
Abstract
Background
The benefits of surgical correction of adult tetralogy of Fallot are well known. The current recommendation is for total correction regardless of age. This study analyzed perioperative factors affecting early outcome after corrective surgery in adulthood in the current era.
Methods
This was a retrospective chart review of 40 consecutive patients over 18 years of age who underwent total correction of tetralogy of Fallot from September 2006 to June 2013. Patients with pulmonary atresia and absent pulmonary valve were excluded. The mean age at surgery was 26.60 ± 8.69 years (range 18–49 years).
Results
The mean intensive care unit stay was 3.30 ± 2.29 days (range 0.75–12 days) and hospital stay was 9.97 ± 3.39 days (range 7–22 days). Mortality was 5% (2/40). Multiple parameters indicating immediate postoperative outcomes and their relationships to selected pre-, intra-, and postoperative factors were analyzed. Multivariate analysis showed that postoperative right ventricular dysfunction had a significant influence on mortality (p < 0.001) and hospital stay (p = 0.01). Performing zero-balance ultrafiltration decreased the need for renal replacement therapy (p = 0.034), duration of ventilation (p = 0.009), incidence of low cardiac output (p = 0.006), intensive care unit stay (p = 0.01), and hospital stay (p = 0.009).
Conclusions
Total correction of tetralogy of Fallot is a safe option for presentations as late as adulthood. The protective effect of zero-balance ultrafiltration on postoperative morbidity needs to be reassessed in larger studies.
Keywords
Introduction
Adult patients with uncorrected tetralogy of Fallot (TOF) pose a management challenge because longstanding hypoxia leads to multisystem damage. Also, right ventricular (RV) hypertrophy and fibrosis predispose to arrhythmias and RV dysfunction.1–7 Although the benefits of early repair are well known,8 it is not unusual to find adult patients with uncorrected TOF in India and other countries. The current recommendation is for total correction of TOF regardless of age. This study analyzed perioperative factors affecting early outcomes after corrective surgery for TOF in adulthood in the current era, in the background of advances in the operating room and intensive care unit.
Patients and methods
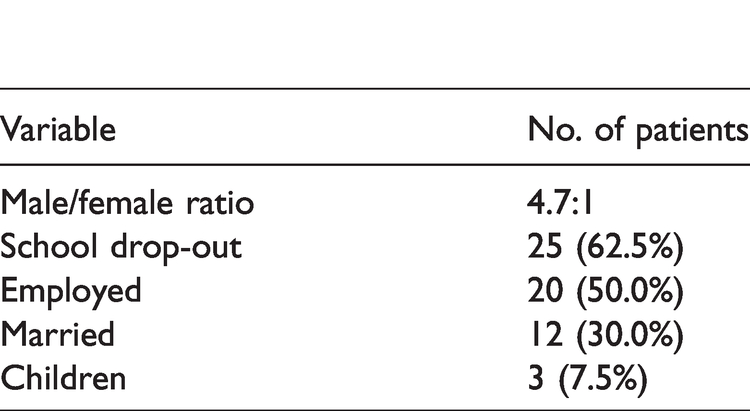
The study was approved by the hospital research and ethics committees. The hospital database was accessed for details of all patients who underwent intracardiac repair of TOF at more than 18 years of age. Patients with pulmonary atresia and ventricular septal defect (VSD) and TOF with absent pulmonary valve syndrome were excluded. A total of 40 patients older than 18 years underwent intracardiac repair of TOF at our center between September 2006 and June 2013. The mean age at diagnosis was 5.37 ± 8.71 years (range 0–39 years) and at surgery it was 26.60 ± 8.69 years (range 18–49 years). Other demographic and socioeconomic data are listed in Table 1.
Socioeconomic data of 40 adult patients with tetralogy of Fallot.
The charts of the patients were reviewed. In addition to demographic and socioeconomic data, the timing of diagnosis, reason for delay in surgery if any, New York Heart Association class, history of complications, history of phlebotomies, and previous surgical procedures were recorded. Details of imaging collected included the pulmonary annulus diameter, diameter of the main pulmonary artery and branch pulmonary arteries (with z scores), predominant level of right ventricular outflow tract (RVOT) obstruction, peak RVOT gradient, type of VSD, presence of additional VSD, aortopulmonary collaterals, coronary artery anomalies, additional defects such as atrial septal defect and left superior vena cava, and ventricular function. A fractional area change less than 35% on 2-dimensional echocardiography and/or a tricuspid annular plane systolic excursion less than 16 mm were considered to be indicators of RV dysfunction. Data regarding pre- and postoperative ventricular function were collected. Preoperative hemoglobin level, packed cell volume, platelet count, and oxygen saturation by pulse oximetry were recorded. The diagnosis was confirmed by echocardiography in all patients. The details of cardiac catheterization studies, when carried out, were collected.
