
Abstract
Background
Although carotid artery disease can occur in patients who have coronary artery disease (CAD), ostial stenosis of a left common carotid artery (CCA) along with CAD is a rarely reported condition.
Case report
We describe a rare case of severe stenosis of the left CCA ostium and CAD, which were successfully treated with an off-pump coronary artery bypass and aorto-left CCA bypass. This strategy minimizes the risk of perioperative strokes. Furthermore, an aorto-supra aortic trunk bypass provides a more physiological blood flow pattern than cerebral approaches. This approach would be a safe and effective treatment option.
Keywords
Introduction
Proximal common carotid artery (CCA) stenosis is an unusual condition with a prevalence of between 1% and 2% out of all carotid artery cerebral ischemia cases. We report a rare case of a surgical repair of severe stenosis of a left CCA ostium and coronary artery disease (CAD).
Case presentation
A 76-year-old man presented with an asymptomatic stenosis of the left CCA ostium. He had a history of a brain embolization and percutaneous coronary intervention for an acute myocardial infarction. Angiography revealed a severe stenosis at the origin of the left CCA (Figure 1). Additionally, he had CAD, and coronary angiography revealed in-stent restenosis of the mid-left anterior descending artery (LAD) stent. The proximal segment of the intermediate (IM) branch and distal segment of the right posterior descending artery (PDA) had severe stenosis.
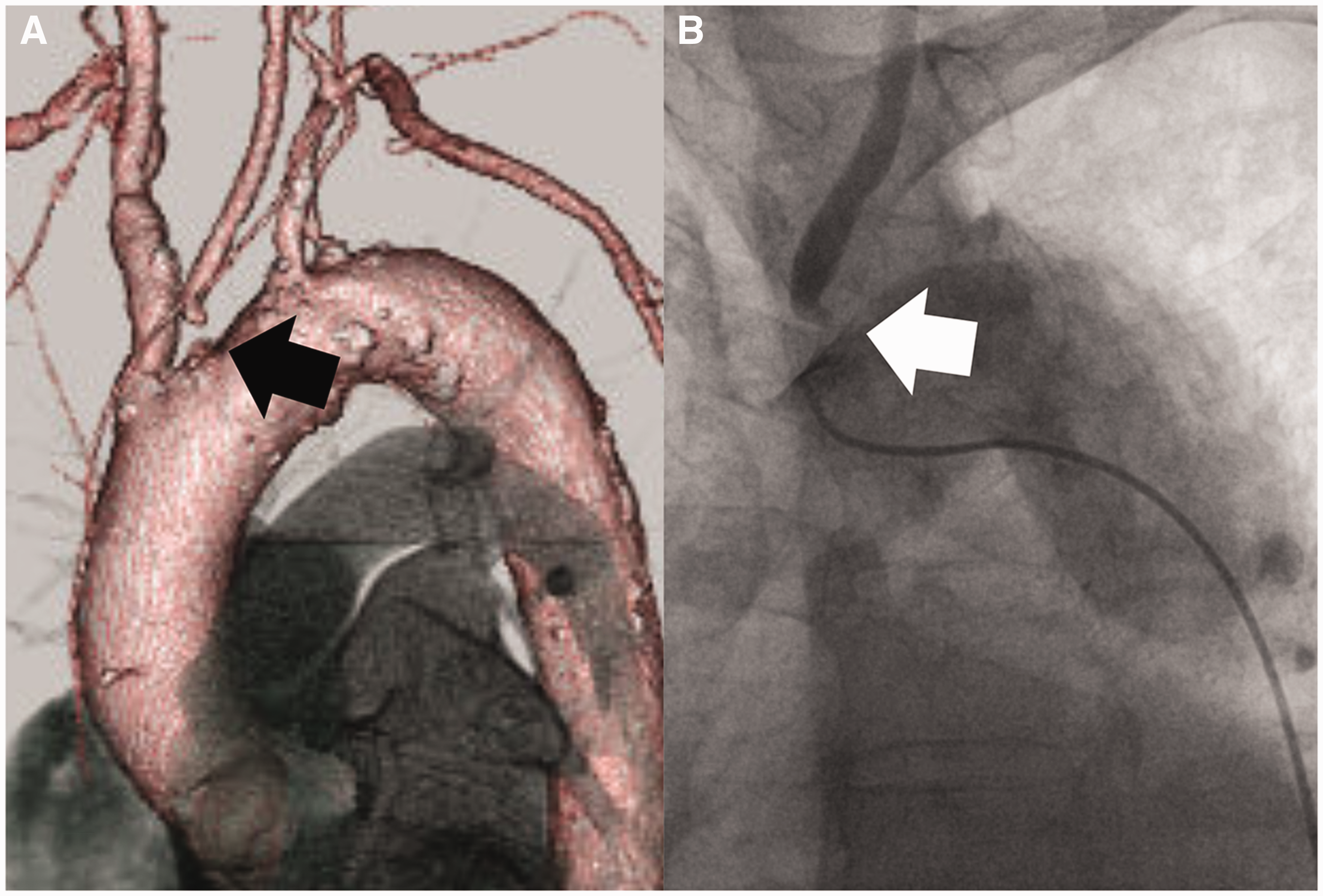
(A) Preoperative computed tomography angiography in the left lateral view showing a severe stenosis of the left CCA ostium (black arrow). (B) Preoperative angiography in the left lateral view demonstrates a 99% stenosis of the left CCA origin (white arrow).
