
Abstract
Background
To maintain the patency and longevity of arteriovenous fistula, the availability of a venous segment with adequate diameter is important. In Indian population, many chronic kidney disease patients have poor caliber veins. The study aimed to evaluate the efficacy of hydrostatic dilatation versus Primary balloon angioplasty of small caliber cephalic veins of (≤2.5 mm) preoperatively in terms of patency rate and maturation time of arteriovenous fistula.
Methods
Patients (n = 80) with an end-stage renal disease requiring arteriovenous access surgery for hemodialysis with small caliber cephalic veins were randomized into two groups, i.e., hydrostatic dilatation and primary balloon angioplasty, each with 40 patients. All patients underwent a thorough clinical examination as well as duplex ultrasound vein mapping of both upper extremities. Patients were followed up for six months and primary patency, maturation time, and complications were noted.
Results
Immediate technical success with good palpable thrill was achieved in 97.5% of patients in the primary balloon angioplasty group and 87.5% in the hydrostatic dilatation group. The fistula maturation time in the primary balloon angioplasty group was 34.41 days and 46.18 days in the hydrostatic dilatation group. In the primary balloon angioplasty group, the primary patency of the fistula was 97.5% and 87.5% in the hydrostatic dilatation group, at six months. The arteriovenous fistula functioning rate was 77.5% in the hydrostatic dilatation group as compared to 92.5% in the primary balloon angioplasty group at six months. The incidence of surgical site infection was 5% in the primary balloon angioplasty group as compared to 10% in the hydrostatic dilatation group.
Conclusion
Primary balloon angioplasty of small caliber cephalic veins (≤2.5 mm) performed prior to arteriovenous fistula creation for hemodialysis is a beneficial procedure.
Introduction
Chronic kidney disease (CKD) is a global public health concern, with rising incidence and prevalence. Mortality due to CKD showed an increasing trend between 2005 and 2015 by 32% with up to 1.2 million deaths worldwide. 1 Vascular access patency and adequate hemodialysis are essential for the optimal management of patients with stage V CKD. Surgically created arteriovenous fistula (AVF) is a commonly practiced procedure among the available types of access creation. Studies have demonstrated that native fistula access has good patency rates (4–5 years) and needs fewer re-interventions when compared to other access types. 2 Moreover, it improves the patient survival and quality of life and reduces morbidity and mortality. 3
To achieve a successful fistula, the duplex ultrasound (DUS) study plays a crucial role in the evaluation of both arterial and venous systems of the upper limb. DUS is the most preferred preoperative vascular mapping method that is not only cost-effective but also has patient compliance.4–7 It has been reported that physical examination along with preoperative ultrasound mapping significantly improves the short-term patency and the suitability of AVF for dialysis. Another important factor responsible for vascular access patency is the vein size. 8 Threshold of >2.5 mm vein diameter is required for successful AVF creation. Research has reported that radiocephalic AVF and brachiocephalic AVF have 66%, and 81% maturation rates, respectively. Hence, both vein size and type of fistula significantly affect the maturation. 9
Techniques such as balloon-assisted maturation, venous angioplasty, access vein/central vein stenting, fistula superficialization, venous branch ligation, interposition of vein grafts, transposition, and extensive preoperative imaging have been developed to improve the patency of fistula.9,10 However, the patency of the fistula still remains low as these measures aid in the functioning of the fistula and do not focus on increasing the vein utilization at the time of fistula creation. 11 Hence, there is a greater need for creating successful arteriovenous (AV) access from a cephalic vein with a smaller caliber. The present study thus intended to evaluate and compare the efficacy of primary balloon angioplasty (PBA) of cephalic veins with a diameter less than or equal to 2.5 mm for hemodialysis as compared with standard hydrostatic dilation (HD) technique in terms of maturation time and patency of autogenous brachiocephalic AVF.
