
Abstract
Background
The aim of this study is to analyze the clinical outcomes of triple valve repair for rheumatic heart disease in terms of both early results and long-term benefits.
Methods
Between January 2008 and December 2016, all the patients who underwent triple valve repair for rheumatic heart disease were included in this study.
Results
Thirty-eight patients underwent triple valve repair procedure for rheumatic heart disease at our institute. Mean age was 33 years; 60.5% were females. Techniques used to achieve mitral valve repair were: commisurotomy (n = 26), prosthetic ring annuloplasty (n = 9), posterior teflon annuloplasty (n = 23), leaflet shaving (n = 14), implantation of neochordae (n = 5) and pericardial patch augmentation of mitral valve leaflets (n = 6). For aortic valve repair, the techniques used were: commisurotomy (n = 23), leaflet shaving (n = 16), pericardial patch augmentation (n = 3), subcommisural plication (n = 10), free margin plication (n = 2) and free margin resuspension (n = 1). Tricuspid valve repair was performed using modified Devega's technique (n = 32), commisurotomy (n = 9) and posterior annular plication (bicuspidization) (n = 5). The operative mortality was 0%. There was no primary repair failure. Estimated survival at the end of 1 year, 5 years and 10 years was 100%, 91.6% and 65.8%, respectively. Overall freedom from reintervention at 1, 5 and 10 years was 100%, 96.4% and 61.4, respectively.
Conclusion
Triple valve repair provided satisfactory early and long-term results in this challenging subset of patients and can be considered as an acceptable option for significant triple valve disease due to the absence of anticoagulation-related events.
Introduction
Diseases of the heart valves constitute a major cause of disability, reduced quality of life and premature mortality from cardiovascular diseases worldwide. In developing countries, rheumatic fever remains the leading cause of heart disease in children and young adults. 1 The age of presentation is much earlier than the western world, and severity of symptoms are more pronounced at an earlier age. 2 It has long been known that advanced rheumatic heart disease may affect multiple valves and undermine myocardial function severely. Clinically significant valvular heart disease involving mitral, aortic and tricuspid valves simultaneously usually presents with advanced heart failure, and it is recommended that all three valvular lesions be surgically corrected. Despite advances in cardiac surgery, triple valve surgery (TVS) is associated with an increased risk of operative mortality and thus remains a surgical challenge.3,4 Improvements in myocardial protection, operative techniques and expertise, and postoperative care have resulted in improved early and late outcomes over the last decade. 5 Furthermore, they are often subjected to long duration of cardiopulmonary bypass (CPB) and prolonged myocardial ischemia. In the modern era of cardiac surgery, contemporary reports in literature have demonstrated a reduction in operative mortality that ranges between 3 and 16%3–5; in spite of this, triple-valve procedures have been performed less frequently in recent years. Also, whether to repair or replace the valves remains controversial. The need for preventing the risks of long-term anticoagulation and experience of the operating surgeon also factor into the surgical decision. Bioprostheses are not an ideal substitute in the young. Mitral and tricuspid valve lesions are usually amendable for repair surgery but repairing the aortic valve with mitral and tricuspid valves is a surgical challenge. Very few studies report the results of triple valve repair procedure for rheumatic heart disease.6,7 The aim of this study is to analyze the clinical outcomes of triple valve repair for rheumatic heart disease in terms of both early results and long-term benefits.
Materials and methods
Study design
The present study is a retrospective single-centre study that includes patients who presented with clinically significant valvular heart disease involving mitral, aortic and tricuspid valves simultaneously (triple valve disease) and had all the three valves repaired with the etiology being rheumatic heart disease. The decision to repair all the three valves was taken based on preoperative echocardiography parameters. This study was approved by our institutional Ethics Committee (NHH/AEC-CL-2020-445). Patients’ demographic, operative and postoperative data were recorded in our institutional database and were extracted and evaluated. Postoperative outcomes were tracked from the database and by active follow-up after obtaining verbal consent from the patient.
The primary end point was a composite of successful valve repair with early and late mortality, freedom from reintervention and freedom from severe residual valvular lesion. Early mortality was defined as all-cause mortality at 30 days. 8 Late mortality was defined as all-cause mortality after 30 days of surgery. Secondary end points were postoperative incidence of major adverse cardiac and cerebrovascular events and were defined as any of the following complications: postoperative bleeding requiring reexploration, prolonged mechanical ventilation (>48 h), tracheostomy, postoperative stroke, need for a permanent pacemaker and new onset hemodialysis. During follow-up, the current patient status and functional class were noted.
Surgical technique
All operations were carried out with CPB with ascending aorta and bicaval cannulation. At 30°C, cardiac arrest was induced and maintained with antegrade cold blood cardioplegia solution. Mitral valve was approached through a left atriotomy in all cases. A careful segmental analysis was done to assess and confirm the valvular lesion and pathology. Mitral valve lesions were repaired first, followed by aortic valve and lastly tricuspid valve. All tricuspid valve corrections were carried under cardioplegic arrest. Modified Devega's repair for tricuspid valve was achieved using a single polypropylene suture from the anteroseptal to the posteroseptal commissure with a pledget placed between each entry site into the annulus. Techniques of individual valve repair were decided depending upon the pathology. All the patients were assessed with intra-operative transesophageal echocardiograms (TEE) after weaning off CPB.
Statistical analysis
Statistical analyses were performed with SPSS software (version 22.0., IBM Corp., Armonk, NY, USA). Continuous variables were described as mean and variation of each observation from the mean value (standard deviation) represented as mean ± SD or median and interquartile range if they failed to follow a normal distribution. Categorical variables were described by taking percentages. Survival analysis was done using Kaplan–Meier. Multivariable analysis with Cox regression method was done to identify independent factors for survival.
Results
Baseline characteristics
Patient baseline and preoperative data are summarized in Table 1. Between January 2008 and December 2016, a total of 3930 patients were operated for rheumatic heart disease. Amongst these patients, 238 patients underwent triple valve surgery. Amongst these, only 38 patients underwent triple valve repair procedure for rheumatic heart disease at our institute. There were 15 males and 23 females, ages ranged from 8 and 64 years (mean age 33 ± 15 years). Twenty-one patients were in New York Heart Association (NYHA) class 2, 15 patients in NYHA class 3 and 2 patients were in NYHA class 4. Eighteen patients were in atrial fibrillation at the time of the surgery.