Intraoperative data included surgical findings, additional procedures, cardiopulmonary bypass (CPB) time, aortic crossclamp time, details of cardioplegia, total circulatory arrest time, ultrafiltration techniques, and reexploration. Details of antifibrinolytics and blood and blood products used intra- and postoperatively were also collected. Immediate postoperative outcome data included low cardiac output syndrome, ventricular dysfunction, arrhythmias, the need for renal replacement therapy, duration and type of inotropic support, ventilator support time, the need for reexploration, duration and quantity of chest tube drainage, intensive care unit (ICU) stay, and hospital stay. Inotrope use was quantified using the Wernovsky inotropic score and the vasoactive-inotropic score. Low cardiac output was diagnosed from a combination of factors such as a drop in mixed venous O2 (<75%), widening arterial-mixed venous O2 difference (>20%), increasing lactate level (>2 mmol·L−1), and requirement for inotrope usage for more than 36 h; the presence of 3 or more factors was considered low cardiac output syndrome.
Standard techniques of anesthesia were employed in all patients. Following a median sternotomy, aortic and bicaval cannulation was used to establish CPB. The procedure was carried out under moderate to severe systemic hypothermia. Intermittent antegrade cold blood cardioplegia with St. Thomas’ Hospital cardioplegic solution was used for myocardial protection. The left side of the heart was vented by direct suction through the foramen ovale. The surgical approach was primarily transatrial-transpulmonary. An additional limited ventriculotomy was performed when required, and care was taken to keep the ventriculotomy small to avoid postoperative arrhythmias. The main, right, and left pulmonary arteries were dissected. After aortic crossclamping under total CPB, the right atrium was opened and infundibular resection performed in all cases. The VSD was closed from the right atrium when it was subaortic. When the defect was sub-arterial, it was closed through the RVOT incision. Additional VSD were closed directly when feasible or by using patch material. The pulmonary valve was probed using graded dilators before and after VSD closure. The surgical approach to the RVOT and the pulmonary valve (native valve repair, bioprosthetic valve, or valved conduit) was decided after inspecting the anatomy, and depended on the availability of valved conduits. The emphasis was to ensure pulmonary valve competence at the end of the corrective surgery. Associated procedures were then performed. A small atrial septal defect or patent foramen ovale was left when there was preoperative RV dysfunction. After weaning from CPB, routine direct measurement of RV and left ventricular (LV) systolic pressures was undertaken to rule out significant residual RVOT obstruction. The adequacy of repair was routinely assessed on transesophageal echocardiography. Primary sternal closure was carried out in all cases.
In cases where a previous shunt had been instituted, the surgical technique was modified. With a central shunt, a sternotomy was performed after initiating peripheral CPB with femoral arterial and venous cannulation. Aortic and superior vena caval cannulation was carried out after the sternotomy. A short period of total circulatory arrest was needed when the central shunt was being divided. A Potts shunt was closed by a transpulmonary approach, the shunt insertion was closed from within the pulmonary artery using a pericardial patch. A Waterston’s shunt was divided and transfixed. A Blalock-Taussig shunt was dissected out before administration of heparin, and the shunt was obliterated after CPB was instituted. The shunt was ligated/divided and transfixed/clipped with a hemostatic vascular clip.
Zero-balance ultrafiltration (ZBUF) is a method of filtration in which the filtered fluid is replaced with an equal volume of a balanced salt crystalloid solution to remove inflammatory mediators and vasoactive substances and to reverse hemodilution and decrease tissue edema. ZBUF was performed following the termination of CPB in all cases with a hematocrit closer to 40% at the termination of CPB. The flow through the hemofiltration circuit was set at a rate of 10–15 mL·kg−1·min−1 initially, and increased gradually to a maximum of 20 mL·kg−1·min−1 if tolerated hemodynamically. The volume of filtrate to be removed was calculated using the formula: volume of filtrate = (a−b) × c/b, where a = final hematokrit desired (target 40%–45%), b = final hematokrit on bypass, and c = patient’s estimated blood volume. During ZBUF, the volume was maintained via the main arterial pump. The rate of transfusion must be held below the rate of flow through the circuit. The optimal volume and filling pressures were determined by the surgeon and/or anesthetist/perfusionist.
