
Abstract
An 85-year-old man with appetite loss, lightheadedness, and leg edema was referred to our institution. Computed tomography and transthoracic echocardiography revealed a left ventricular pseudoaneurysm with a maximal diameter of 80 mm and severe mitral regurgitation. Coronary angiography showed 90% stenosis and total occlusion of the left circumflex artery at segments 11 and 12, respectively. He was diagnosed with postinfarction left ventricular pseudoaneurysm and underwent patch repair using two bovine pericardium patches and biological glue, mitral valve replacement, and coronary artery bypass grafting. His postoperative course was uneventful.
Introduction
The appropriate repair technique for postinfarction left ventricular pseudoaneurysm remains controversial. We describe a case of double-patch and glue repair of a postinfarction left ventricular pseudoaneurysm.
Case report
An 85-year-old man presented with appetite loss, lightheadedness, and edema of his legs. He was referred to our hospital with the diagnosis of heart failure 18 days after the onset of symptoms. Computed tomography and transthoracic echocardiography revealed a left ventricular (LV) pseudoaneurysm with a maximal diameter of 80 mm and severe mitral regurgitation (Figure 1a, 1b). Coronary angiography showed 90% stenosis and total occlusion of the left circumflex artery at segments 11 and 12, respectively (Figure 1c). Myocardial infarction with unknown onset was considered to be the cause of the LV pseudoaneurysm. Surgery was performed via a median sternotomy. Cardiopulmonary bypass was initiated with cannulation of the ascending aorta and the right atrium. Moderate hypothermia was induced. After aortic crossclamping, antegrade and retrograde cold blood cardioplegia was administered. Severe adhesion was found around the pseudoaneurysm. After incision of the pseudoaneurysm, a 25-mm hole was noted between the base of the LV and the pseudoaneurysm (Figure 2a). Two round-shaped bovine pericardial patches were sutured using 4-0 polypropylene sutures: one circumferentially on the LV side (Figure 2b, 2c) and another outside with a Dacron patch (Figure 2d). Subsequently, BioGlue (CryoLife, Inc., Kennesaw, GA, USA) was injected between the patches (Figure 2e). The wall of the pseudoaneurysm was closed using a continuous suture with reinforcement of Dacron felt and BioGlue (Figure 2f, Figure 3). After pseudoaneurysm repair, mitral valve replacement using a Magna mitral 27-mm prosthesis (Edwards Lifesciences Corporation, Irvine, CA, USA) and coronary artery bypass grafting to the posterolateral branch of the left circumflex artery using a saphenous vein graft were performed. The total operation time, pump run, and aortic crossclamp times were 511, 386, and 278 minutes, respectively. The patient was extubated on postoperative day 5 and did not develop acute kidney injury or require dialysis. His intensive care unit stay was 8 days. Postoperative computed tomography and transthoracic echocardiography showed complete closure of the pseudoaneurysm. He was discharged to a healthcare facility for rehabilitation on postoperative day 15. His condition was good at the 9-month follow-up.
