
Abstract
Background
Postoperative delirium is common in patients undergoing coronary artery bypass grafting, characterized by cognitive decline. This study aimed to evaluate the effect of early planned mobilization on delirium after coronary artery bypass grafting.
Methods
This double-blind randomized clinical trial enrolled 92 consecutive patients who underwent coronary artery bypass grafting from September to December 2018. The patients were divided into two groups of 46: a mobilization protocol was applied in the intervention group in the first 2 days after surgery; the control group received routine nursing care only. Demographic data, medical records, and Neecham confusion scores were analyzed.
Results
Patients in the control group used cigarettes (31.1% vs. 11.1%, p = 0.020) and opium poppy for recreation (35.6% vs. 8.9%, p = 0.002) more frequently, had longer intubation times (11.91 ± 3.87 vs. 10.23 ± 2.71 h, p = 0.020), and fewer blood components infused (15.6% vs. 33.3%, p = 0.05). More patients in the intervention group had normal function on the 2nd postoperative day compared to the control group (25 vs. 2, respectively, p = 0.001). The intervention group had significantly higher Neecham scores on postoperative day 2 (22.49 ± 2.03 vs. 26.82 ± 2.10, p = 0.001). Multivariable analysis showed significant associations between Neecham score and age (p = 0.022), ejection fraction (p = 0.015), myocardial infarction (p = 0.016), systolic pressure (p = 0.009), and diastolic pressure (p = 0.008).
Conclusions
Early planned mobilization was effective in reducing postoperative delirium in patients undergoing coronary artery bypass grafting.
Introduction
Coronary artery bypass grafting (CABG) is the most common surgical approach for coronary revascularization. In spite of progress in the surgical procedure, anesthesia management, and postoperative intensive care, CABG patients are still at high risk of postoperative delirium. 1 , 2 Studies have revealed that postoperative delirium has an adverse impact on postoperative outcomes including mortality, nosocomial complications, and cognitive decline. 3 Delirium is a neurological condition typified by acute cognitive dysfunction, variation of mental status, carelessness, and severe disturbance of consciousness. 4 The incidence of postoperative delirium has been reported to vary from 16% to 73% among patients undergoing cardiac surgery. 5 Although the occurrence of postoperative delirium has been well established, the underlying mechanisms are not fully understood. Previous studies reported that systemic inflammation leads to disruption of the blood-brain barrier. Consequently, neurons are predisposed to injury and dysfunction that causes a neuroinflammatory condition. Hence, conditions such as cardiopulmonary bypass that induce systemic inflammation may increase the risk of postoperative delirium. 6 However, the etiology of postoperative delirium seems to be multifactorial and includes older age, concomitant comorbidities such as diabetes, and prolonged mechanical ventilation (>24 h) in the cardiac intensive care unit (ICU). 7 Early mobilization of patients is widely used in different situations in the cardiac ICU, and studies show that early mobilization can improve the recovery of cardiovascular, respiratory, and neurological function.8–10 Most studies on early mobilization have focused on how CABG patients should be mobilized in the physiotherapy management of patients, 11 , 12 and there have been relatively few investigations on the effects of early mobilization on postoperative delirium. This study aimed to assess the effectiveness of early planned mobilization on postoperative delirium in patients undergoing CABG.
Patients and methods
This prospective, randomized, double-blind clinical trial was carried out on consecutive patients scheduled for CABG. The study was completed according to the standards established in the Declaration of Helsinki and was reviewed and approved by the institutional review boards and the hospital ethics committee on June 25, 2018 (IR.IAU.KHUISF.REC.1397.152). Also, it was registered in Iranian Registry of Clinical Trials with registration number ID: IRCT20190611043867N1. The aims of the research were explained to the participants and written informed consent was obtained from all participants before surgery. The sample size was calculated for the primary outcome based on a previous study by Kazmierski and colleagues 12 who reported a 16.3% incidence of postoperative delirium after cardiac surgery. With the significance level set at 0.05, power set at 80%, and a potential attrition rate of 5%, the sample size required to detect differences was 46 for each of the experimental groups. 13
We included patients who agreed to participate in the study, did not undergo emergency CABG, had a Glasgow coma scale score of 15, no hearing, speech, or visual impairment, no neurological and movement disorders, and were conscious. Exclusion criteria comprised any physiologic or hemodynamic instability after surgery (arrhythmia, oxygen saturation < 90%), disturbance of consciousness, and prolonged mechanical ventilation (>6 h).
