
Abstract
Objective
Destroyed lobe of the lung is always secondary to chronic or recurrent lung infections with irreversible damage of pulmonary parenchyma. In this study, we analyzed surgical technique, post-operative complications, mortality, and long-term outcomes of patients undergoing lobectomy of pulmonary lobe destruction.
Materials and methods
A retrospective study of 47 patients that underwent lobectomy due to a destroyed lung parenchyma between January 2010 and December 2019 were reviewed with an average follow-up period of 39 months.
Results
The study included 47 patients with a mean age of 39.4 years. The etiology of lobe destroyed was tuberculosis in 15 (31.9%), non-tuberculosis bronchiectasis in 20 (42.5%), aspergilloma in 09 (19.1%), hydatid cyst in 2 (4.3%), and a mis-diagnosed intrabronchic foreign body in 1 (2.1%). Surgical approach was through posterolateral thoracotomy in 44 (93.6%) patients and video-assisted thoracoscopic surgery in only 3 patients. Mean operative time was 153 min and mean post-operative hospital stay was 7.9 days. The post-operative complications occurred in five (10.6%): atelectasis (n = 2), wound site infection (n = 1), prolonged air leak (n = 1), and hemothorax in one case. No post-operative mortality was noted. A good clinical result was observed in 87.2% of cases.
Conclusion
Surgical treatment of destroyed lobe is a high risk associated surgery. Tuberculosis and aspergilloma are the most common etiologies. Favorable result was obtained in selected patient with an excellent perioperative care.