Baseline characteristics.
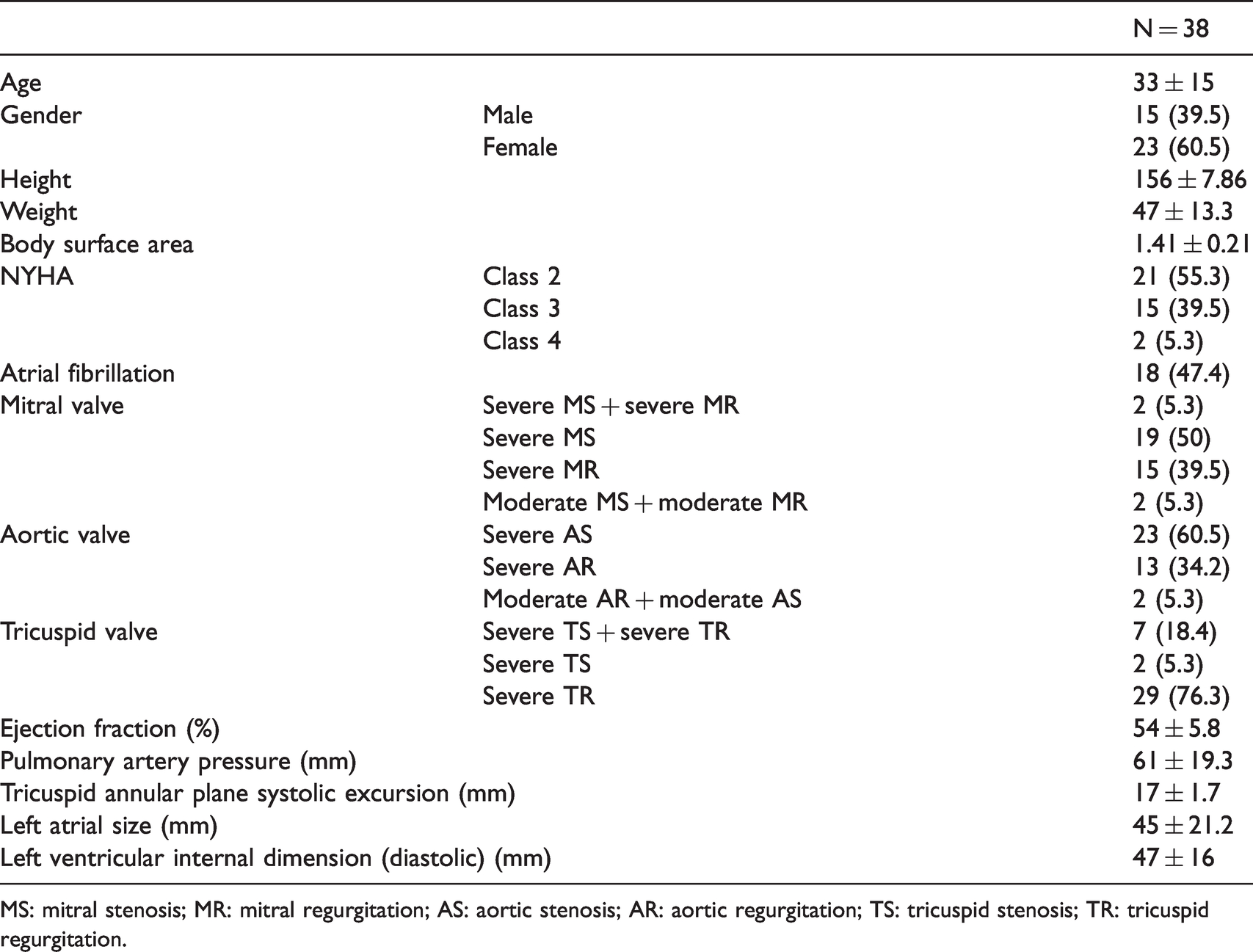
MS: mitral stenosis; MR: mitral regurgitation; AS: aortic stenosis; AR: aortic regurgitation; TS: tricuspid stenosis; TR: tricuspid regurgitation.
Echocardiograms
All patients had TTE at our institute to determine the type and severity of valve disease. Triple valve disease was confirmed in all patients. Mean ejection fraction, pulmonary artery pressure, tricuspid annular plane systolic excursion (TAPSE) were 54%, 61 mm, 17 mm, respectively, with a mean left atrial size and left ventricular diastolic internal dimension of 45 mm and 47 mm, respectively (Table 1).
Mitral valve diseases
Nineteen patients had severe mitral stenosis (MS). Fifteen patients had severe mitral regurgitation (MR), two patients had a combination of severe MS with severe MR and two had moderate mitral stenosis with moderate MR.
Aortic valve diseases
Twenty-three patients had severe aortic stenosis (AS) and 13 patients had aortic regurgitation (AR) and two patients had moderate aortic stenosis and moderate AR.
Tricuspid valve diseases
Twenty-nine patients had severe tricuspid regurgitation (TR), two patients had severe tricuspid stenosis, whereas seven patients had a combination of severe TR and severe tricuspid stenosis.
Operative details
The operative procedures are summarized in Table 2. Techniques used to achieve mitral valve repair were: commisurotomy in 26 patients, prosthetic mitral ring annuloplasty in 9 patients (Carpentier-Edwards Classic annuloplasty ring, Edwards Lifesciences, Irvine, CA, USA), only posterior teflon annuloplasty in 23 patients (where the valve was extensively thickened due to rheumatic heart disease or in patients with high suspicion of developing post repair systolic anterior motion), leaflet shaving in 14 patients, implantation of neochordae in 5 patients using Gore-Tex® sutures (W. L. Gore & Associates, Inc., Newark, DE, USA) and pericardial patch augmentation of mitral valve leaflets in 6 patients.
Intra-operative details.