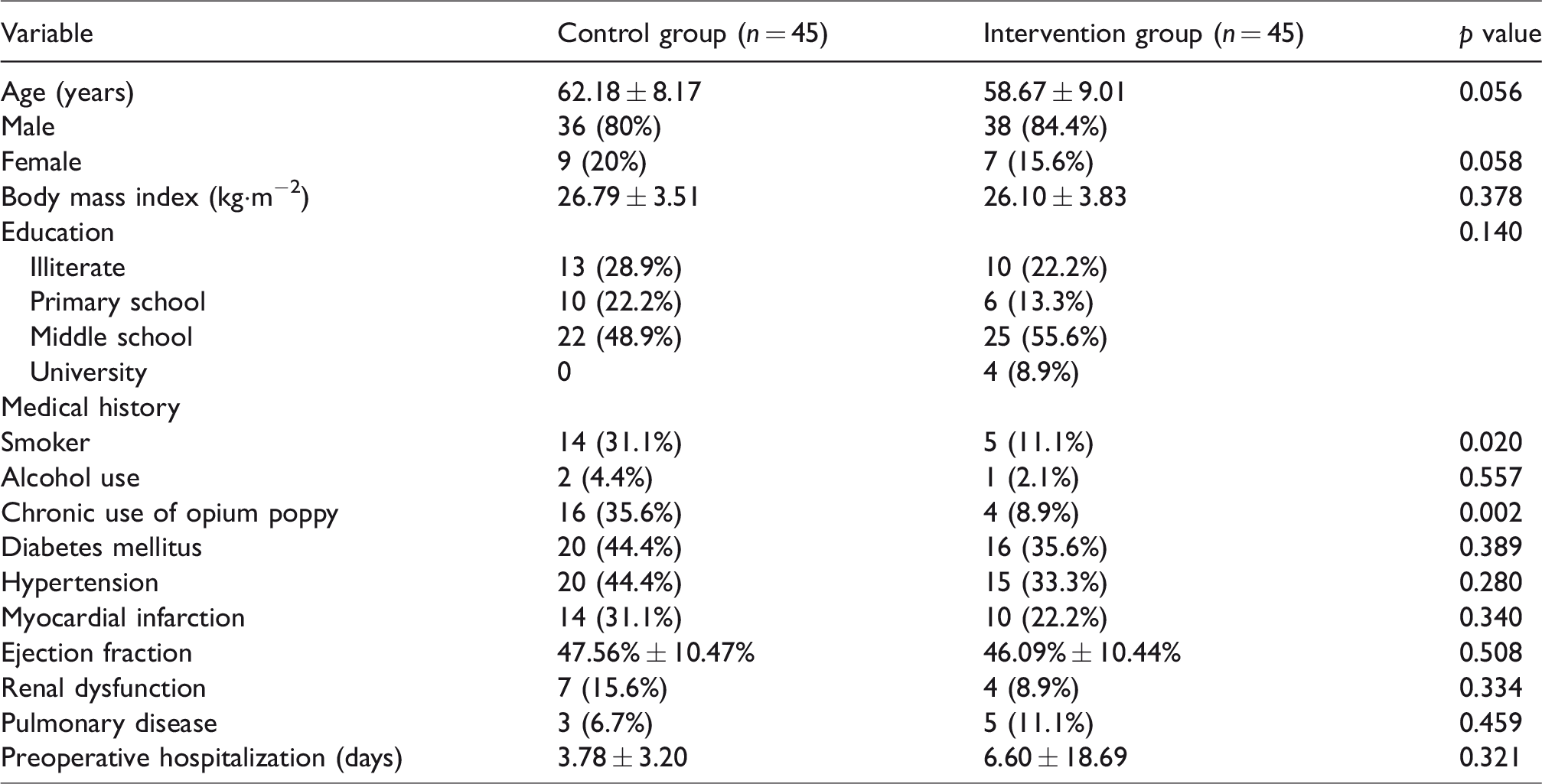
From September to December 2018, 178 eligible participants admitted to the cardiac ICU after CABG were enrolled in our study. Of these, 92 patients met the criteria to enter the study and were assigned at random to a control group of 46 and an intervention group of 46. As depicted in Figure 1, one case in each group was excluded from the final analysis due to lack of data. Our final study population consisted of 74 men (82.2%) and 16 women (17.8%), mean age 60.42 ± 8.72 years. There was no statistically significant difference in terms of demographic characteristics and underlying conditions between the 2 groups. However, preoperative use of cigarettes and opium poppy (≥4 g·day−1) for recreational purposes for at least 1 year were significantly more common in the control group (Table 1).
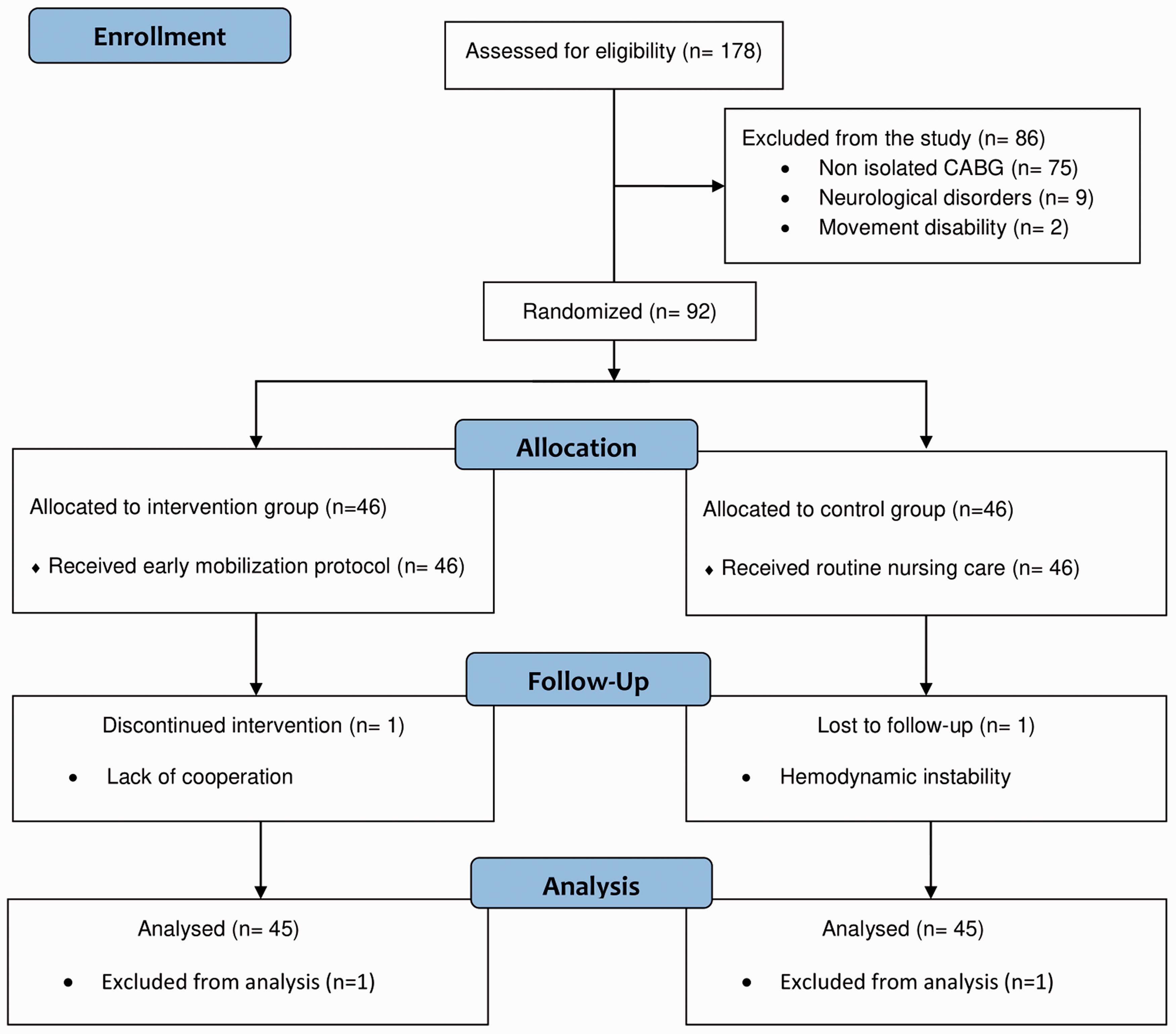
The flow diagram of the study.
Comparison of patient variables between control and intervention groups.
The Neecham confusion scale was used to assess acute confusion on the basis of criteria identified by cardiac ICU nurses. The Neecham confusion scale contains 9 items divided into 3 subscales (responsiveness, behavior, vital