Introduction
Destroyed lung lobe is always secondary to chronic or recurrent lung infections. These irreversible damage of pulmonary parenchymal lobe is mostly caused by tuberculosis, the first etiology in our and other countries with underdeveloped health systems.1,2
Lobectomy exceptionally pneumonectomy for destroyed parenchyma is the only best treatment to cure definitively the symptoms, although it is accompanied with surgical difficulties and post-operative complications.
The aim of this study was to evaluate the results of surgical treatment (lobectomy or more, pneumonectomy are excluded) in patients with a diagnosis of pulmonary lobe destruction.
Materials and methods
During the 10-year period, January 2010 to December 2019, our retrospective study included 47 patients that underwent lobectomy or more due to a destroyed lung lobe.
Patient characteristics and medical history, clinical symptoms, etiologies, site of the destruction, pre-operative evaluation, intra- and post-operative complications, mortality, hospital stay, and long-term follow-up outcomes were noted (Tables 1 and 2).
Clinical characteristics of the patients with destroyed lung lobe.
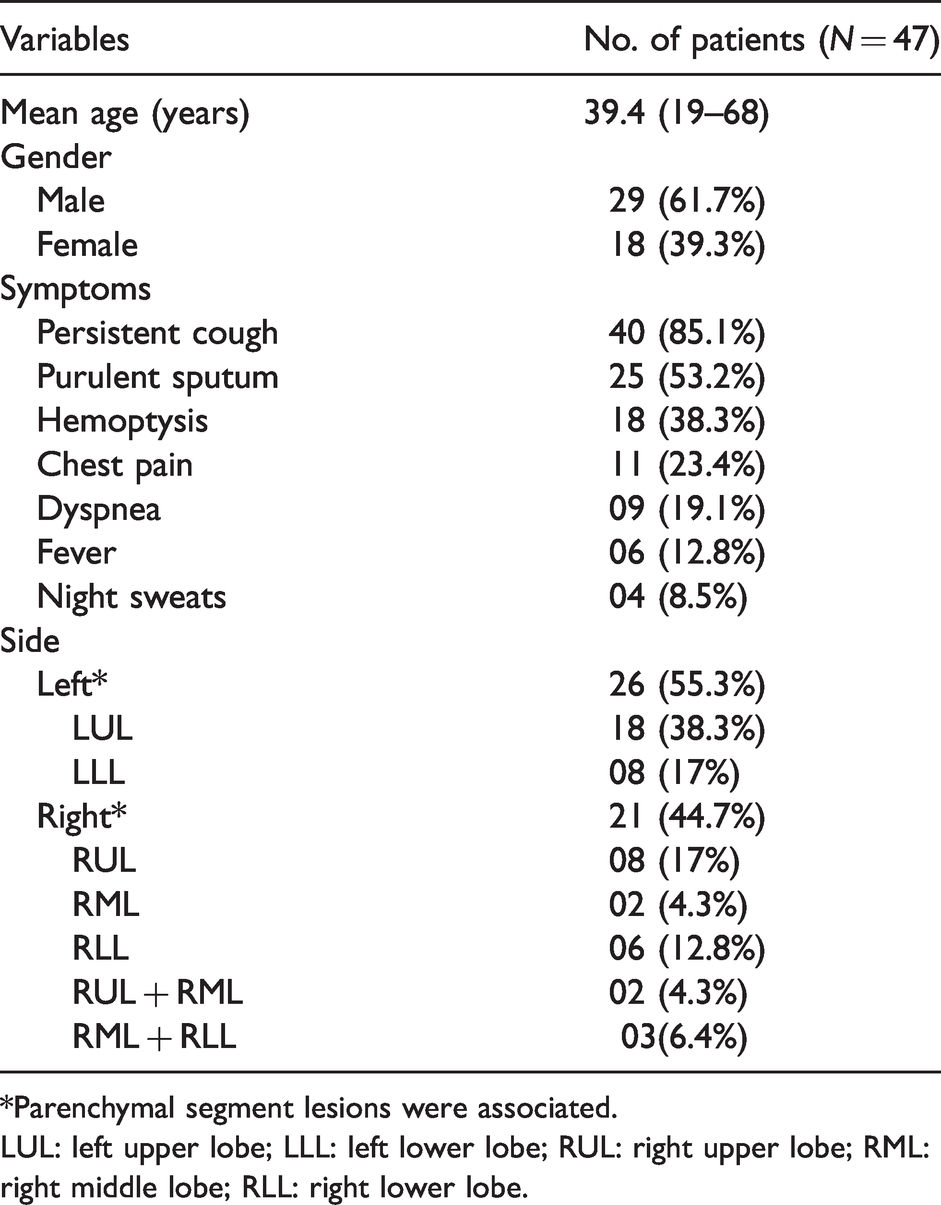
*Parenchymal segment lesions were associated.
LUL: left upper lobe; LLL: left lower lobe; RUL: right upper lobe; RML: right middle lobe; RLL: right lower lobe.
Findings data of the patients with of destroyed lung lobe.
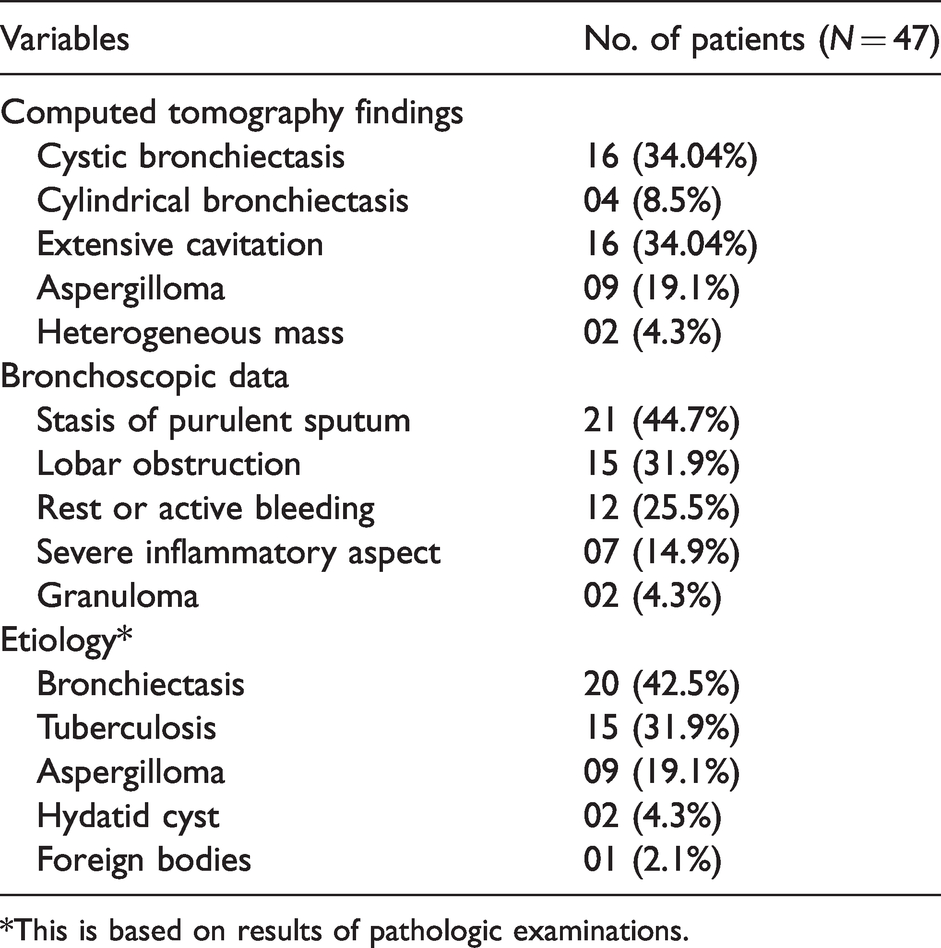
*This is based on results of pathologic examinations.