We planned an off-pump coronary bypass (OPCAB) (left internal thoracic artery (ITA)-LAD and saphenous vein (SV) graft-IM-PDA) and ascending aorta to the left CCA bypass. After a median sternotomy, the left ITA was harvested and the SV was dissected. Following that, three distal anastomoses were performed. The left ITA was anastomosed to the LAD, and the SV was anastomosed to the IM and the PDA. Then, we evaluated the aortic wall before both proximal anastomoses of the SV and a 9 mm tubular graft. Under a single side-biting clamp, a 9 mm tubular graft and the proximal site of the SV were anastomosed to the aorta. Finally, the distal end of the 9 mm graft was anastomosed to the left CCA in an end-to-end fashion (Figure 2A). During the procedure, we monitored the cerebral oxygen saturation using a Foresight (CAS Medical Systems Inc., Branford, Connecticut, USA). We did not use a shunt tube during the distal anastomosis of the CCA because the cerebral oxygen saturation revealed no significant change after carotid clumping. The patient’s recovery was uneventful and postoperative computed tomography showed patent grafts (Figure 2B). External ultrasonography showed that the peak systolic velocity in the common carotid artery (CCA) increased from 9.6 cm/s to 24.5 cm/s after the surgery.
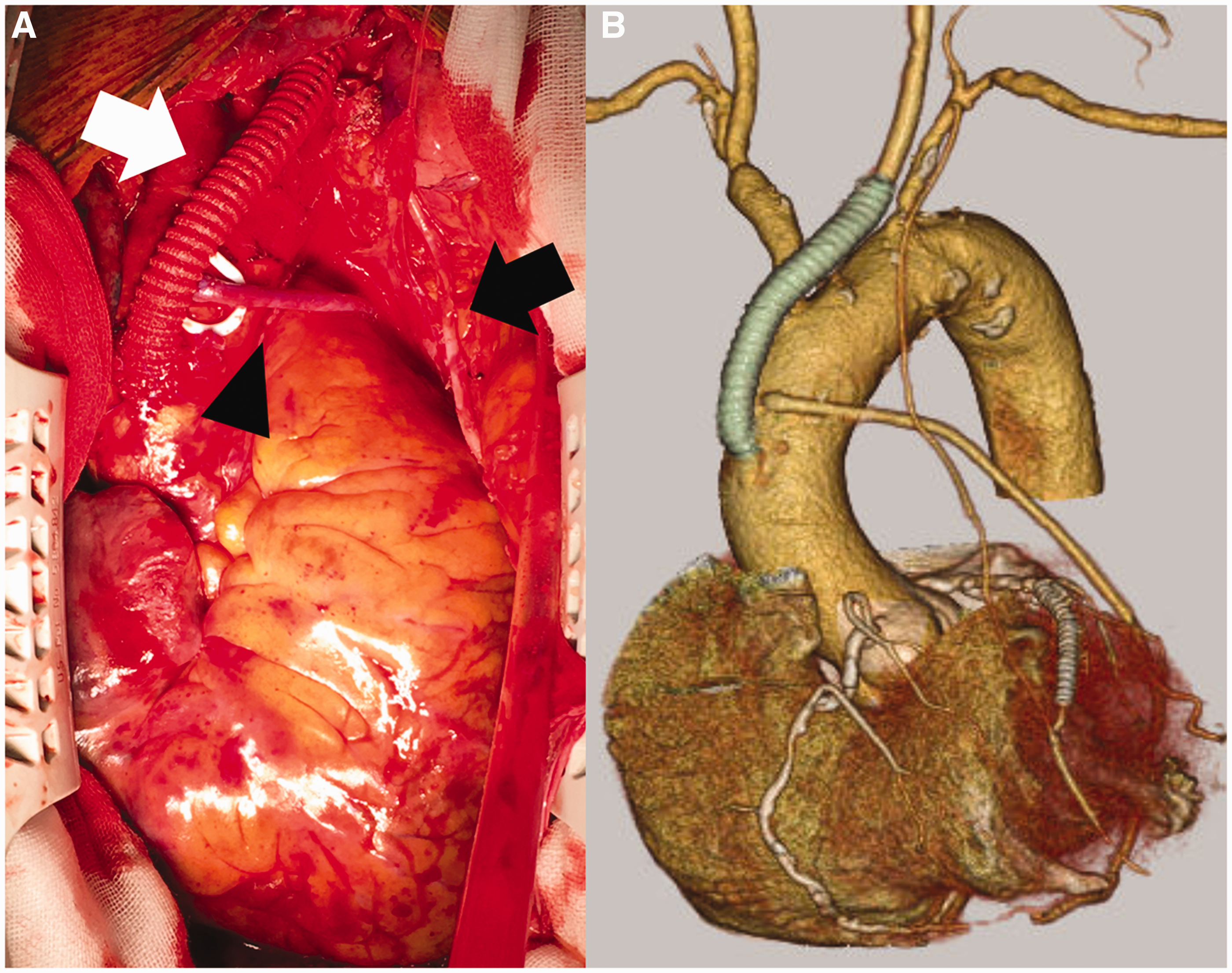
(A) Intraoperative view showing the aorto-left CCA bypass (white arrow), left ITA (black arrow), and SV (black arrow head). (B) Postoperative computed tomography angiography presenting patency of the aorto-left CCA bypass and coronary artery bypass graft.
Discussion
Proximal CCA stenosis is an unusual condition with a prevalence of between 1% and 2% out of all carotid artery cerebral ischemia cases. Takach et al. reported a series of patients with a concomitant brachiocephalic reconstruction and coronary bypass grafting using cardiopulmonary bypass. 1 There have been only two reports describing a concomitant OPCAB and carotid revascularization for proximal CCA stenosis and CAD.2,3 Okamoto and Fukui reported an aorto-bilateral carotid artery bypass and OPCAB. Tazume et al. described an aorto-right subclavian artery bypass with OPCAB. On the other hand, in our patient, a severe stenosis was located only at the origin of the left CCA.