Methods
The present one-year longitudinal study (2015–2016) was conducted at the Department of Vascular and Endovascular Surgery on patients (n = 80) admitted with a diagnosis of end-stage renal disease (ESRD) requiring hemodialysis. Ethical approval was obtained from the Institutional Ethical Review Board of M.S. Ramaiah Medical College and Hospitals (ECR/215/Inst/Ker/2013) before commencing the study. The procedure of the study was instructed to the patients and a written informed consent was also obtained.
Inclusion Criteria: ESRD patients requiring hemodialysis with
Normal Brachial artery on DUS(with a minimum diameter of 3.5 to 4 mm and without any atherosclerotic plaques) Cephalic vein at cubital fossa less than 2.5 mm Patients willing for the procedure after counseling about poor caliber veins Segmental cephalic vein occlusion Central vein stenosis or occlusion Extensive brachial artery disease on duplex ultrasonography Difference of BP of 10 mm Hg or more between the upper limbs
Exclusion Criteria: ESRD patients requiring hemodialysis with
The patients were randomized based on a closed envelope system and allocated into the two study groups based on the technique (HD vs PBA).
The patients’ demographic details and data regarding associated comorbid illnesses and previous history of fistula creation were elicited via a predesigned questionnaire. Preoperatively, all patients were subjected to complete physical examination and DUS. Parameters evaluated by DUS included diameter, blood flow pattern, and patency of the brachial arteries. Cephalic veins were evaluated for augmentation with distal compression, diameter, patency, and depth. The non-dominant upper limb was preferred to measure vein diameter by DUS with a tourniquet and inner wall to inner wall diameter using the B-mode technique.
The cephalic vein and the brachial artery on the planned side were dissected and about 5 cm of the cephalic vein was isolated at the elbow (Figure 1(a)). The vein was then dilated with a 20-ml sterile heparinized saline solution injection. Later, segmental HD was done at 5, 10, 15 cm (Figure 1(b)). Similarly, in the PBA group, after isolating cephalic vein, balloon with guidewire of 0.018 inches was inserted up to the upper arm under direct palpation and DUS guidance through the cephalic vein. Dilatation was done with a balloon of one size higher and length 150 mm inflated for 60 s with a pressure of 10 mm under USG guidance (Figure 1(c) and (d)). In both groups, the technique anastomosis was performed end to side, cephalic vein to brachial artery with 6–0 polypropylene suture. Surgical site infections (SSI) observed were also recorded. As a standard protocol, all patients were given 75 mg of aspirin tablet daily for six months after the procedure. Follow-up appointments with the surgeon were scheduled after the creation of the AVF (Figure 1(e)) on post-operative day 1, week 2, week 6, month 3, and month 6 during dialysis visits or via telephonic conversation (up to 6 weeks in-person consultation in opd and post 6 weeks of the procedure, the patient underwent hemodialysis via AVF. This was followed by telephonic consultation or consultation during HD visits; assessment via the adequacy of hemodialysis, time taken for hemostasis from puncture site after the needle is removed and the duration of hemodialysis and pressures in the AVF during HD). The patency (primary end-point - interval from time of access placement to any intervention designed to maintain or re-establish patency or to access thrombosis or the time of measurement of patency) of the AV access was evaluated at each follow-up. The maturation status of vein (AVF which can be cannulated, 6 mm diameter of the access and a flow rate of minimum 350–500 ml/min, and usual time of 6 weeks to mature) and rate of functioning AVF (secondary end-points - access that is able to deliver a flow rate of 350 to 500 ml/min without recirculation for the total duration of dialysis) were recorded once a week in the proforma.