functions). Each scaled item gives three descriptions that assess mental and physical status. The scores may range from zero (minimal function) to 30 (normal function). The cut-off point for delirium is 24, and a score less than 24 indicates delirium. 14 Cognitive assessment was performed before and after the intervention on the 1st and 2nd postoperative days.
Two hours after extubation on the 1st postoperative day, patients in the intervention group were placed in a sitting position and their legs were hung off the bed for 15 min. On the morning of the 2nd postoperative day, participants were seated on the bed edge for 5 min and then walked 5 meters in the cardiac ICU with pulse oximetry monitoring. On the evening of the 2nd postoperative day, these steps were repeated and the patients walked 10 meters. During the intervention, each patient was accompanied by a cardiac ICU nurse. In the case of a variation in heart rate and oxygen saturation more than 20% from baseline, the intervention was discontinued. 1 Patients in the control group received the routine hospital cardiac ICU care including adequate fluid resuscitation, appropriate inotropic support, ventilator management, and chest physiotherapy. All patients received intravenous paracetamol to relieve postoperative pain and nitroglycerin to control blood pressure.
The patients were moved to the cardiology ward after discharge from the cardiac ICU. They were visited daily by surgeons and cardiologists. Echocardiography was performed and ventricular function was recorded before discharge from the hospital. Weekly follow-up of the patients was conducted in the outpatient clinic for one month, with follow-up by telephone over the course of 6 months.
All statistical analyses were performed using IBM SPSS version 22.0 (IBM, Inc., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation. The independent Student t test was used to identify significant differences between data. Categorical variables are presented as frequency (percentage) and were analyzed using Fisher’s exact test. The Mann-Whitney U test was utilized to compare nonparametric data between the two groups. To investigate the relationship between Neecham confusion score and patient variables, linear multivariable regression models were created for each parameter. All p values ≤0.05 were considered to indicate statistical significance.