The treating team and postoperative care protocols remained largely unchanged for the duration of the study period. Patients were transferred from the ICU to the ward when they were extubated and maintained adequate oxygen saturations with hemodynamic stability off inotropic support, and there was no significant pleural effusion. Pre-discharge and follow-up echocardiographic data and clinical status were recorded. Echocardiographic details included RVOT gradient and pulmonary regurgitation that was graded on a scale of 1 to 4 (trivial, mild, moderate, severe) based on the width of the jet relative to the RVOT, continuous-wave Doppler characteristics, and any reversal of color flow in the branch pulmonary arteries. Early outcome measures considered included hospital mortality, duration of ventilation, duration of ICU and hospital stays, low cardiac output syndrome, renal replacement therapy, inotropic score, and postoperative RV and LV dysfunction.
Measured and calculated continuous variables are expressed as mean ± standard deviation. The effect of various preoperative and intraoperative variables on outcomes were analyzed using univariate (Student’s t test and linear regression) and multivariate (analysis of variance and multiple regression) analysis. Statistical analyses were performed using IBM SPSS version 21.0 software (IBM Corp., Armonk, NY, USA). A p value less than 0.05 was considered significant.
Results
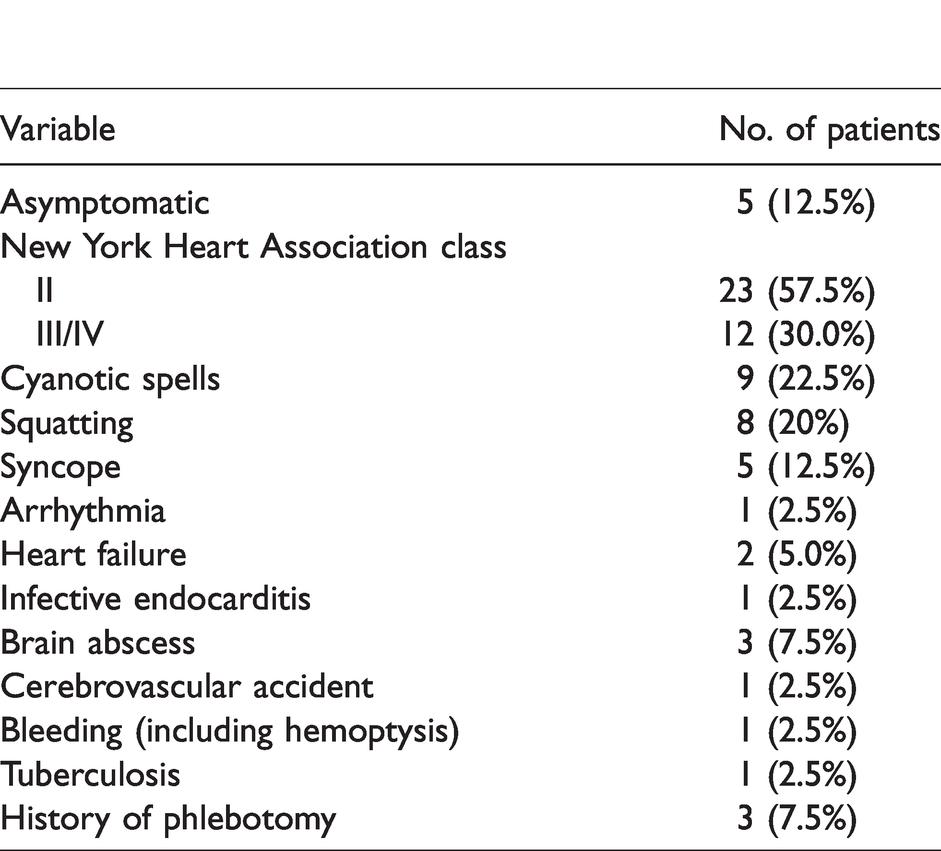
The preoperative clinical data are presented in Table 2. The mean oxygen saturation was 81.6% ± 10.1% (range 57%–97%) and the packed cell volume was 59.8% ± 11.06% (range 33%–78%). Seven (17.5%) patients had undergone previous shunt surgeries: 4 modified Blalock-Taussig shunts, 1 Potts shunt, 1 left classic Blalock-Taussig shunt, and 1 Waterson’s shunt. Financial reasons and/or lack of awareness was cited by 18 (45.0%) patients as the reason for delay in surgery. Preoperative imaging data are summarized in Table 3. Cardiac catheterization studies were performed in 35 (87.5%) patients: 3 (7.5%) had raised RV end-diastolic pressure, and one (2.5%) had raised LV end-diastolic pressure, suggestive of preoperative ventricular dysfunction. Surgical data are listed in Table 4. The techniques used for reconstruction of the RVOT are summarized in Table 5. The mean ICU stay was 3.30 ± 2.29 days (range 0.75–12 days) and hospital stay was 9.97 ± 3.39 days (range 7–22 days). The ICU data are summarized in Table 6. Hospital mortality was 5% (2/40); one patient died within 24 h of surgery due to severe RV dysfunction, and the other died on postoperative day 21 due to low cardiac output leading to multiorgan dysfunction. Both patients had intracardiac correction with a transannular patch only, resulting in free pulmonary regurgitation, and were operated on earlier in the series. Other data from the immediate postoperative period are summarized in Table 6. Surgical reexploration of the mediastinum was considered when bleeding in the first 2 h was >300 mL·h−1 or >200 mL·h−1 for 4 consecutive hours despite adequate replacement of clotting factors. Reexploration was also performed in patients with hemodynamic instability or cardiac tamponade. The average chest tube output on days 0–3 was 741 mL (range 100–3610 mL). Three (7.5%) patients underwent reexploration for clinically significant bleeding.