Pre-operative chest X-ray (Figure 1(a) to (f)) and chest computed tomography (CT) was performed in each patient (Figure 2(a) to (d)). The diagnosis of destroyed lung lobe is defined by radiology as a total destruction of the pulmonary lobe with the evidence of irreversible parenchymal damage, presence of severely forms of lobe bronchiectasis, big cavities or complex aspergilloma with diffuse pleural thickening and chest wall retraction.

Chest X-ray showing a dense infiltration in the right upper lung field (a); bronchiectasis of the upper left lobe (b); bronchiectasis of the middle lobe (c); mass with cavity of the left lower lobe (d); aspergilloma of the upper left lobe (e); and cavities destroying the totality of the upper right lobe (f).
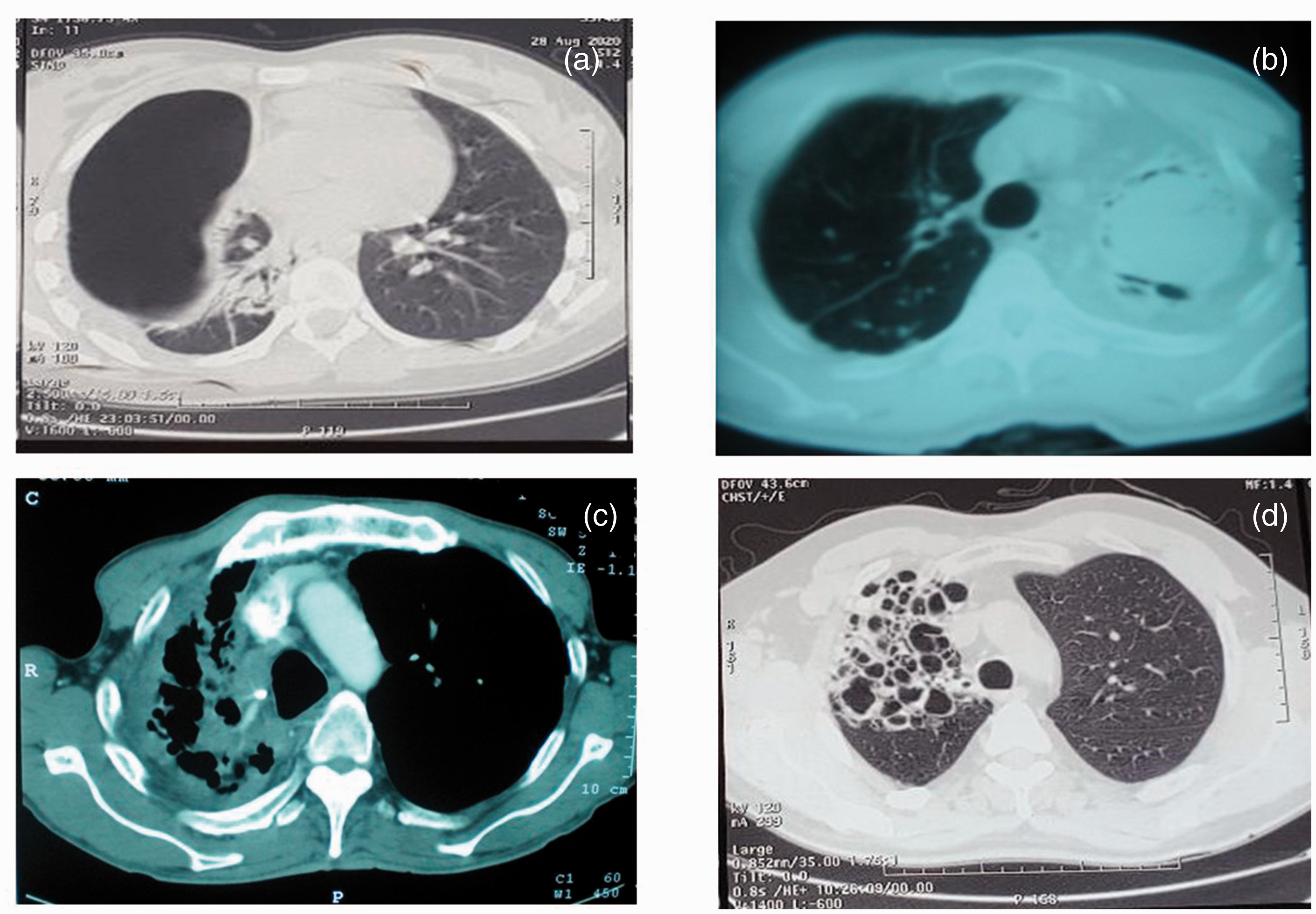
Chest computed tomography showing a giant cavity of the destroyed right upper lobe (a); aspergilloma of the upper left lobe (b); destruction of the right upper lobe (c); bronchiectasis of the upper left lobe (d).