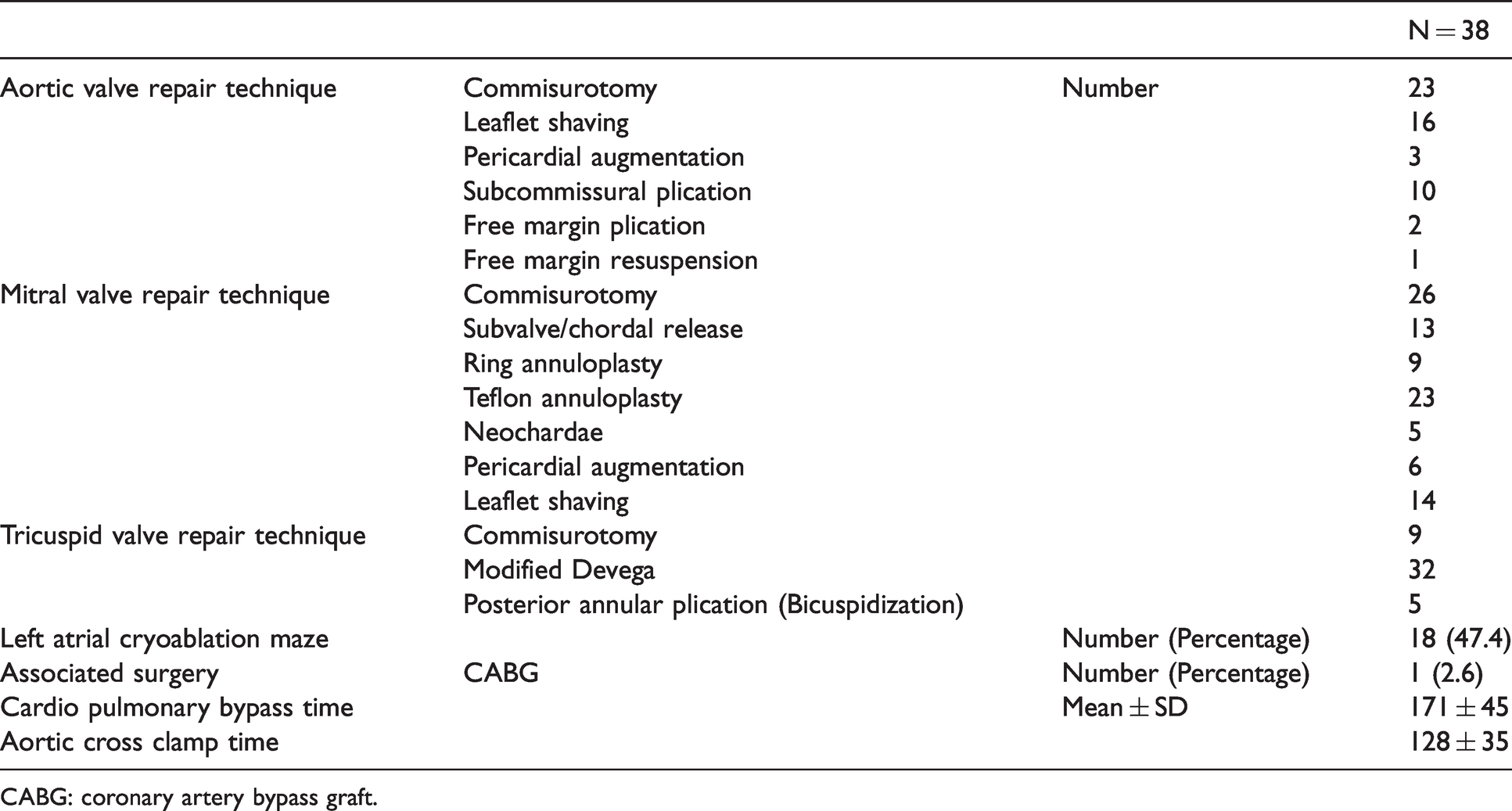
CABG: coronary artery bypass graft.
For aortic valve repair, the techniques used were: commisurotomy in 23 patients, leaflet shaving in 16 patients, pericardial patch augmentation in 3 patients, subcommisural plication in 10 patients, free margin plication in 2 patients and free margin resuspension in 1 patient. For aortic stenosis, commisurotomy and leaflet shaving were done commonly.
For tricuspid valve repair, inspection of the heart showed evidence of TR such as right atrial and ventricular dilation. Our preferred approach is the classic horizontal atriotomy. The tricuspid valvular apparatus was carefully inspected. The severity of tricuspid annular dilatation was assessed. The tricuspid valve leaflets were examined for any evidence of pathology. Tricuspid valve repair was performed using modified Devega's technique as described by in 32 patients, commisurotomy in 9 patients and posterior leaflet plication resulting in bicuspidization in 5 patients.
Mean CPB times and mean aortic cross clamp times were 171 and 128 min, respectively. Regarding the rhythm surgery, all 18 patients who were in atrial fibrillation at the time of the surgery underwent left atrial cryoablation maze. One patient underwent coronary artery bypass grafting as a concomitant procedure.
Postoperative outcomes
After weaning off CPB, on TEE assessment, all patients had either trivial or mild valvular insufficiency.
Mortality
There was no early all-cause mortality.
Morbidity
Postoperative outcomes are summarized in Table 3. Postoperative complications included prolonged ventilation (eight patients), pericardial drainage one week after surgery for effusion (one patient). Median ICU duration was four days (Table 3). Median postoperative hospital stay was 11 days. No patients had postoperative bleeding requiring reexploration, stroke or new onset hemodialysis or tracheostomy. Postoperatively, only 4 out of the 18 patients who underwent rhythm surgery remained in atrial fibrillation. Patients who underwent rhythm surgery were started on oral anticoagulation for three months if they reverted back to sinus. For the patients who remained in atrial fibrillation after rhythm surgery, oral anticoagulation was continued lifelong, maintaining INR between 1.8 and 2.2.
Postoperative details.