Results
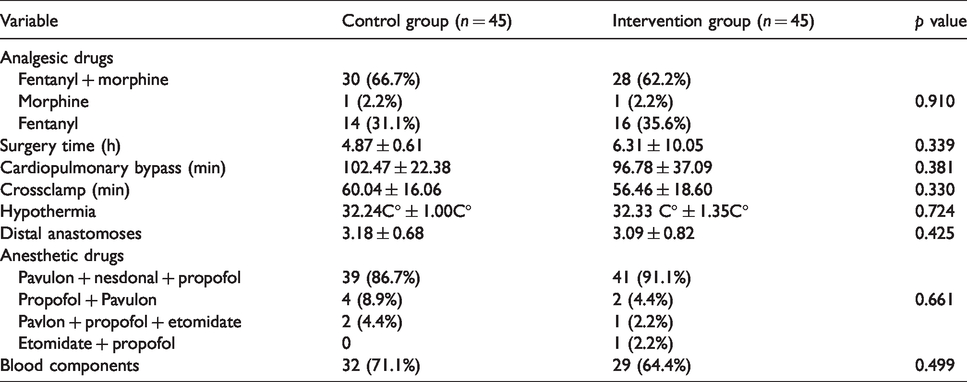
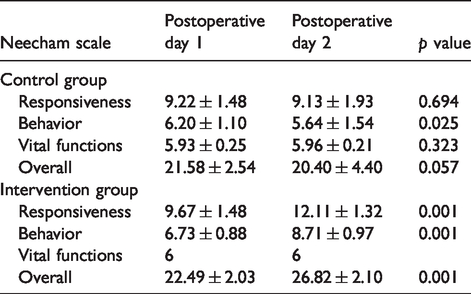
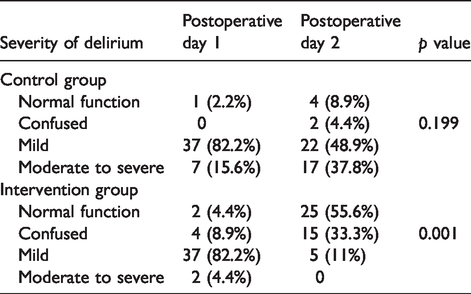
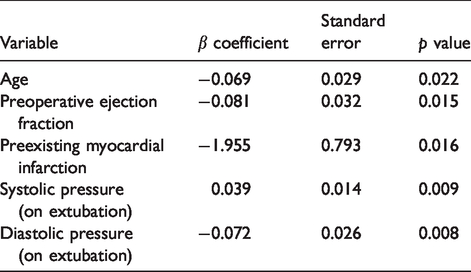
There was no significant difference in intraoperative variables between the two groups (Table 2). However, patients in the control group experienced significant prolonged mechanical ventilation (>6 h) and received fewer blood components in the cardiac ICU (Table 3). There was no record of mortality or severe postoperative complications among the patients in both groups. Table 4 and Table 5 represent study outcomes regarding delirium status. Table 4 gives the Neecham confusion scores in both the control and intervention groups. There was no significant change in the control group on postoperative day 1 and 2, while patients in the intervention group had significantly higher Neecham confusion scores on the 2nd postoperative day. The incidence of mild postoperative delirium in both groups was 82.2% on the 1st postoperative day. Table 5 indicates that 55.6% of patients in the intervention group vs. 8.9% in the control group experienced normal function on the 2nd postoperative day. The number of patients who had moderate to severe postoperative delirium in the control group increased on the 2nd postoperative day (37.8%). The multivariable regression model showed a significant association between Neecham confusion score and age, preoperative ejection fraction, preexisting myocardial infarction, systolic and diastolic pressures on extubation (Table 6).
Intraoperative variables.
Postoperative variables.
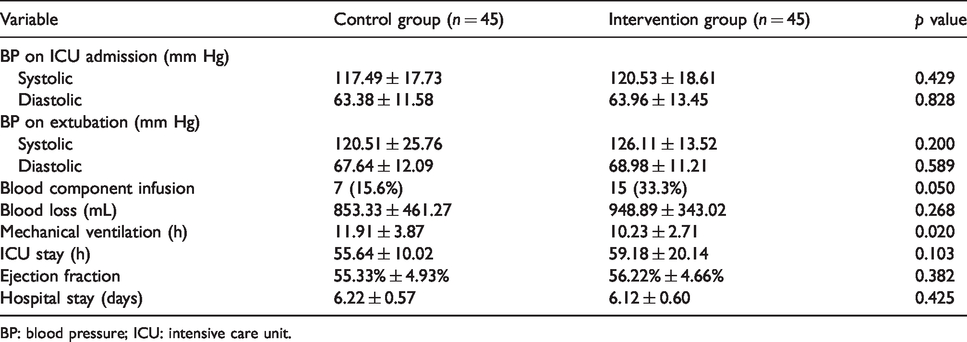
BP: blood pressure; ICU: intensive care unit.
