
Abstract
Cardiac calcified amorphous tumors are rare non-neoplastic intracavitary masses with unknown cause. A 60-year-old man presented with sustained ventricular tachycardia. Transthoracic echocardiography and contrast-enhanced angio-computed tomography demonstrated an expanding 73 × 40 mm sized calcified mass in the left ventricle. He underwent successful total removal of the mass and cryo-ablation at the normal myocardial border. Histopathological examination confirmed a diagnosis of cardiac calcified amorphous tumors. The postoperative course was uneventful, without ventricular tachycardia recurrence. To our knowledge, this is the first reported case of confirmed cardiac calcified amorphous tumors causing ventricular tachycardia and treated by surgical resection combined with cryo-ablation.
Introduction
Cardiac calcified amorphous tumors (CCATs) are rare non-neoplastic cardiac tumors, first described in 1997. 1 As the clinical features of CCATs resemble those of other cardiac tumors, including symptoms related to obstruction or embolization, they may be confused with primary cardiac neoplasms. Surgical resection is the only treatment to reduce symptoms, prevent embolization, and obtain a pathologic diagnosis. Herein, we report a rare case of CCATs with sustained ventricular tachycardia (VT), successfully treated by surgical resection combined with cryo-ablation.
Case report
A 60-year-old man was admitted to our emergency department with loss of consciousness and a functioning implantable cardioverter defibrillator (ICD). His medical history included ICD implantation for ventricular fibrillation (VF), hypertension, dyslipidemia, diabetes mellitus, and chronic atrial fibrillation. While examining for VF, a cardiac fibroma (54 × 26 mm) in the left ventricle (LV) was diagnosed using transthoracic echocardiography (TTE), computed tomography (CT), and enhanced magnetic resonance imaging. We proposed surgery for LV mass, but he refused. Instead, he underwent regular follow-up examinations. TTE, transesophageal echocardiography, and enhanced CT demonstrated normal LV function (ejection fraction of 69% and mild MR) and an enlarged calcified mass (73 × 40 mm) originating from the inferior wall of the LV (Figure 1(a) and (b)). However, even after increasing the β-blocker dose and initiating a new antiarrhythmic drug, sustained VT frequently recurred (Fig.1C) and ICD delivered shocks. We assumed that sustained VT was related to the growing LV mass. Since medical treatment was ineffective, surgical resection was performed.
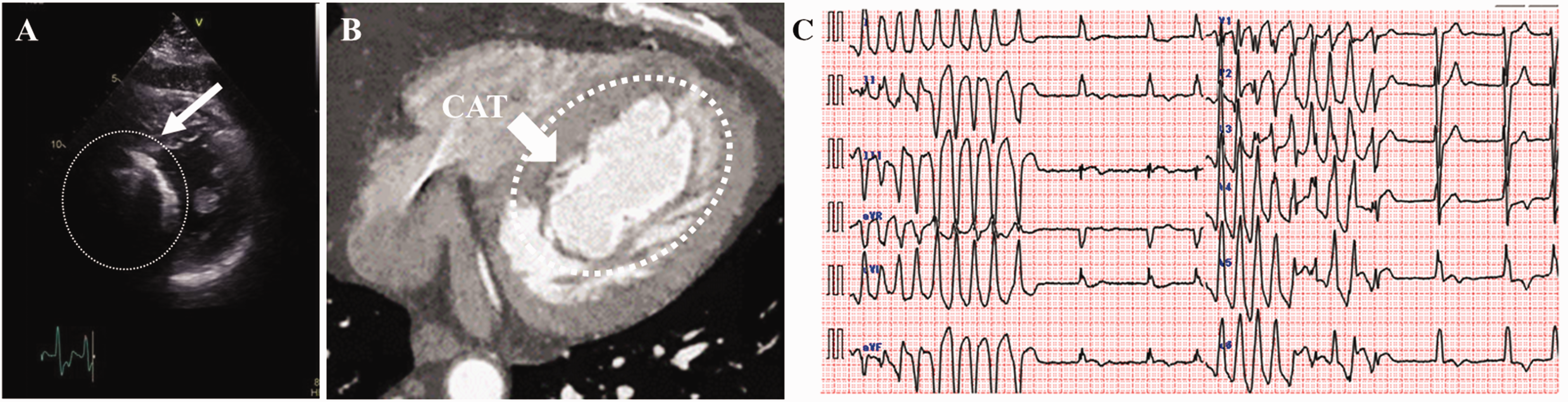
(a) Transthoracic echocardiogram of the short-axis view reveals a calcified tumor in the left ventricle. (b) Enhanced computed tomography reveals a calcified mass emanating from the inferior wall of the left ventricle. White arrow, calcified amorphous tumor (CAT). (c) Presenting electrocardiogram shows ventricular tachycardia originating from the left ventricle.