Clinical data of 40 adult patients with tetralogy of Fallot.
Preoperative imaging data of 40 adult patients with tetralogy of Fallot.
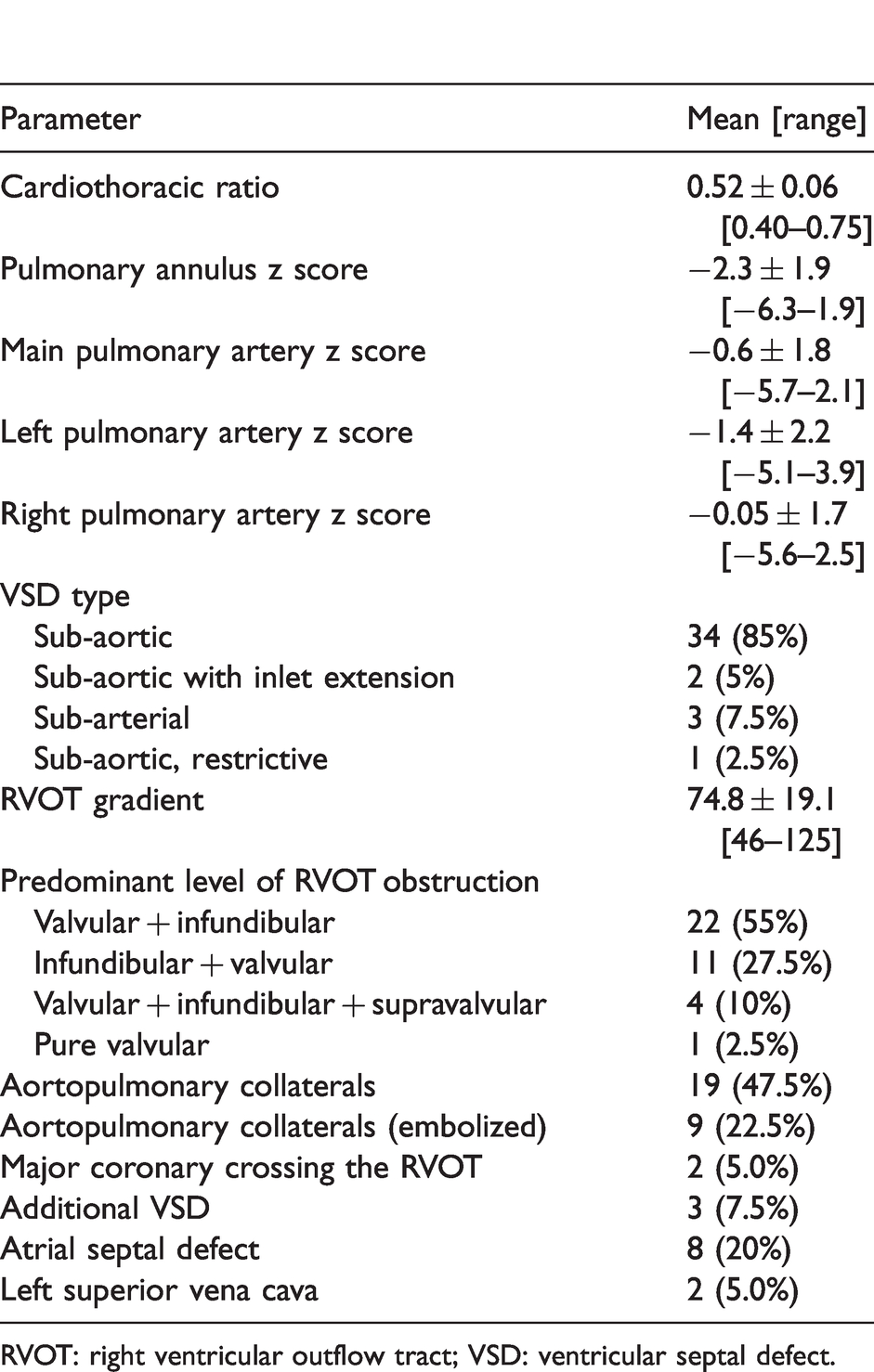
RVOT: right ventricular outflow tract; VSD: ventricular septal defect.