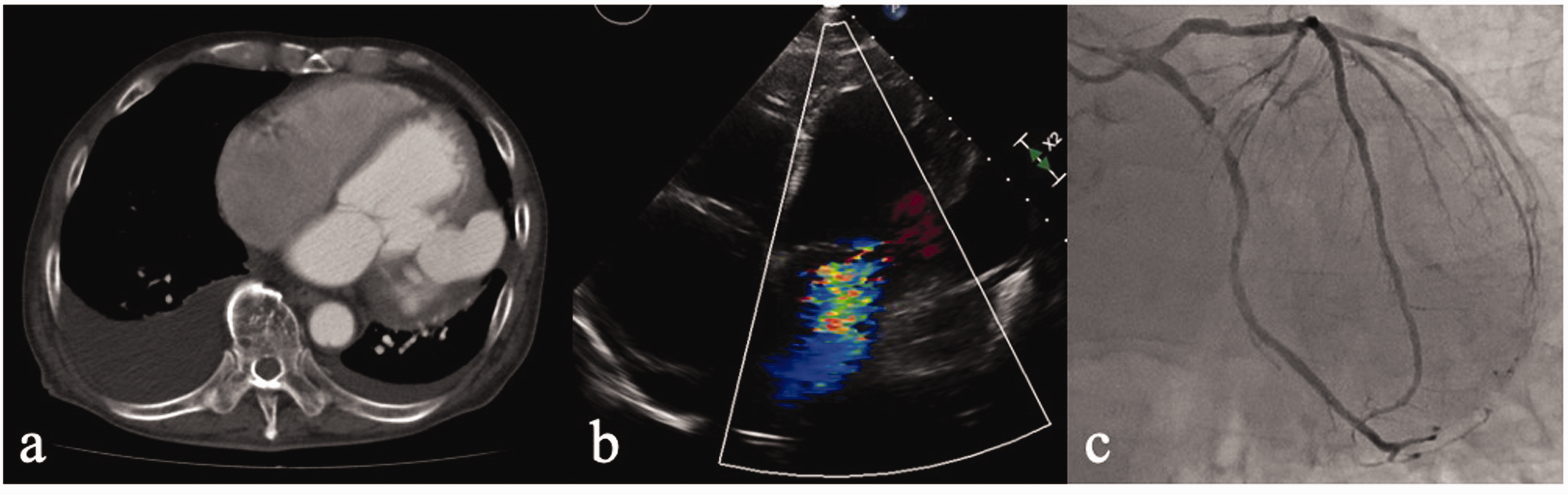
(a) Computed tomography revealing a left ventricle pseudoaneurysm with a maximal diameter of 80 mm. (b) Transthoracic echocardiography showing mitral regurgitation. (c) Coronary angiography demonstrating stenosis of the left circumflex artery.

(a) The communication between the pseudoaneurysm and the left ventricle via a 25-mm hole. (b) A round-shaped bovine pericardial patch was sutured circumferentially on the left ventricular side using 4-0 polypropylene sutures. (c) The pericardial patch was inserted into the left ventricle. (d) Another round-shaped bovine pericardial patch and a Dacron patch were sutured outside the left ventricle, using 4-0 polypropylene sutures. (e) BioGlue was injected between the two pericardial patches. (f) The pseudoaneurysm was closed using a continuous suture with Dacron felt reinforcement.
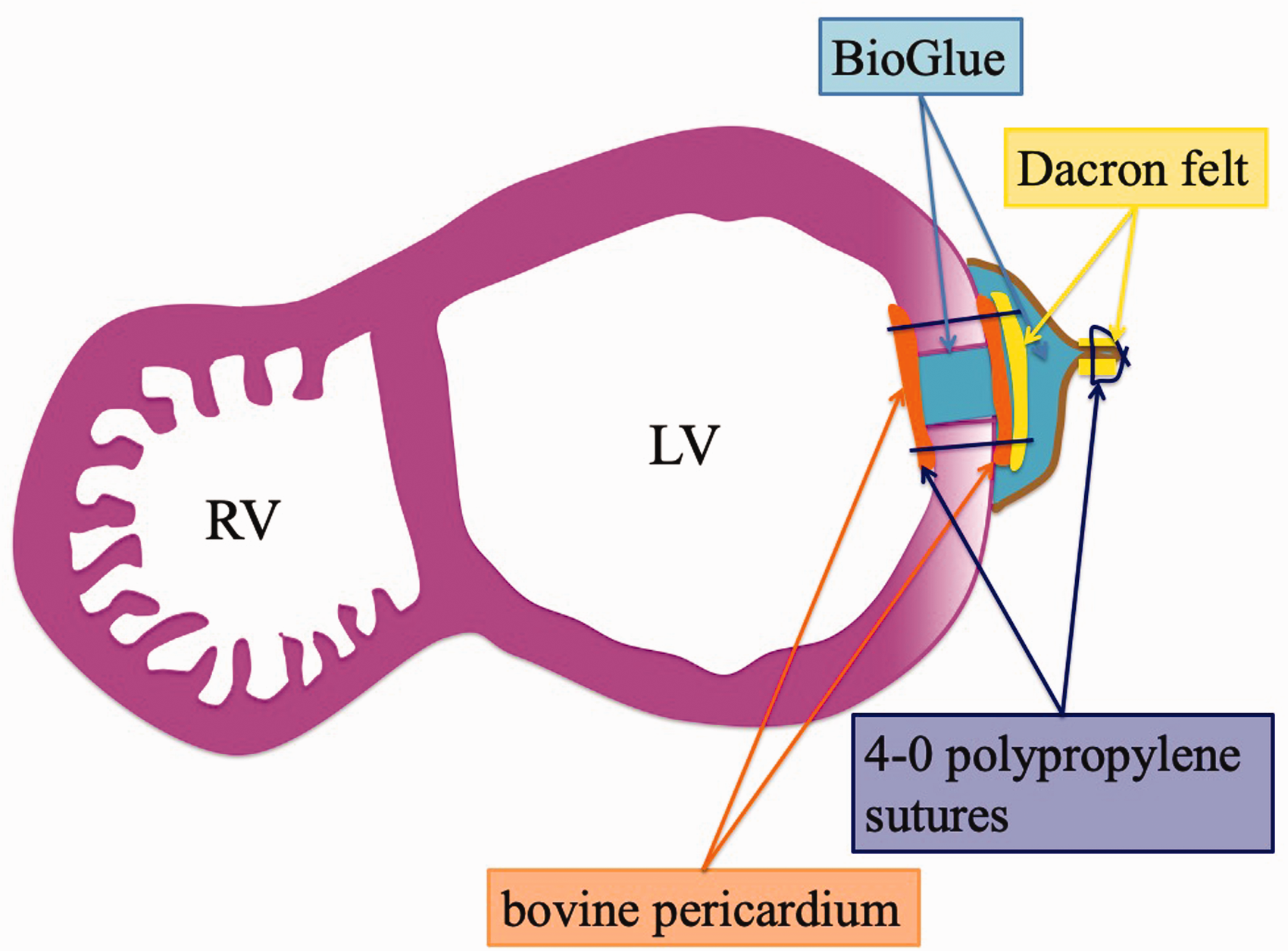
Schema of the repair using two patches and BioGlue. LV: left ventricle; RV: right ventricle.
Discussion
Several pathologies can cause LV pseudoaneurysm, among which, myocardial infarction accounts for 55% of cases.1–4 Clinical presentations of LV pseudoaneurysm include congestive heart failure, mitral regurgitation, tachyarrhythmia, systemic thromboembolism, and cardiac rupture. However, specific symptoms do not necessarily manifest and the diagnosis of pseudoaneurysm can be delayed. 3 , 4 Because an untreated LV pseudoaneurysm has a 30%–45% risk of rupture, 5 , 6 surgical repair is advocated. 2 Urgent surgery is recommended when a pseudoaneurysm is discovered within 2–3 months after the onset of myocardial infarction because the timing of rupture is unpredictable. 1 , 2 On the other hand, when diagnosis is made years postinfarction, the need for surgery is determined by symptoms rather than by the risk of rupture. 3 , 4 The overall early postoperative mortality rate of postinfarction pseudoaneurysm ranges from 20% to 36%.1–3, 7 Moreover, additional valve surgery and coronary artery bypass grafting is suspected to increase the perioperative mortality rate. 8