The LV was approached through the apex. Massive gray-white necrotic tissue leaked from the mass upon incision of the apex (Figure 2(a)). The tumor protruded from the septal side into the LV and reached the inside of the posterior papillary muscle. All visible masses, including the papillary muscle calcification, were excised (Figure 2(b)). The tumor in the posterior papillary muscle was resected together with the capsule, and the posterior papillary muscle was fixed to its original position using a 4-0 Prolene suture with a felt strip. Cryo-freeze coagulation using cryoICE (AtriCure, USA) was performed around the border between the normal myocardium and the removed mass from the lumen (Figure 2(c)). A pericardial patch was sewn into the LV, excluding the papillary muscle to prevent mitral regurgitation (MR). Finally, the LV incision was repaired by another bovine pericardial patch strip for outer reinforcement. He had an uneventful postoperative recovery, without recurrence of VT during the one-year follow-up. Postoperative TTE showed an ejection fraction of 44% and mild MR. Histopathologic examination revealed amorphous debris, fibrinous material, and calcified nodules, consistent with a CCAT diagnosis (Figure 3(a) and (b)).
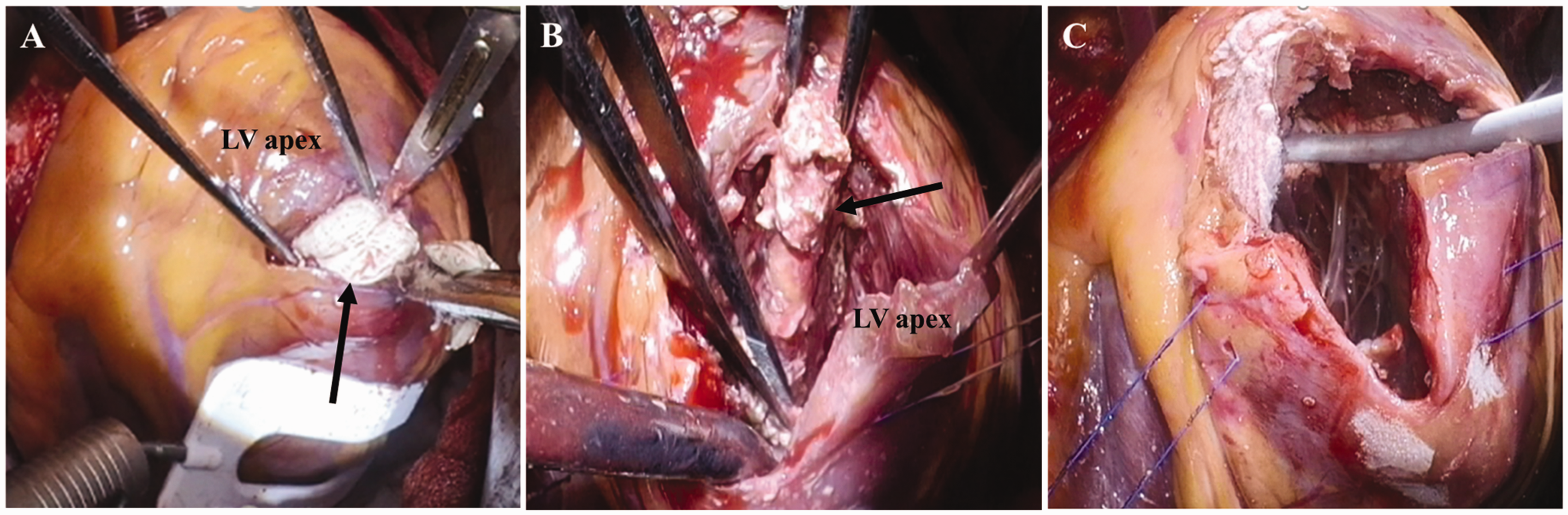
(a) Intraoperative presentation from the left ventricle apex shows massive gray-white necrotic tissue leaking from the tumor (black arrow). (b) Complete excision of the tumor (black arrow), including the papillary muscle calcification, was performed. (c) Cryo-freeze coagulation using cryoICE was performed all around the border between the normal myocardium and the excised tumor from the lumen. CAT: calcified amorphous tumor.