Surgical data of 40 adult patients with tetralogy of Fallot.
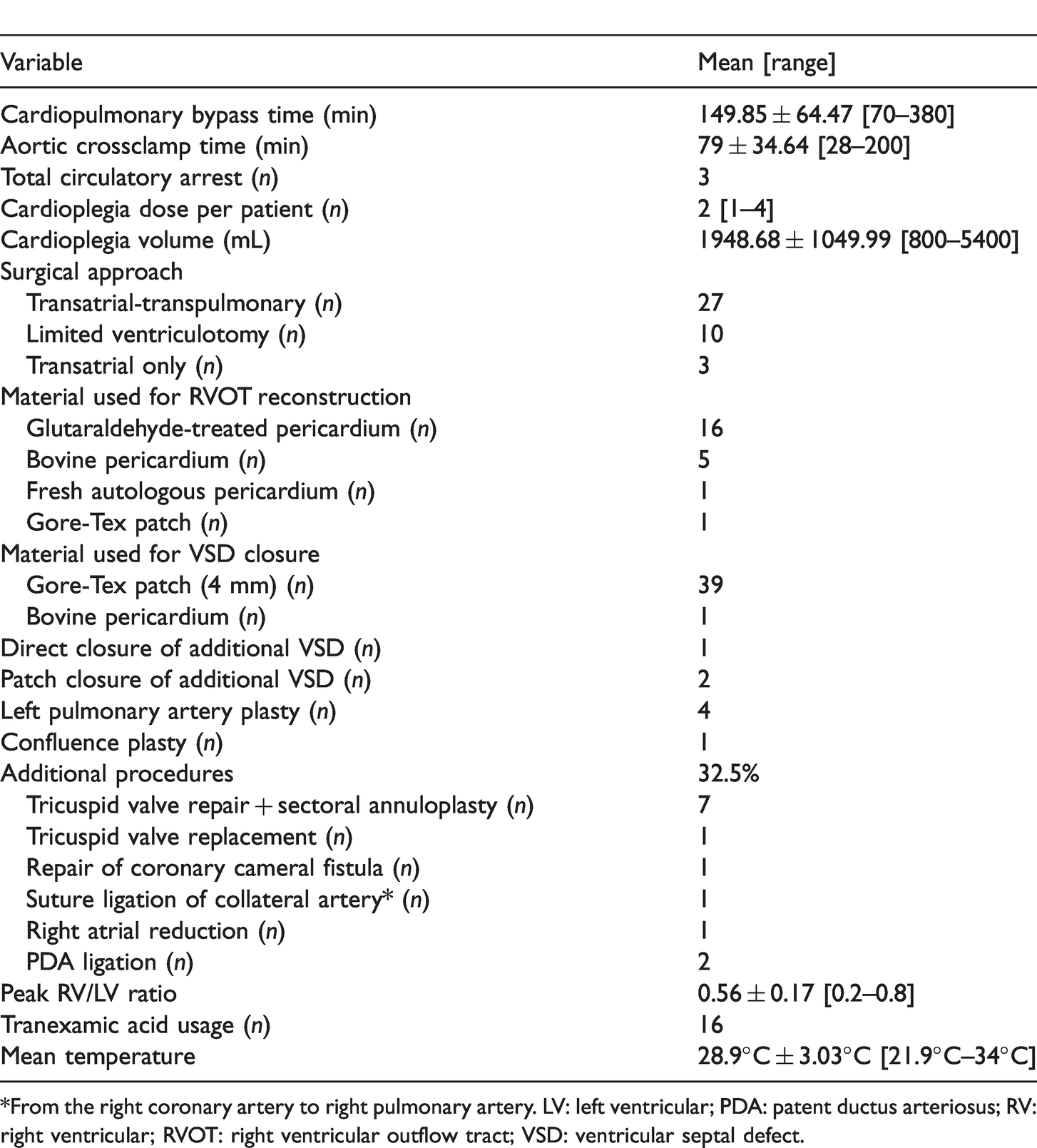
*From the right coronary artery to right pulmonary artery. LV: left ventricular; PDA: patent ductus arteriosus; RV: right ventricular; RVOT: right ventricular outflow tract; VSD: ventricular septal defect.
Techniques of right ventricular outflow tract reconstruction.