All patients undergo usual laboratory tests and bronchoscopic exploration to research a local cause of destruction and to realize microbiological examination.
Positive serum aspergillus-antigen test confirmed the aspergillus infection in nine cases (19.1%) but the hydatidosis serology was negative in the five patients (10.6%) with suspicious hydatid disease (history of surgery for hepatic hydatid cyst in three cases and radiological appearance of hydatid membrane in CT scan (heterogeneous mass like a bronchial rupture of the cyst) in two case.
Pre-operative exploration of the respiratory function tests included arterial blood gas test, forced expiratory volume in 1 s (FEV1), forced vital capacity and sometimes a six-min walk test (6-MWT). Because of nonfunctional destroyed parenchyma, ventilation-perfusion scan was not realized and spirometry was sufficient.
A pre-operative anesthetist consultation was necessary to evaluate the cardiac function and to research others comorbidities.
In all the patients, we have preconized systematic respiratory physiotherapy and postural drainage, and antibiotics according to sputum culture results two to three weeks before surgery.
The antibacillar treatment was given to patients with tuberculosis diagnosed pathologically in the post-operative period during six months with standard regimen (2RHZE, 4 RH) (H: isoniazid, R: rifampicin, E: ethambutol; Z pyrazinamide) or more (12 or 24 months) in the four patients (8.5%), with multi-drug resistant tuberculosis.
Surgical technique
Surgery of destroyed lung parenchyma improves generally the ventilation function but when the patient has a limited preoperative function lobectomy should be performed with attention particularly when the concerned lobe contain normal functional areas of parenchyma.
All the patients were operated under general anesthesia with double-lumen endotracheal intubation confirmed by fiber-optic bronchoscopy. An aspiration of the tracheobronchial tree is performed in order to decrease sputum and to minimize the risk of intraoperative bronchial contamination.
The patients were placed in the contralateral decubitus position, and a classical posterolateral thoracotomy approach was performed in 44 (93.6%) patients (Figure 3(a)), and only 3 patients were operated via video-assisted thoracoscopic surgery (VATS) for middle lobe (n = 2) and left lower lobe (n = 1) bronchiectasis.
