
Abstract
We describe the case of a 65-year-old man with cryoglobulinemia undergoing cardiac surgery for combined mitral and aortic endocarditis, his preoperative management, and postoperative complications including purpura fulminans as the result of a cryoglobulinemia crisis, ending in death.
Keywords
Introduction
The use of cardiopulmonary bypass (CPB) with cold-blood cardioplegia is standard practice for patients undergoing cardiac surgery. However, a small subset of patients lack the ability to tolerate hypothermia during CPB, including those with cryoglobulinemia, because it may precipitate disease manifestations. Unfortunately, there are very few cases in the literature describing adequate management of these patients in the perioperative period.
Case report
A 65-year-old man presented to the emergency room with a one-month history of relapsing fever, dyspnea, and rash (Figure 1A). Previous evaluation and biopsy had revealed leukocytic vasculitis. A bone marrow biopsy showed monoclonal gammopathy of undetermined significance. He had remote hepatitis C (HCV) infection although he had completed therapy with an undetectable viral load and HCV-RNA. Blood cultures revealed Streptococcus viridans, and transesophageal echocardiography showed a perforated aortic valve cusp and mitral valve vegetation with associated regurgitation. Preoperatively, his cryocrit was 53% and he underwent two rounds of plasma exchange and apheresis. Concomitant aortic and mitral valve replacement was performed without complication using a 23-mm Perimount Magna Ease and a 27-mm Medtronic Mosaic valve, respectively, under normothermic CPB and warm blood cardioplegia. Intraoperatively, the aortic crossclamp time was 163 min and the CPB time was 194 min. The native aortic and mitral valves were sent for culture. While recovering in the intensive care unit, extubated, and off vasoactive support on postoperative day 4, the patient had a persistent high spiking fever (40.3°C) that was addressed with antipyretics. His postoperative treatment for cryoglobulinemia was managed by our institution’s rheumatology team who elected for steroid treatment. The fever persisted and regional ice packs were applied by nursing staff, which resulted in a dramatic change in hemodynamics, manifesting as hypotension requiring high-dose vasoactive support. Bedside echocardiography showed biventricular failure precipitating cardiogenic shock requiring venoarterial extracorporeal membrane oxygenation. Concurrently, rapidly worsening total body purpura fulminans (Figure 1B, 1C) was noted. This was associated with areas where ice packs had been placed. Despite management, biventricular failure persisted and the skin lesions worsened, necessitating right upper extremity and bilateral lower extremity amputations. Rheumatology deemed the patient too unstable to undergo apheresis and decided to continue steroid suppression. His wife elected to withdrawal care. At autopsy, subendocardial acute ischemia, severely congested lungs with hemorrhage, intracranial infarction and subdural hemorrhage, splenic infarction, and significant skin necrosis were observed.