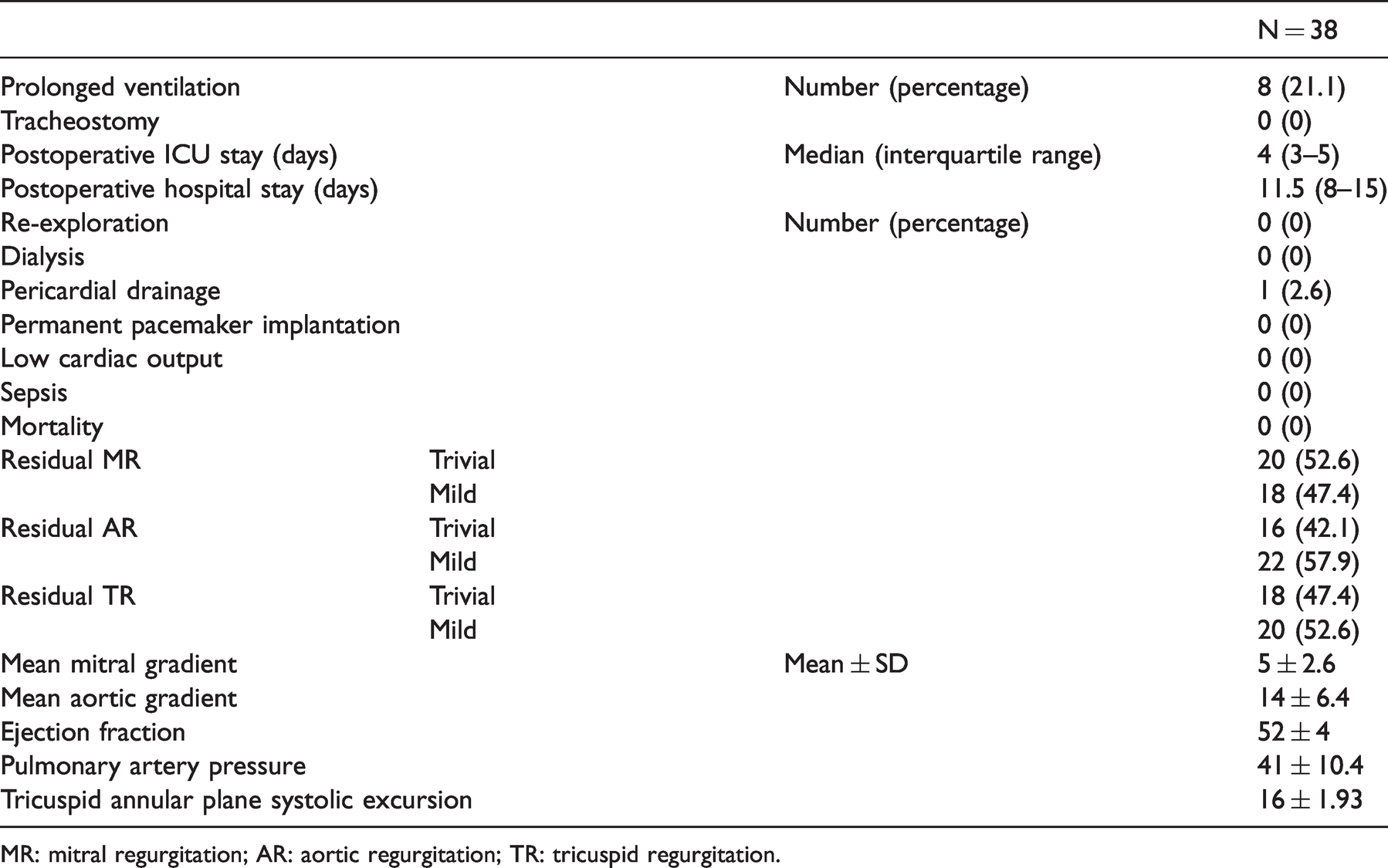
MR: mitral regurgitation; AR: aortic regurgitation; TR: tricuspid regurgitation.
Echocardiograms
All patients underwent TTE before discharge. Mean ejection fraction, pulmonary artery pressures and TAPSE were 52%, 41 mm Hg and 16 mm, respectively. Residual MR was trivial and mild in 20 and 18 patients, respectively; residual AR was trivial and mild in 16 and 22 patients, respectively. Residual TR was trivial and mild in 18 and 20 patients, respectively. Postoperatively, mean gradients across the aortic and mitral valves were 14 mmHg and 5 mm Hg, respectively.
Follow-up
Follow-up data were available in 34 patients out of the 38 patients discharged (89%) with a mean of 72 months (range 2–144 months). During follow-up, 6 patients had a late mortality at a mean duration of 89 months after the primary operation. Four were valve related mortalities and two were due to non-cardiac reasons. Out of the four valve-related mortalities, three had sudden unexplained death, one died in the immediate postoperative period of the redo valvular surgery due to low cardiac output. Estimated survival at the end of 1 year, 5 years and 10 years was 100%, 91.6% ± 5.8 and 65.8% ± 13.5, respectively (Figure 1(a)). CPB time (p = 0.04), aortic cross clamp time (p = 0.022) were identified as factors predicting late mortality on univariable analysis; however, on multivariable analysis using cox regression, none were identified as independent factors affecting late mortality. Out of four patients who remained in atrial fibrillation after rhythm surgery, three continued to be in atrial fibrillation during the follow-up period. In addition to it, there were five more patients in new onset atrial fibrillation.