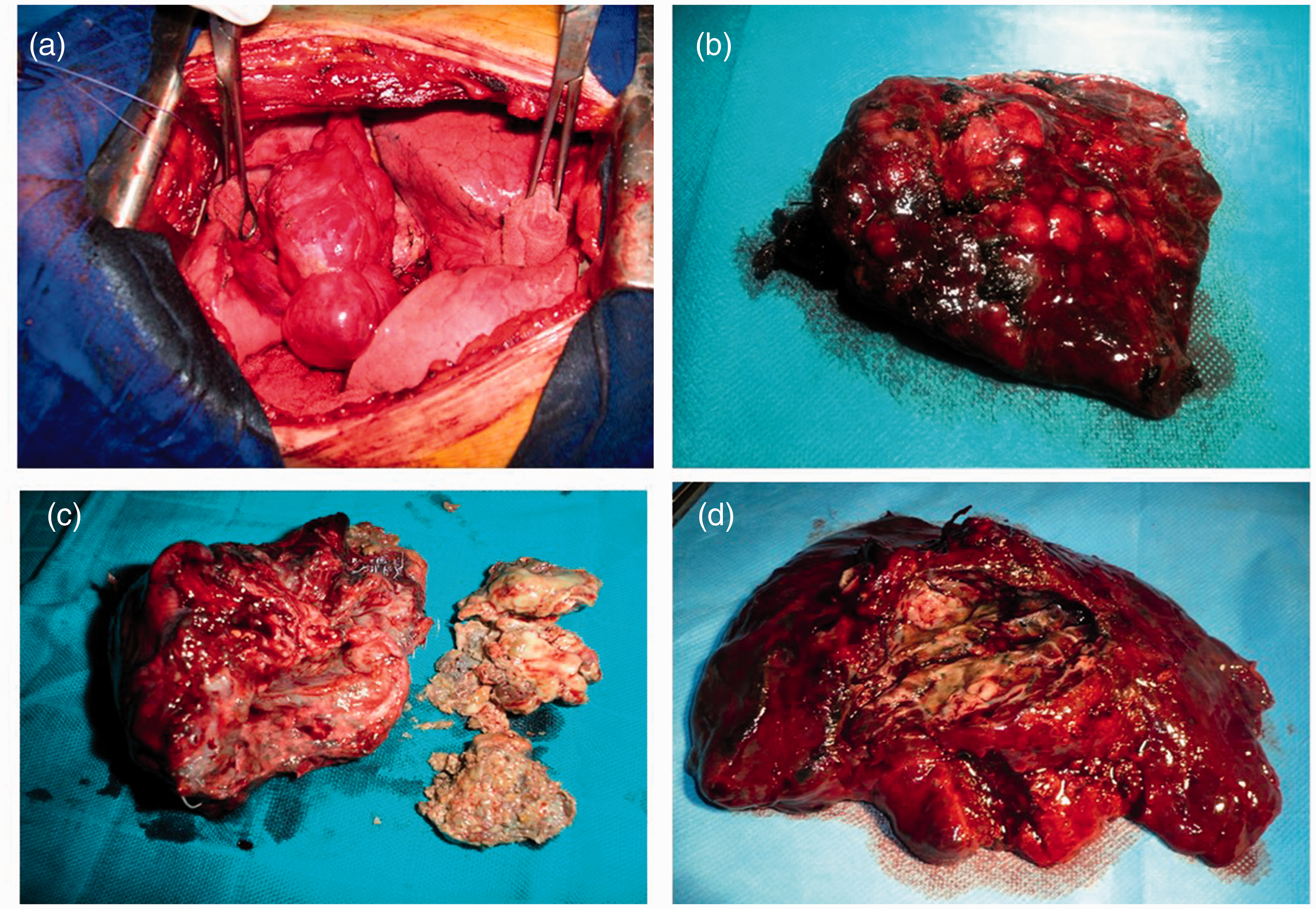
Operative views: posterolateral thoracotomy with destroyed right lower lobe by bronchiectasis (a); a right lower lobe bronchiectasis specimen (b); aspergilloma in the destroyed left upper lobe (c); tuberculous cavity of the right upper lobe (d).
The left side was concerned in 26 (55.3%) and the right side in 21 (44.7%) patients.