There are no established management guidelines for proximal CCA stenosis due to its rarity. Paukovits et al. described that the inclusion criteria of this lesion is a 70% luminal diameter stenosis in patients with ipsilateral ischemic neurologic symptoms or an 85% stenosis in asymptomatic patients. 4 Our patient was asymptomatic but had 99% stenosis at the origin of the left CCA.
An endovascular approach for proximal CCA stenosis is less invasive than open surgery and has recently become a common procedure. Some researchers have reported the transfemoral endovascular treatment of patients with proximal CCA lesions.4,5 However, in our case, an endovascular repair was not suitable for several reasons. First, the engagement of the guiding catheter and establishment of a backup support via the femoral artery was suspected to be difficult due to the ostial stenosis of the left CCA. Second, an endovascular repair from either a transfemoral or transcarotid approach had a risk of embolization because the preoperative CT showed a vessel thrombus and calcification of the aortic arch.
The OPCAB and aorto-supra aortic trunk bypass has several advantages. First, OPCAB has the advantage of avoiding other morbidities associated with cardiopulmonary bypass. Second, the aorto-supra aortic trunk bypass reportedly provides a more physiological blood flow pattern than cerebral approaches, such as a carotid-subclavian bypass. 6 Furthermore, in our patient, the ascending aorta and distal site of the left CCA were seen to be relatively healthy. Therefore, the side-bite clamping of the ascending aorta and clamping of the distal left CCA were considered to be a safe procedure. If the ascending aortic wall had been highly atheromatous, the side-bite clamping should have been avoided. In such cases, the proximal anastomosis of the SV using a suture device and the cerebral approach should have been performed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by the local research ethics committee (Reg. No. 9).
Informed consent
Written informed consent was obtained from the patient for publication of this case.