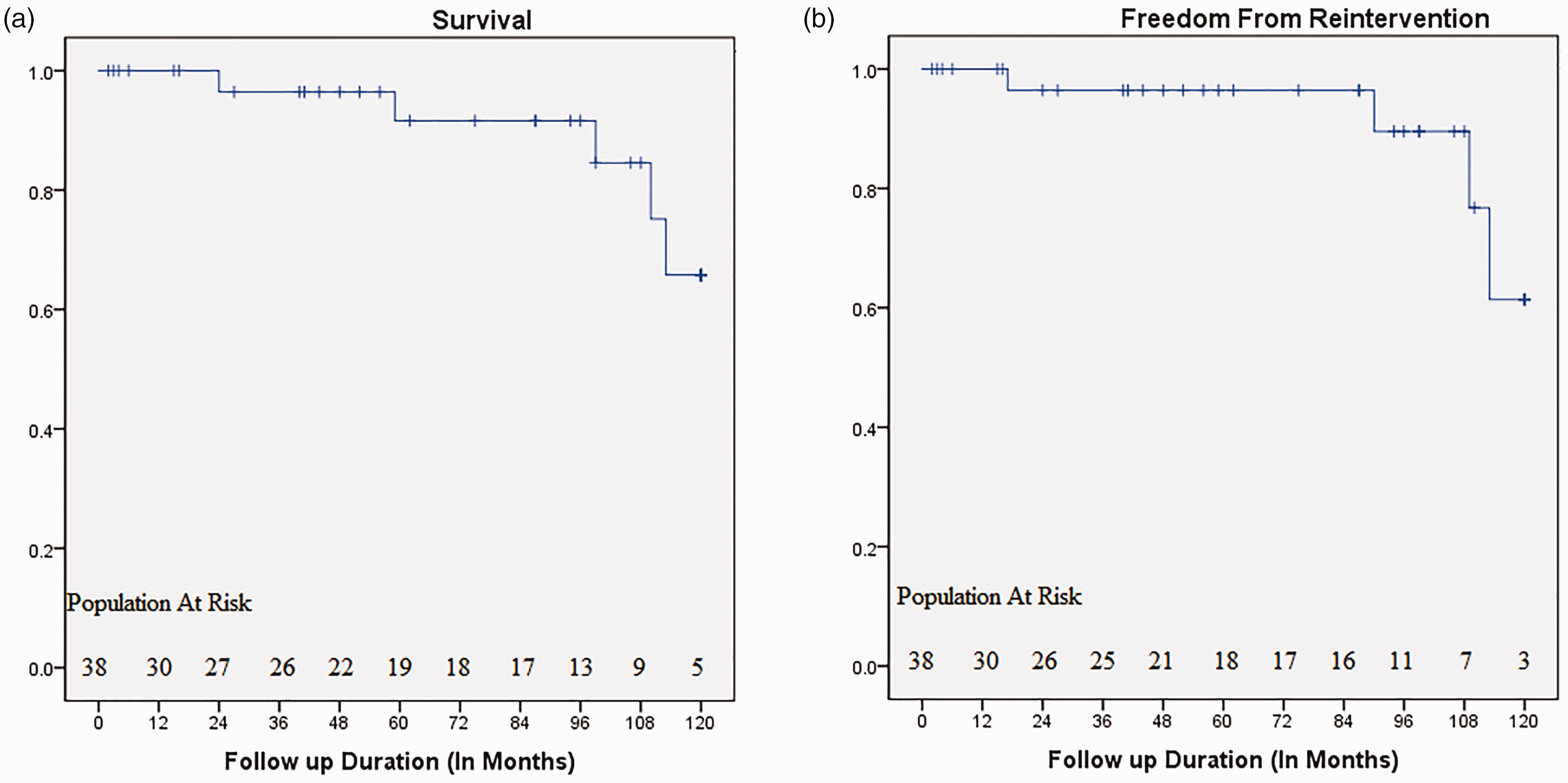
(a). Long-term survival in patients undergoing triple valve repair surgery and (b) long-term freedom from reintervention in patients undergoing triple valve repair surgery.
Reintervention
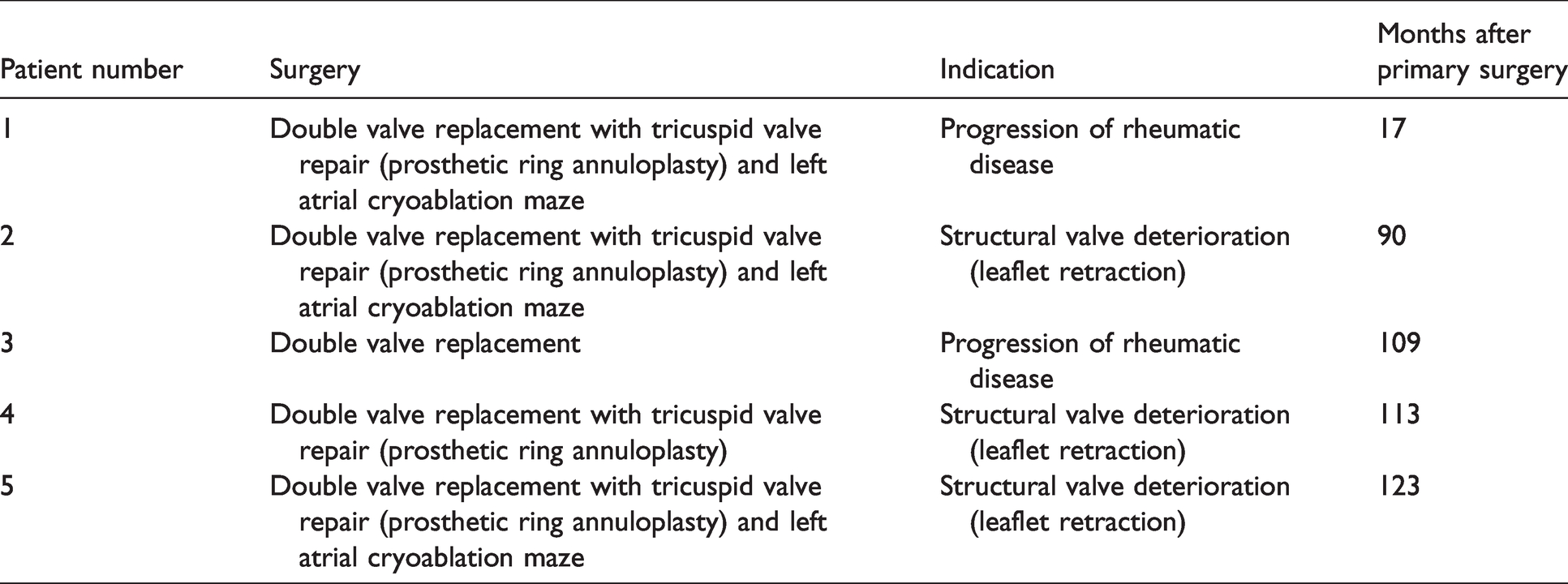
Five patients underwent a reintervention during the follow-up period at a mean duration of 90.4 months after the primary surgery. Four patients amongst them underwent replacement of aortic and mitral valves and tricuspid valve repair (using prosthetic ring annuloplasty). Details of the redo surgeries are given in Table 4. Overall freedom from reintervention at 1, 5 and 10 years was 100%, 96.4% ± 3.5 and 61.4 ± 17.4, respectively (Figure 1(b)).
Follow-up details.