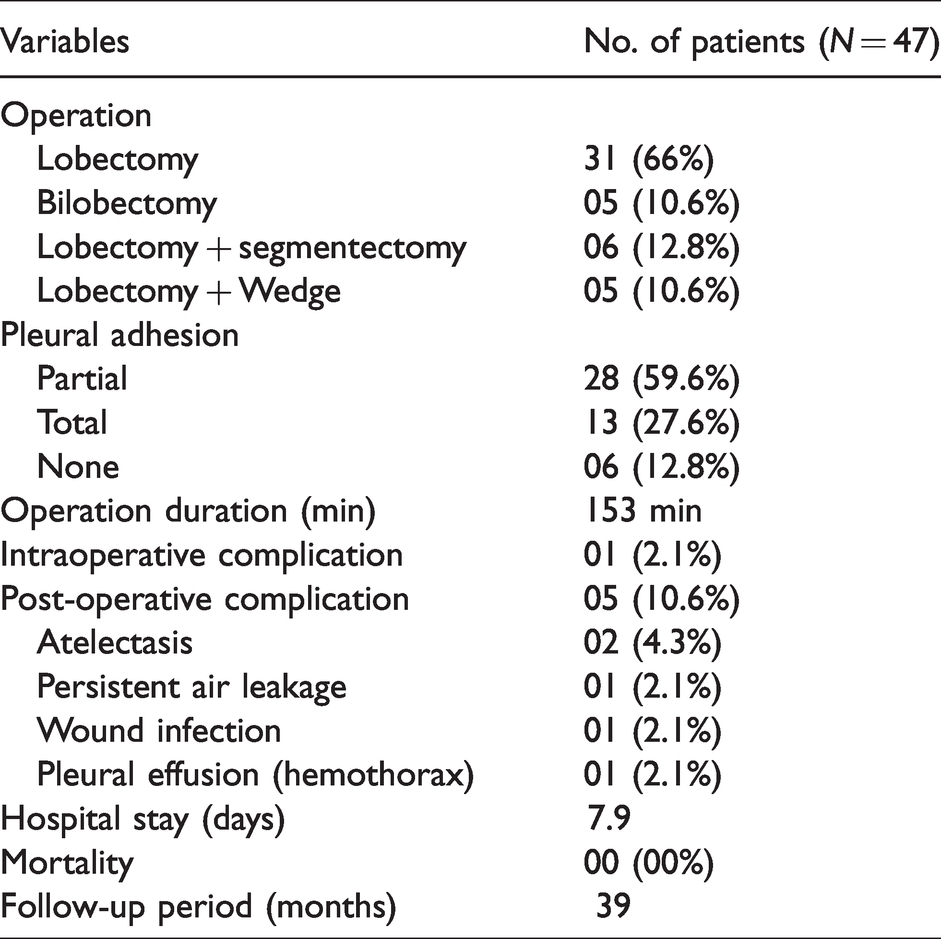
In all patients, lobectomy or more (bi-lobectomies or lobectomy associated with segmentectomy or wedge resection) were performed (Table 3). The dissection was difficult in 35 cases (74.5%) with severe pleural and pleuro-parenchymal adhesions. And in 11 patients (23.4%), we have used extrapleural space to progress in pulmonary liberation.
Operative and post-operative results of the patients.
After total lung liberation and vascular ligature, a great importance was given to bronchial stitches, the bronchus was cut open and the bronchial stump was made using separated stitches of 2/0 or 3/0 poly-diaxanone absorbable suture in 27 cases (57.4%) and closed using an endoscopic stapling device in 20 cases (42.6%). Finally, the bronchial stump was covered with pleural flap or adjacent tissues such as mediastinal and exceptionally pericardial or an intercostal muscle flap to prevent fistula development.
After a good hemostasis and acceptable pulmonary re-expansion, two chest tubes were inserted into the pleural space in all the patients and were transferred to the intensive care unit for 6 to 24 h. Then, our department if the patients are stable. Post-operative follow-up was performed using chest radiography and the chest tubes were removed successively (minimally one day) if the drainage volume was 200 ml or less with good radiologic control.
Results
Our study included 47 patients (29 men and 18 women) who were operatively treated due to a destroyed lung lobe between 2010 and 2019. The patients had a mean age of 39.4 (range 19–68) years.
The main respiratory symptoms found in our patients were persistent and chronic cough in 40 cases (85.1%), whereas purulent sputum in 25 (53.2%), hemoptysis by 18 (38.3%), and chest pain by 11 (23.4%) patients. The apparition of chronic symptoms were from 1 to 15 years (mean: 6 years), which is due to frequent medical visits and frequent hospitalization. No case of bilateral lesions.
The bronchoscopy showed a stasis of purulent sputum in 21 cases (44.7%), lobar obstruction in 15 patients (31.9%), rest or active bleeding in 12 cases (25.5%), inflammatory aspect of the bronchial tree in all cases but severe in 7 (14.9%) and granuloma in 2 (4.3%) cases and suspicious of probable foreign body in 1 case (2.1%).
No patient have positive acid-fast bacillus in sputum (direct exam and/or culture) but Streptococcus pneumonia was detected in 11 cases (23.4%), Haemophilus influenzae in 7 (14.9%), Klebsiella pneumoniae in 4 (8.5%), more than two in 4 cases (8.5%) and sterile in the other cases.
Hemoptysis is the most life-threatening complication, in our exercise patient with minim hemoptysis are submitted to medical hemostatic treatment with scheduled surgery. However, when the hemoptysis was abundant, arterial embolization is performed and in the case of life-threatening bleeding it became a surgical emergency.