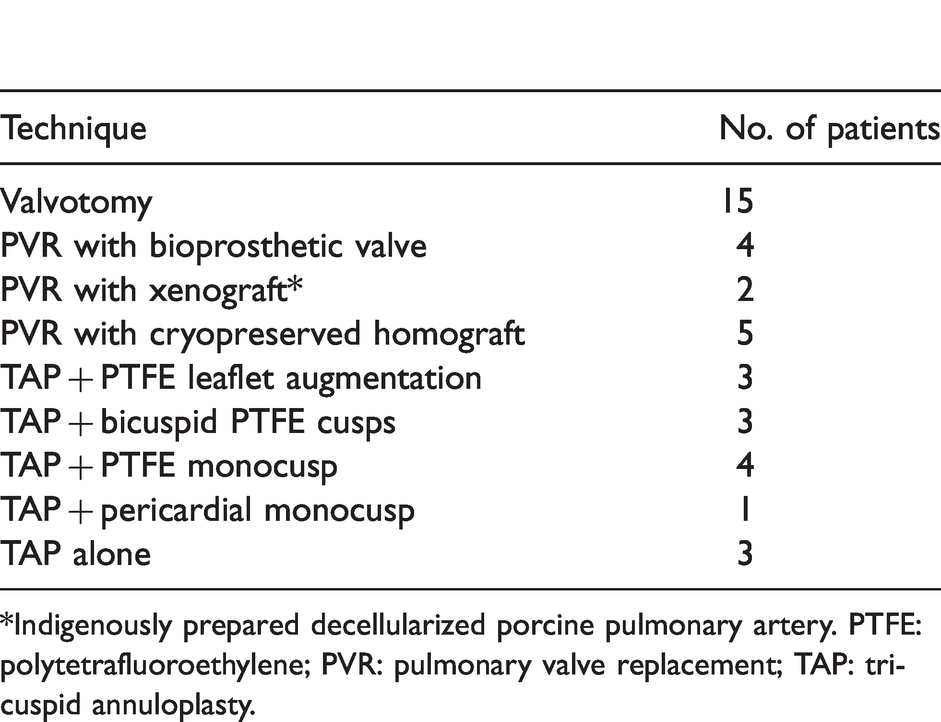
*Indigenously prepared decellularized porcine pulmonary artery. PTFE: polytetrafluoroethylene; PVR: pulmonary valve replacement; TAP: tricuspid annuloplasty.
Immediate postoperative data.
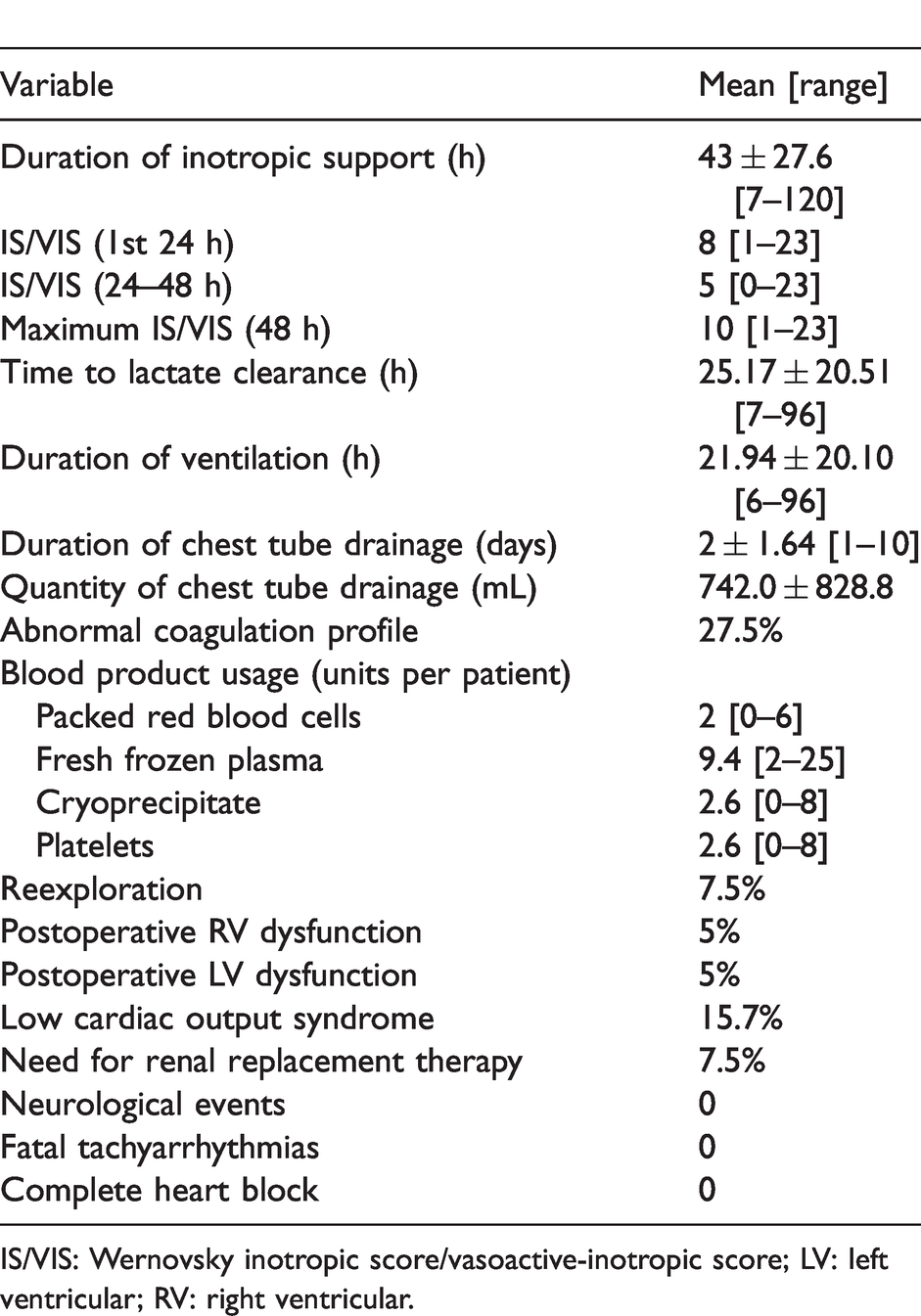
IS/VIS: Wernovsky inotropic score/vasoactive-inotropic score; LV: left ventricular; RV: right ventricular.
On univariate analysis, older age at surgery (R2 = 0.099), higher packed cell volume (R2 = 0.099), smaller pulmonary annulus (R2 = 0.099), main pulmonary artery z score (R2 = 0.109), and higher RVOT gradient (R2 = 0.099) were associated with adverse outcomes. Preoperative RV dysfunction had a significant association with duration of ventilation (p = 0.012) and need for renal replacement therapy (p = 0.041). Previous shunt surgery had a significant association with low cardiac output syndrome (p = 0.006), inotropic score (p = 0.025), and need for renal replacement therapy (p = 0.041). Among the intraoperative factors, longer crossclamp time (R2 = 0.105) and greater number of cardioplegia doses (R2 = 0.099) were associated with adverse outcomes, while ZBUF had a significant protective effect on low cardiac output syndrome (p = 0.027). Preoperative packed cell volume (R2 = 0.099) and postoperative pulmonary regurgitation (R2 = 0.099) were significantly associated with postoperative RV dysfunction. Postoperative RV dysfunction was significantly associated with low cardiac output syndrome (R2 = 0.1404) and high inotropic score (p = 0.03). Postoperative LV dysfunction was significantly associated with low cardiac output syndrome (p = 0.017) and high inotropic score (p < 0.0001). Multivariate analysis showed that the factors affecting outcome included the severity of RVOT obstruction which was significantly associated with higher inotropic scores (p = 0.035). Among the intraoperative factors, ZBUF had a significant positive effect on low cardiac output syndrome (p = 0.006), renal replacement therapy (p = 0.0344), duration of ventilation (p = 0.009), and ICU (p = 0.010) and hospital stay (p = 0.009). Postoperative RV