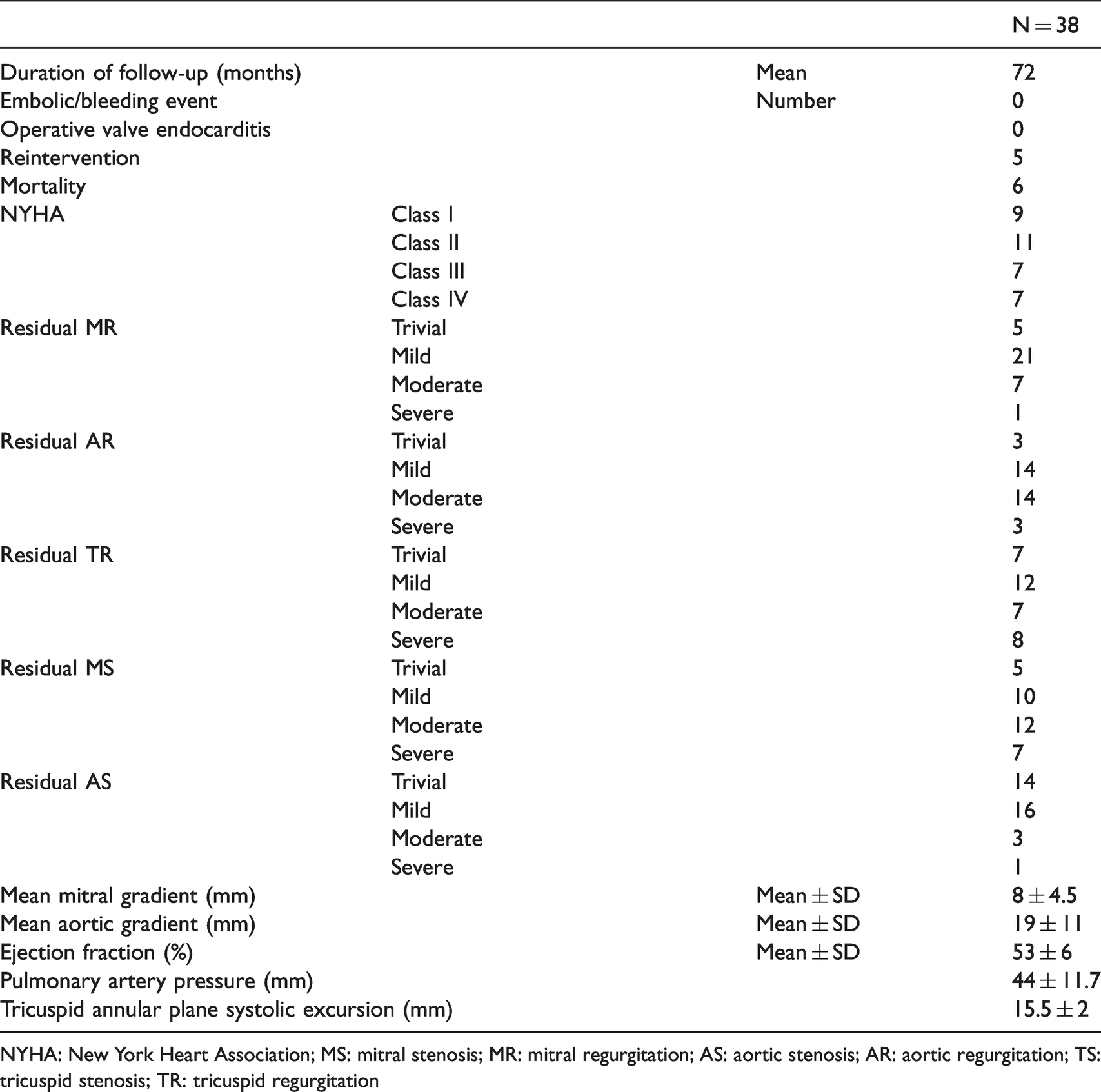
NYHA: New York Heart Association; MS: mitral stenosis; MR: mitral regurgitation; AS: aortic stenosis; AR: aortic regurgitation; TS: tricuspid stenosis; TR: tricuspid regurgitation
Clinical status
No patients experienced an embolic/bleeding event or operated valve endocarditis during the follow-up. Seven patients were in NYHA class IV (including five which were reoperated), seven patients were in NYHA class III, remaining patients were in class I or II at the time of follow-up.
Echocardiograms
The echocardiogram data were available for all 34 patients. Details about the reintervention in all the three valves are given in Table 5. Apart from the five patients who were reoperated, eight more patients had either one or more severe residual valvular lesion due to progression of rheumatic disease as examined on transthoracic echocardiography at 24, 27, 41, 52, 75, 94, 99 and 120 months after primary operation (mean = 66.5 months). These patients have been advised reoperation depending on the severity of the residual valvular lesion; however, they have not undergone the same due to cost constraints. Among all the severe residual valvular lesions, freedom from severe residual MR, severe residual MS, severe residual AR, severe residual AS and severe residual TR at 10 years was 100%,74.8%, 87.5%, 85.7% and 60.5%, respectively (Figures 2(a), (b) and 3(a), (b)).
Reintervention details.