The indication of surgery was made only in symptomatic patients; first with hemoptysis, recurrent infection resistant to medical treatment, chronic purulent sputum, or frequent hospitalization for severe bronchopneumonia and poor or reduced quality life. In one patient with severe hemoptysis and destroyed right upper lobe, preoperative embolization was realized to reduce intraoperative blood loss and surgical difficulty.
Pre-operative respiratory function tests were performed in all patients and arterial blood gas test in only six patients. Mean pre-operative FEV1 was 2.72 l (range 1.86–3.43) and 74.7% (range 68–92%) of the predicted FEV1.
The operative time ranged from 80 to 320 min (mean 153 min). One intraoperative complication (bleeding: 650 ml) occurred in a patient with complex aspergilloma of the left upper lobe.
The etiology of the underlying primary diseases included nonspecific bronchiectasis in 20 (42.5%) (Figure 3(b)), complex aspergilloma in 15 cases (31.9%) (Figure 3(c)), tuberculosis in 9 (19.1%) which 4 (8.5%) were multi-drug resistant (Figure 3(d)), complicated hydatid cyst in 2 (4.3%), misdiagnosed foreign body located in the right lower lobe in 1 (2.1%) patient and right middle lobe syndrome caused by nontuberculous enlarged lymph nodes.
The post-operative morbidity rate (occurring within 30 days post-operatively) was 10.6% (five patients), including atelectasis associated with stasis of secretions in two (4.3%), persistent pulmonary air leak in one (2.1%), wound site infection in one patient (2.1%), and hemothorax in one case (2.1%), requiring a reoperation for diffuse bleeding and use two powdered topical absorbable hemostats with a good outcomes after six days of drainage. No case of bronchopleural fistula was noted.
The mean post-operative hospital stay was 7.9 days in our series. All the patients were followed radiographically and clinically during 1; 3; 6; and 12 months. The mean follow-up period was 21.5 ± 16.2 (range 6–73) months. Long-term outcomes were judged positive since no recurrence of the disease or other surgery-related complications were described during the 39 months of follow-up after surgery.
Discussion
Pulmonary destroyed lobe results from chronic pulmonary or recurrent inflammatory infectious diseases and is defined as an extensive destruction and irreversible damage of a part of lung parenchyma, with physiological consequences as decreased ventilation/perfusion ratio.
Hemoptysis, a frequent complication of destroyed lobe of the lung, is usually seen in tuberculosis cavities, bronchiectasis essentially in aspergilloma but in the others etiologies like hydatid cyst, necrotic pneumonia. The others symptoms: chronic cough; chest pain; purulent and persistent sputum are present with variable degrees and frequencies. The chronicity of symptoms is concluded from frequent medical visits and frequent hospitalization.3–6
The common causes of parenchymal destruction are particularly tuberculosis disease followed by bronchiectasis secondary to airflow obstruction, aspergilloma, lung abscesses, bronchial stenosis, congenital malformation, complicated hydatid cyst, and neglect foreign bodies.6–11 In our study, nonspecific bronchiectasis first and tuberculosis were the major causes of destroyed lung, these pathologies are still frequent in developing countries.1–3,12,13 Tuberculosis was the major causes of destroyed lung or lobe, which is consistent with many reports in the literature, 5 but other authors like in our work report non-specific causes: Halezeroglu et al., 3 and Sayir et al. 2
In the literature, we find that respiratory infections are associated with hypertrophy of the lymph nodes responsible of the compression of the bronchial tree lumen; the thickening of the bronchial wall responsible of the lumen narrowing decrease the progression of bronchial secretions with stagnation, infection, and parenchymal consequences as the pneumonia and destruction.2,14,15
The aim of early surgical treatment of lung lobe destroyed is to prevent fatal complications like massive hemoptysis and septicemia; reduce the risk of empyema and aspergillosis graft; avoid the installation of pulmonary hypertension and/or pulmonary systemic shunt, and to increase the patient’s quality of life.
Interventional embolization is an effective treatment for massive hemoptysis as a result of the destroyed lung lobe, but it is temporary with possibility of recurrence. 15
This technique was used in one patient with a severe hemoptysis (>750 ml) and surgery was realized 24 h after.