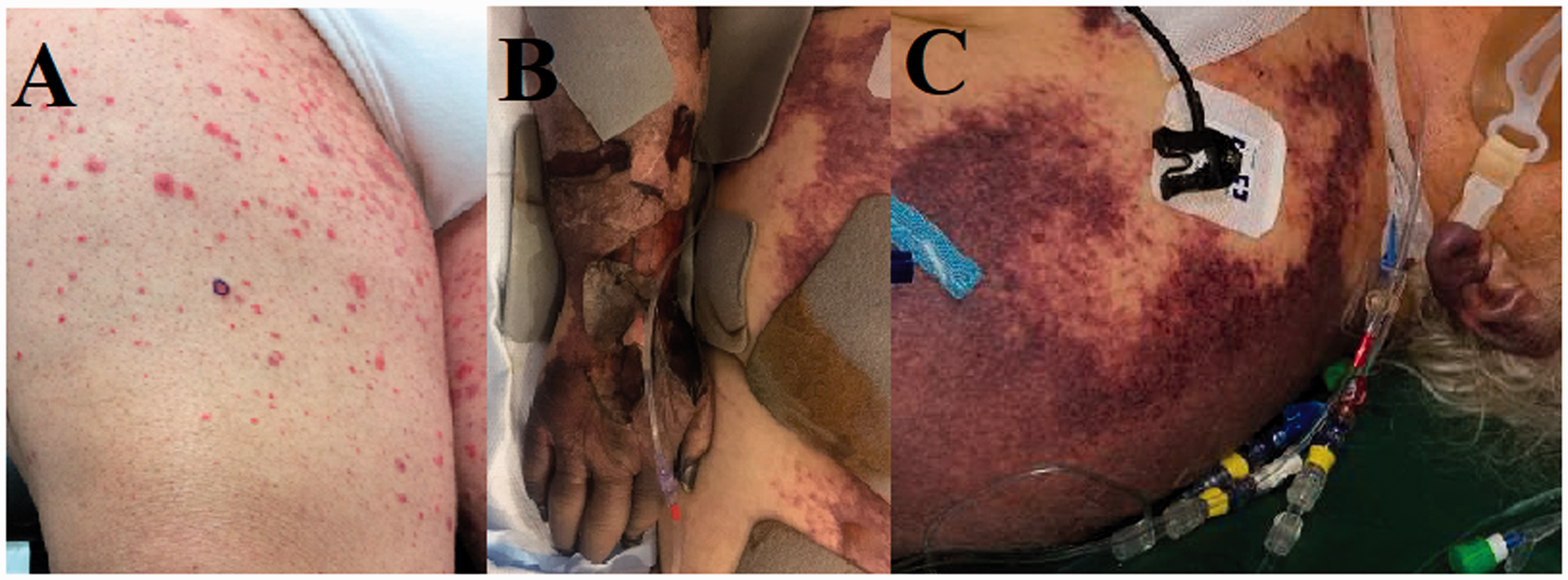
The patient’s skin lesions. (A) The rash upon diagnosis of Streptococcus viridans endocarditis. (B, C) Acute worsening of the rash and necrosis in areas of ice pack application.
Discussion
Cryoglobulinemia was defined in 1933 as phase-change reversible cryoglobulins (CG) in plasma that precipitate at temperatures below 37°C. Diagnosis can be difficult given the fact that healthy adults may have detectable levels of CG. 1 Pathologic CG levels leading to disease are categorized into three types based on the type of immunoglobulins present. Our patient had polyclonal immunoglobulins with a monoclonal immunoglobulin and associated active rheumatoid factor, or type II mixed essential cryoglobulinemia. 1 HCV is associated with type II cryoglobulinemia in 95% of patients, and 80% of these patients have detectable anti-HCV antibodies.2,3 Approximately 15% of patients with any cryoglobulinemia exhibit cutaneous manifestations at normothermia, i.e. macules and papules (as did our patient, Figure 1A), but this increases to 80% in type II disease given the immune complex deposition into the subcutaneous vasculature, causing thrombosis, purpura, and necrosis. 4 Clinical features of cryoglobulinemia reflect three mechanisms of tissue damage: increased blood viscosity, deposition of CG into small arteries and capillaries, resulting in ischemia, infarction, or necrosis; as well as activation of systemic vascular inflammatory mediators. Diagnosis relies on determination of the cryocrit. This test controls the precipitation of CG followed by centrifugation to determine the packed volume as a percentage of the total serum volume. Normal cryocrit values range from 2% to 7% before symptoms manifest. Our patient had a cryocrit of 56%, dropping to 23% after treatment with plasma exchange and apheresis preoperatively.
There are rare case reports of cryoglobulinemia complications following cardiac surgery, although these reports are similar to our case in that normothermic CPB and warm blood cardioplegia was administered. 5 However, these reports fail to mention the patient’s cryocrit and preoperative treatment for their cryoglobulinemia. It is important to balance the hypothermic benefits of CPB against the potential risk of CG precipitation. In our case, the patient had a catastrophic feedback loop of high circulating CG with cutaneous manifestations precipitated by inadequate plasma removal and ice pack therapy for refractory fever remittance. This engendered cutaneous necrosis and consumptive coagulopathy, which ultimately resulted in purpura fulminans and death.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.