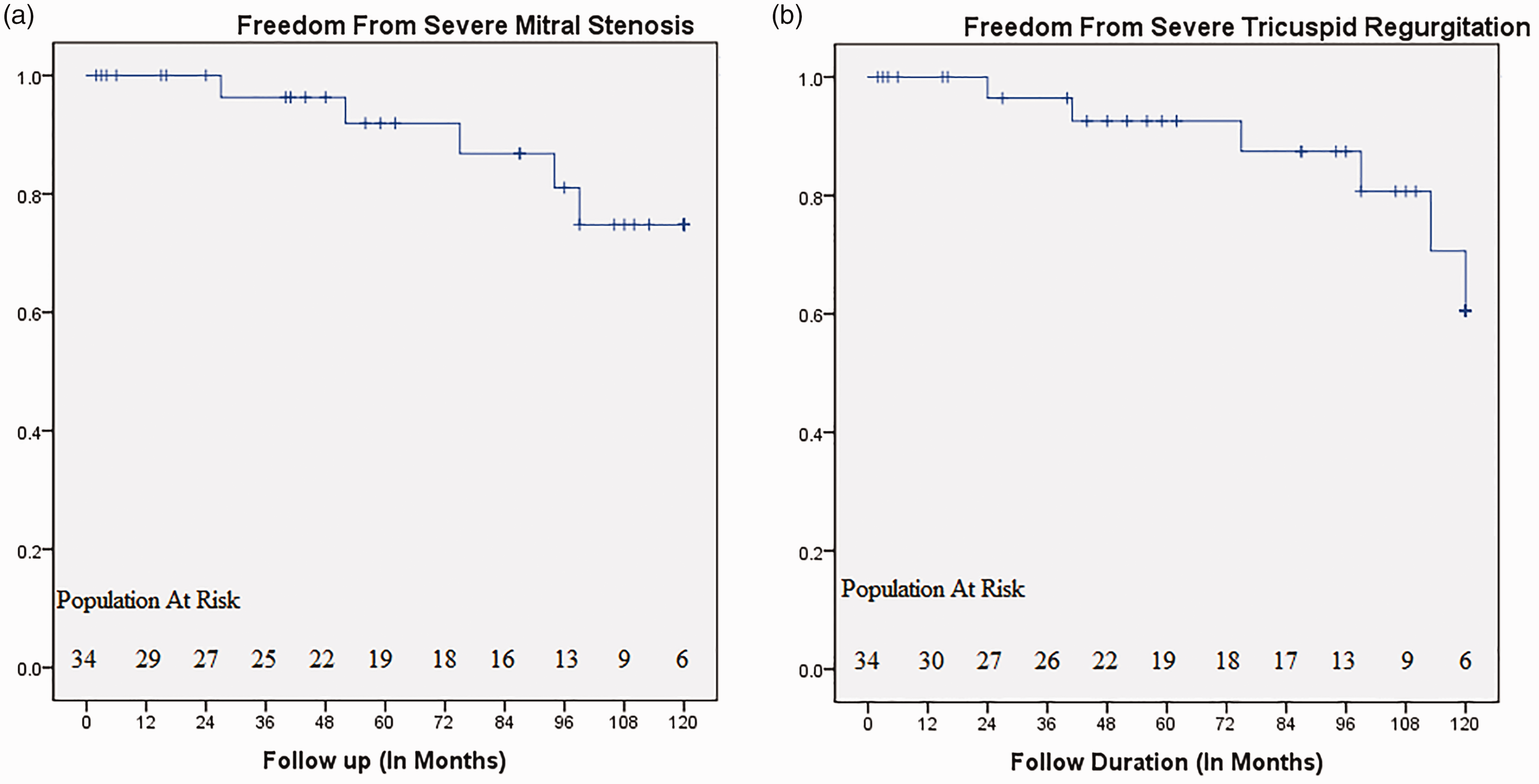
(a) Freedom from severe mitral stenosis and (b) freedom from severe tricuspid regurgitation.
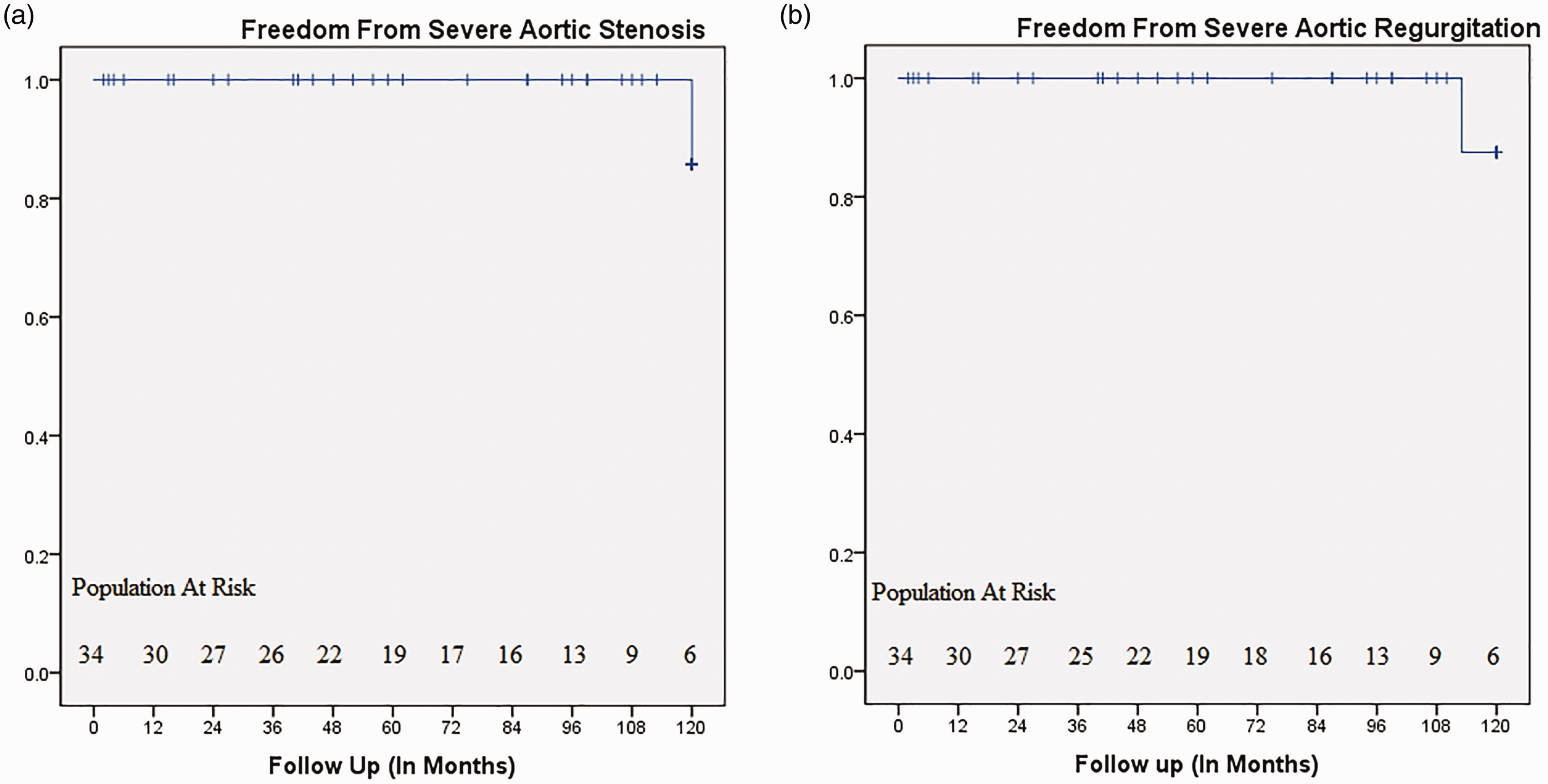
(a) Freedom from severe aortic stenosis and (b) freedom from severe aortic regurgitation.