In chronic cases or cases in which the communication between the LV and the pseudoaneurysm is small, direct closure using horizontal mattress sutures with Teflon felt strips is usually employed. 1 , 2 , 7 In acute cases with a necrotic fragile myocardium, patch repair with synthetic or pericardial patches is safe and effective. 8 When the defect in the LV is large or located near the base of the heart, double-patch repair can directly restore the LV physiological geometry. 8 In our case, although the infarcted myocardium around the pseudoaneurysm was not fragile, the communication between the LV and the pseudoaneurysm was too large to be sutured directly. We used a pericardial patch on the LV side to prevent thrombosis formation, despite no clear evidence of its superiority; further studies with a larger sample and longer follow-up are necessary to evaluate the results of double-patch repair.
In our patient, postoperative patch dehiscence could result in fatal bleeding and sudden death. Although the cytotoxic effect of BioGlue remains a concern, we chose to use it for double-patch repair. Following the manufacturer’s instructions, we ensured that the applicator tip was appropriately primed before using BioGlue. Careful follow-up is needed to detect signs of recurrent pseudoaneurysm. Reoperation can be required in some patients for recurrent pseudoaneurysm, although the frequency is low. 2 , 3 In our patient, there was no sign of recurrence noted on echocardiography at the 9-month follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.