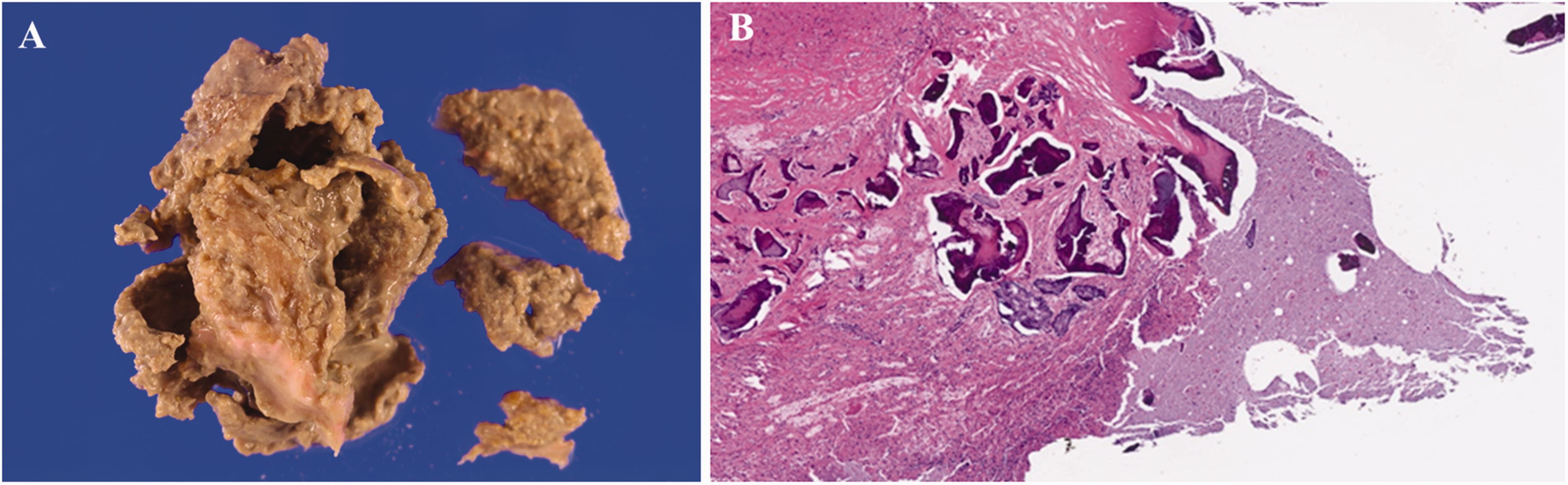
(a) Macroscopic appearance of the mass. (b) Microscopic appearance of the mass. Histopathologic examinations show amorphous debris, fibrinous material, and calcified nodules (hematoxylin and eosin ×10).
Comment
The histologic features of CCATs comprise nodular calcium deposits in a background composed of fibrin or amorphous fibrillary materials. However, the origin and etiology of CCATs remain unclear.
Although case reports of CCATs exist, discussions regarding the epidemiology, clinical imaging, treatment, and convalescence of CCATs are mainly indistinct. Patients typically present with dyspnea, syncope, and systemic embolism. 2 Surgical total tumor resection remains the only curative procedure, if symptomatic. However, recurrence has been previously reported in a patient who underwent incomplete resection of a right ventricular CCAT. 3
Based on a review of 80 reported cases of CCATs from 1997 to 2019, CCATs most frequently originate from the mitral valve and annulus (34/80 cases), with only 8/80 cases of LV CCATs. 2 , 4 , 5 Additionally, there is only one previous report of sustained VT resulting from CCATs, 6 and no reports on the surgical resection of a CCAT due to VT.
In the present case, VT occurred concurrently with an increase in CCAT size, and was resistant to antiarrhythmic therapy. Therefore, we considered surgical resection to be necessary. Tumor-induced VT has been reported, and two causes have been considered. 7 First, altered myocardial architecture might lead to dispersed repolarization, anisotropic conduction, and micro-reentry. Second, humoral elements released from myocardial cells or the direct compression of myocardial fibers might lead to automatic ventricular arrhythmias. Additionally, we performed cryoablation on the tumor excision area and normal myocardial border, similar to a previous report that performed cryoablation, with electroanatomical mapping assistance, for recurrent VT after surgical tumor resection. 8
Clinical studies have suggested that CCATs are very fragile and at risk of systemic embolization.3–5 We repaired the CCAT resection surface with a bovine pericardial patch to prevent it from coming into contact with the LV cavity, as the CCAT contents could spread and cause an embolism. Based on the present case, surgical tumor resection and cryoablation at the border of the normal myocardium might be considered effective for preventing VT recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.