Discussion
Triple valve surgery, including aortic, mitral and tricuspid valves procedures, still remains a challenge for cardiac surgeons in terms of both early and late mortality. Majority of the existing literature on triple valve surgery consists of valve replacements either single or multiple. The reported in hospital mortality of triple valve surgery in recent literature ranges between 2.5 and 20%.9–14 Usual concerns associated with valve replacements continue to have a significant impact on the quality of life of the patients due to risk of anticoagulation-related adverse events. Thus, a strong consideration must be given to offer triple valve repair to patients with advanced triple valve disease with an advantage of avoidance of anticoagulation and better preservation of ventricular function. Even though there are studies on outcomes of mitral and tricuspid valve repairs with aortic valve replacement for triple valve disease, 12 we have found very few studies looking at triple valve repair as a feasible option. 6 The aim of our study was to describe the experience with patients who underwent triple valve repair at our institute in an attempt to assess the early and late mortality, freedom from reoperation and freedom from severe residual valvular lesions. (Figure 3(a) and (b))
In Grinda series for triple valve repair for young rheumatic patients, operative mortality was 4.7%. 6 They reported no late mortalities with a mean follow-up of 51 months and only 2 patients (10%) underwent redo valvular replacements at 14 and 32 months after the primary operation. In our study, we did not encounter any early mortalities, and the estimated survival at 1, 5 and 10 years was 100%, 91.6% ± 5.8 and 65.8% ± 13.5, respectively. Overall freedom from reintervention at 1, 5 and 10 years was 100%, 96.4% ± 3.5 and 61.4 ± 17.4, respectively. Out of 34 patients who were followed up, 15 patients had either a reintervention/late mortality or any severe residual valvular lesion with range of 2–144 months (mean of 72 months), whereas 19 patients experienced complete success without any of the above complications. On univariate analysis, aortic cross clamp time (p = 0.047) and postoperative pulmonary artery pressure (p = 0.008) were significant for predicting a complete success for the patients; however, on multivariable analysis using cox regression, none were identified as independent factors affecting complete success. In our series all the patients who underwent rhythm surgery, we performed only left atrial maze as it has shown to decrease the aortic cross clamp time; however, there is no significant difference between biatrial and left atrial maze in terms of conversion to sinus rhythm. 15 In addition to it, our finding that aortic cross clamp time was one of the significant factor predicting complete success for triple valve repair surgery in the long term, corroborates with our decision to perform only left atrial maze instead of biatrial maze.
Noack et al. 12 reported a 30-day mortality 16.1% with one-year and five-year survival of 71.8% and 54.6%, respectively, for triple valve surgery. They identified preoperative NYHA functional class IV, pre-op renal failure on hemodialysis, previous liver dysfunction, previous myocardial infarction and age as predictors for late mortality. In our study, CPB time (p = 0.04), aortic cross clamp time (p = 0.022) were identified as factors predicting late mortality on univariate analysis. Other studies have reported a five-year survival between 55 and 87%3,5,9,12–14,16,17 following triple valve surgery, involving either single or multiple valvular replacements. Lio et al. 13 reported 10-year rates of freedom from thromboembolism and anticoagulation-related haemorrhage as 88% ± 5 and 88% ± 4, respectively. Our results both early and late are comparable to the studies who have reported triple valve surgery using valvular replacements.
In our experience, we decide to repair the valves where anticoagulation needs to be avoided. For mitral valves, we prefer to repair whenever the anterior mitral leaflet is pliable and not severely calcified. We repair the aortic valve if the leaflet mobility is relatively preserved and calcification extent is less than one third of the leaflet area, as in cases of extensive calcification, we have seen poor longevity of aortic valve repair. Moreover, in cases of aortic stenosis, it is more feasible to perform a valvotomy. Tricuspid valve is usually repaired, as anticoagulation requirement is very high for tricuspid valve replacement and tricuspid valve repair has been known to be an acceptable surgical option.
Regarding significant residual lesion, we observed that mitral valve lesions were more common at 10-year follow-up as compared to aortic valve lesions due to the progression of rheumatic disease. Freedom from severe residual TR was only 60.5% at 10 years due to use of Modified Devega's technique and bicuspidization, used due to cost constraints. Tricuspid valve repair without ring annuloplasty has shown to have a higher recurrence of severe TR compared to ring annuloplasty. 18
Significant triple valve disease is still fairly common in developing countries due to rheumatic heart disease. Despite improvements in myocardial protection and postoperative management of patients, triple valve surgery remains a challenge in terms of surgical expertise involved when all the three valves are to be repaired. The authors would like to convey that in a resource limited clinical setup, valve repair surgery would be significantly cheaper as compared to valve replacement (both single and multiple valvular) not just in the short term but also in the long term. Multiple factors contribute to the increased cost of valve replacement surgery in the long term. It is not only due to less patient compliance to anticoagulation monitoring (both due to cost and lack of accurate testing centers in the remote areas of the country) but also due to anticoagulation-related adverse effects requiring hospital readmission and/or reintervention. Whereas, the valve repair patients would be free from anticoagulation and its attendant events; hence, its additional costs would be significantly less. The cost and risk of performing redo valvular surgery haves decreased as compared to previous years hence valve repair (either single or multiple) can be contemplated as a satisfactory option in terms of efficacy, cost and better quality of life in experienced centers.
Limitations
This was a retrospective study and is associated with all its limitations of this type of study. We could follow-up only in 89% of the patients discharged in spite of our best efforts. The reason being we cater to patients from different geographical locations across the Indian subcontinent where they lack access to basic forms of communication and cannot do regular follow-up due cost constraints and they seek medical attention only during severe discomfort.
Conclusion
The triple valve repair for aortic, mitral and tricuspid valves is a good alternative to valve replacement in selective subset of patients of rheumatic heart disease where durable valve function can be achieved with satisfactory early and late outcomes in terms of mortality, freedom from reintervention. Additionally, it avoids anticoagulation and its attendant effects.
Footnotes
Authors’ note
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by our institutional Ethics Committee (NHH/AEC-CL-2020-445).
Informed consent
Verbal informed consent was obtained from all participants.