dysfunction was significantly associated with duration of hospital stay (p = 0.014), while postoperative LV dysfunction was associated with higher inotropic scores (0.014) on multivariate analysis. Postoperative RV and LV dysfunction (p = 0.001) had significant associations with hospital mortality. Although on univariate analysis, age at surgery, preoperative hematocrit, low platelet count, altered coagulation profile, deep hypothermia, and low annulus z scores were associated with significant postoperative bleeding, reexploration, and blood product usage, these factors were not found to be statistically significant on multivariate analysis. ZBUF was performed in 23 cases. On univariate analysis, ZBUF had a significant protective effect on low cardiac output syndrome. On multivariate analysis, ZBUF had a significant positive effect on low cardiac output syndrome, duration of ventilation, and ICU and hospital stays. Significant postoperative bleeding was found in 15 patients in whom ZBUF was not performed. However, the effect of ZBUF on postoperative bleeding, reexploration rates, and blood product usage was not statistically significant.
Discussion
Outcomes of various techniques of surgical management of TOF in children have been well described. A different set of challenges must be addressed in the management of uncorrected adult TOF.1–7 A comprehensive analysis of the factors that affect early outcome, especially in the background of advances in the operating room and intensive care unit has not been published. Van Arsdell and colleagues8 recommended between 3 and 11 months as the optimal age for repair; mortality varied from 0 to 2.6% in this series. This is much better compared to adult TOF, highlighting the essential difference in physiology between the two subsets. In the largest published series of 793 patients, Nollert and colleagues2 reported 30-day mortality of 25% in 1997. Khan and colleagues,9 in their recent series of 80 patients, reported mortality of 8%; 11.25% had low cardiac output, and 25% moderate to severe pulmonary regurgitation. The current 5% is a marked improvement.
