperative management of chest tubes and their optimal removal time is still a matter of continuing research. 37 The best moment for chest removal is still debated, however, studies have shown that there is no difference in pneumothorax recurrences when tubes are removed during inspiration or expiration.26,29,30,37 More importantly, coordination with the patient along with the Valsalva maneuver is the best approach to removing chest tubes. Newer tools that help predict chest tube removal success include pleural gas analysis to detect pleural CO2 levels, and pleural fluid protein levels. These two pleural fluid and gas characteristics may play an important role in the future of chest tube removal.38,39 Until all of these newer approaches become universally accepted, a working knowledge of pleural physiology is required not only by thoracic surgeons but also by nurses and residents to provide the best care for patients.
Special attention is merited to the anatomical type of air leaks, whether alveolar or bronchial. Because these two very distinct types of air leaks are managed differently and have their individual prognostic significance; careful attention to water seal characteristics help to differentiate the unique therapeutic needs of each of these pathologies. Water seal drainage systems are not only treatment tools but also offer a diagnostic and prognostic value significant to the thoracic surgeon. Proper knowledge of pleural physiology, air pressures, and fluid kinetics, as well as water seal manifestations, provides clinicians and health care providers with a valuable instrument.
In Colombia, there is a current scarcity of literature regarding postoperative air leak management, and despite the lack of data on Latin American approaches to postoperative persistent air leaks, this review is intended to highlight the importance of following an algorithmic approach to pleural fistulas and postoperative air leak management using water seal in a developing country. As the acquisition of newer digital systems has been slow, large randomized and multicenter studies are lacking in Colombia and South America. At present, evidence-based trials and retrospective studies on postoperative air leaks are being conducted to improve our standard of care.
The treatment of air leaks remains a challenge even for the most experienced surgeon. Although many countries follow their own protocols for the management of air leaks, as well as international guidelines established by pioneers, many surgeons follow an adjusted approach based on experience and institutional resources. To the veteran thoracic surgeon, the management of air leaks may not seem that complex. However, an algorithmic approach plays an important role in creating a mental framework for how to face different surgical scenarios such as air leaks. In Colombia, we have combined both international recommendations and local experience with air leaks, considering our circumstances of endemic trauma and TB. Currently, the country has only one general thoracic surgery residency program, and it is therefore critical to teach the best postoperative air leak management approaches to young surgeons.
Although efforts are being made to increase the use of newer digital systems in Colombia, being a developing country has its challenges that are well recognized. Despite these hurdles, we keep on improving patient care with the resources available, following North American and European standards whenever possible.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.