Neecham confusion scores.
Severity of delirium.
Multivariable regression analysis of Neecham confusion score and patient variables.
Discussion
This study was undertaken to examine the effects of early planned mobilization on postoperative delirium in CABG patients. Data were collected on 90 hospitalized patients who underwent CABG. Mild postoperative delirium was common in our series, affecting 82.2% of patients. Our results show that early planned mobilization can reduce the incidence of postoperative delirium in patients undergoing CABG. These patients are at risk of developing postoperative delirium due to the complexity of the surgery, administration of anesthetic and sedative agents, and postoperative complications. Furthermore, postoperative delirium is likely to be caused by the synergistic effects of hypoperfusion and fast rewarming during cardiopulmonary bypass. 15 Postoperative delirium not only imparts distress to patients, families, and medical staff but also its development has been linked to an increased cost of care and cognitive recovery. Nevertheless, the exact etiology of postoperative delirium and cognitive impairment after CABG remains unclear. 16
Recent studies indicate that clinical practice guidelines are focused on non-pharmacologic therapies as first-line interventions for the management of postoperative delirium. Accordingly, healthcare staff should apply strategies to prevent and manage postoperative delirium, which can result in multiple negative impacts including increased length of ICU stay, hospitalization, and death. 17 To this end, the ABCDE bundle (awakening, breathing, coordination, delirium monitoring and management, early mobilization) was designed as an interdisciplinary patient-centered evidence-based strategy to prevent and reduce the risk of ICU delirium and weakness. 18
We observed statistically significant differences in the Neecham confusion score in terms of responsiveness, behavior, and overall score on the 2nd postoperative day in the intervention group. Our outcomes are consistent with Ziyaeifard and colleagues 19 findings showing that implementation of early mobilization has positive effects on cognitive outcome and ICU stay after cardiac surgery. In parallel with our results, a systematic review by Santos and colleagues 20 indicated that early mobilization is important to prevent postoperative complications, improve functional capacity, and reduce the length of ICU stay in patients undergoing cardiac surgery. Delirium is strongly associated with multiple factors such as advanced age, sex, and diminished cardiac function. Mobilization and exercise improve the sleep quality of patients by decreasing the levels of prostaglandin and tumor necrosis factor-α. Moreover, the increase in the Neecham confusion score in the intervention group may be related to an improvement in the tissue oxygenation level because of the mobilization practice.
There are several limitations to this study. First, our main objective was to assess the effects of early mobilization on postoperative delirium. Hence, development of delirium in a general ward or after discharge from the hospital may have been missed. Secondly, because of the short observation period and small sample size, our statistical analysis might have limitations that require validation in a future trial with a larger sample. Finally, the present investigation was a single-center study and some predictors such as cerebrovascular diseases due to aging and electrolyte disturbances may have not been included. Therefore, our results should not be generalized to all CABG patients. We concluded that early mobilization could reduce delirium as assessed by the Neecham confusion scale following CABG. This intervention can be part of the routine care in the cardiac ICU to enhance cognitive function and decrease the risk of postoperative delirium.
Footnotes
Acknowledgements
This article is adapted from a Master of Science thesis in nursing approved by Islamic Azad University of Isfahan (Khorasgan). We are sincerely grateful to Khorasgan Islamic Azad University Welfare Organization, the cooperation of nursing homes, and all aged people who participated in the codification and writing of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.