Lobectomy or more is the only treatment method that enables symptomatic patients with destroyed lung lobe despite all the surgical difficulties and potential complications. 5 The other indications of surgery is the possibilities of massive hemoptysis, recurrent infections, and multi-drug-resistant tuberculosis or extensive evolution of parenchyma destruction.3,5
In our study, one patient that developed massive hemoptysis was operated under emergency conditions and she had a tuberculosis-destroyed left upper lobe with aspergilloma graft.
Parenchymal resection of an inflammatory and infectious lung disease is regarded as a high-risk procedure because of the chronical lesions, state of patients, and technical difficulties, these circumstances were responsible for higher risk of post-operative complications.
Surgery of destroyed lobe of the lung was usually accompanied with high risks of complications like persistent air leakage, pulmonary infection, post-operative hemothorax, empyema, bronchopleural fistula, respiratory failure.
These frequent complications are explained by major technical difficulties associated with pulmonary resection: the anarchy and disorganization of the anatomical structures, the fibrous and sclerosis of pleural adhesions, the hilar fibrous thickening, lymph node incarceration and calcifications around the mediastinal structures (vascular and bronchia), responsible for changes in the anatomical location of the lung due to a mediastinal shift and difficulties of anatomical dissection with possibilities of massive bleeding. 3
The difficulties of dissection, bleeding, opened-cavities, and the length time of surgery are provider of recurrent infections.
Surgical resection of the destroyed lobe of the lung has been a great challenge in medical practice, mainly due to intraoperative blood loss, and frequent per operative opening of infected cavities responsible of the high incidence of post-operative infectious complications.
Some authors propose to realize, preoperative embolization in the preoperative preparation of surgery of the destroyed lung in the aim to reduce intraoperative blood loss and decrease surgical difficulty.
Anatomic lobectomies were performed on patients with destroyed lung lobe by the use of VATS, based on experience of surgeons in tuberculosis and inflammatory thoracic operations. However, in some conditions the conversion to a standard thoracotomy or an axillary operation with small incisions was imposed. 5
The principle factors of conversion are incompleteness of interlobar fissures, peribronchial lymph node calcification and pleural adhesions, and high fibrous thickening around the hilum.
The left side is more affected than the right side (in our series, the left lung was affected in 26 (81.2%) and the right lung in 6 (18.7%)). The reason for this difference is the narrowness and horizontality of the left main bronchus which may have an effect on the drainage of secretions.
Moreover, using an adequate closure technique for the bronchial stump and covered it by adjacent tissues decreases the risk of bronchopleural fistulas; persistent air leakage; and infection of the pleural cavity. There was no difference between manually bronchial stump closure using three rows of 3/0 polyglactin absorbable suture or using staplers.
Surgical morbidity and mortality for destroyed lobe of the lung is variable and depends absolutely on the etiology:
In inflammatory lung, diseases have been reported between 4 and 8.5%.
12
In tuberculosis and sequelae, Huang et al. reported 21.4% of complications after anatomic lobectomy by VATS.
5
In aspergilloma, the reported rate of mortality after pulmonary aspergilloma surgery varies from 5% to 10% and these rates increased in the group with complex aspergilloma.8,9 The rate of post-operative complications of aspergilloma ranges from 25% to 70%.8–10
The chronic suppurative diseases such as bronchiectasis and tuberculosis affect the quality of life of the patients but the very important problem is the life-threatening complications including massive hemoptysis, graft fungal infections, septicemia, empyema, and pulmonary–systemic shunting.2,3 Preoperative embolization may reduce intraoperative blood loss and surgical difficulty.16
Ruan et al. 17 treating tuberculosis destroyed lung (34 lobectomy and 79 pneumonectomy) identified independent risk factors (male gender and age ≥40 years old) as predictive of severe post-operative complications. They emphasize that special attention should be paid in case associated with chronic pulmonary aspergillosis (CPA) to avoid a poor outcome (23.3% of severe complications vs. 8.4% without CPA).
The limitations of our study are the retrospective character and selection of patients with good general state and no contra-indication of general anesthesia.
Conclusion
The post-operative complications after pulmonary resection of destroyed lung depend essentially on the etiology of the parenchymal destruction. The insufficient antibiotic use and inadequate follow-up in patients with tuberculosis and lung infections are frequent causes of destroyed lung but in the last years, it has been decreasing steadily because of the early diagnosis.
Footnotes
Acknowledgement
The authors thank Yassine Amara MD for English language edition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.