Postoperative RV and LV dysfunction had significant associations with mortaltity on multivariate analysis, which is self-explanatory. Symptom status (85%), previous shunts (20%), need for tricuspid annuloplasty or conduits for RVOT reconstruction (62.5%), and the fact that only 37.5% of patients were managed with pulmonary valvotomy alone, emphasizes that RVOT obstruction was severe in the majority of patients in this series. It is interesting and important to note that preoperative packed cell volume, which is a surrogate for the degree of hypoxia and thereby the severity of RVOT obstruction, was significantly associated with postoperative RV dysfunction. This reflects the chronic deleterious effects of RV hypertrophy and hypoxia. As expected, postoperative pulmonary regurgitation was significantly associated with postoperative RV dysfunction, which in turn was associated with mortality. This highlights the importance of maintaining a competent valve in the RVOT in the postoperative period. The effects of sudden volume overload in a chronically hypertrophied RV after intracardiac repair with a transannular patch alone, especially in older patients, is well described.10–12 Our policy has been to insist on a competent valve during primary repair to reduce ventricular dysfunction after surgery, either in the form of valve repair (valvotomy and valve-sparing techniques) or pulmonary valve replacement with a bioprosthetic valve or valved conduits such as a homograft or xenograft.13–15 In cases where tricuspid annuloplasty was required, a limited ventriculotomy was performed to reduce the size of the tricuspid annulus. It is important to note that this policy was violated in both the deaths in this series, only to reaffirm the policy. The limited number of patients in each subgroup of RVOT approach precluded subgroup analysis.
The impact of previous shunt surgery on outcomes of intracardiac correction is controversial.4,5,16 Previous shunt surgery was reported to have no effect on outcomes in the studies of Rammohan and colleagues5 and Presbitero and colleagues.4 On univariate analysis, we found a significant relationship between shunt surgery and postoperative inotropic use and low cardiac output in the postoperative period, and the requirement for renal replacement therapy. This could be attributed to the fact that shunt dissection and take-down was performed on CPB in these cases, thereby prolonging CPB time. No significant correlation (p = 0.6) with the need for reexploration for bleeding was noted in patients with previous shunt surgery. In contrast to the report of Nandi and colleagues,16 previous shunt surgery did not result in higher hospital mortality in our experience. While studies have recommended the routine use of epsilon-amino caproic acid, aprotinin, and a cell saver to minimize bleeding in chronically cyanotic patients,1 we did not use either of these drugs or a cell saver. Some patients in this study received tranexamic acid at induction with no significant reduction in either the quantity of drainage or the need for reexploration.
To the best of our knowledge, the benefits of ZBUF in open heart surgery for the chronically cyanosed adult congenital heart disease patient have not been studied. Beneficial effects of conventional ultrafiltration and ZBUF to remove inflammatory mediators in children has been reported.17 A meta-analysis of all randomized controlled trials that looked at the benefit of ZBUF failed to find any benefit in adults. The same study found that ZBUF decreased the duration of mechanical ventilation in pediatric patients after CPB, but failed to find any other benefit.18 In the current study, ZBUF had a significant protective effect against low cardiac output syndrome on univariate analysis. On multivariate analysis, it had a significant positive effect on low cardiac output syndrome, duration of ventilation, and ICU and hospital stays.
The drawbacks of this study include the retrospective nature and relatively small number of patients for subgroup analysis. We concluded that repair of uncorrected tetralogy of Fallot in adulthood is a safe surgical option, with mortality showing a decreasing trend in parallel with improvements in operating room and ICU standards. Pre-, intra-, and postoperative factors influencing outcomes in the current era have been determined in the current study, with postoperative RV and LV dysfunction being major factors associated with mortality. The importance of preventing pulmonary regurgitation in the immediate postoperative period, and thus RV dysfunction and consequent mortality, cannot be overstated. Performing zero-balance ultrafiltration had a significant positive influence on postoperative morbidity. Further research is warranted to assess the positive impact of ZBUF, an easily available technique, on immediate postoperative outcomes.
Supplemental Material
AAN882870 Research Data - Supplemental material for Adult tetralogy repair: factors affecting early outcome in the current era
Supplemental material, AAN882870 Research Data for Adult tetralogy repair: factors affecting early outcome in the current era by Sowmya Ramanan, Navaneetha Sasikumar, Krishna Manohar, Salla Sweta Ramani, RaghavanNair Suresh Kumar , Ravi Agarwal, Raghavan Subramanyam and Kotturathu Mammen Cherian in Asian Cardiovascular and Thoracic Annals
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.