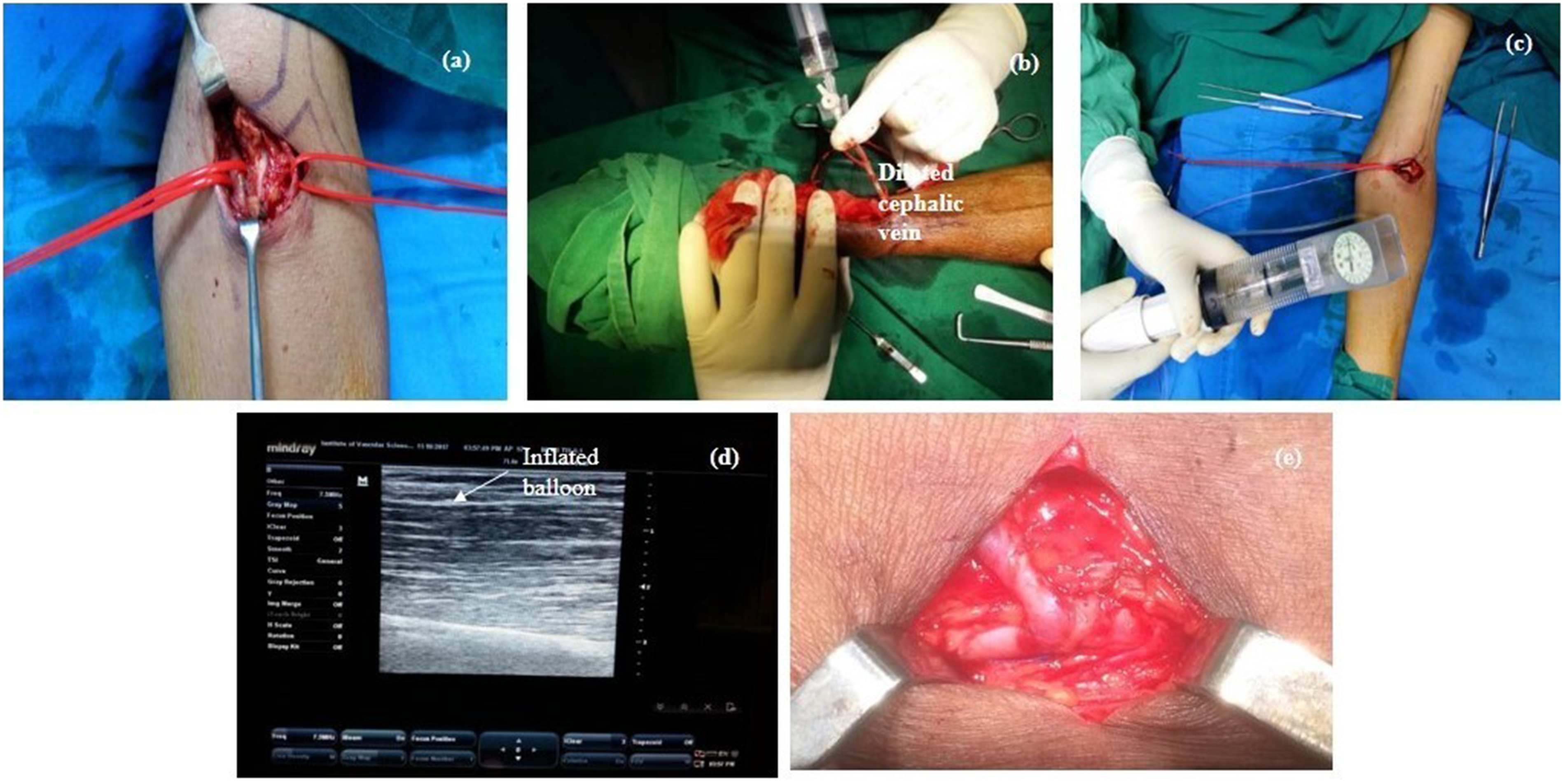
Arteriovenous fistula creation: hydrostatic dilatation and primary balloon angioplasty (a) exposed brachial artery and cephalic vein intraoperative photograph of hydrostatic, (b) dilatation of the vein done with 20G IV cannula inside the vein, (c) primary balloon angioplasty of cephalic vein, (d) inflated balloon seen in Doppler scan, and (e) completed arteriovenous fistula in the elbow.
The patency of AV access was evaluated clinically as well as using a Doppler ultrasound. The maturation status of the vein for an increase in vein diameter was evaluated using a high resolution (7 MHZ or higher) linear ultrasound probe. A functioning AVF was evaluated for the diameter of the draining vein at the caudal, mid, and cranial regions of the upper arm. The whole draining vein was scanned. The diameter recorded confirmed the patency of the fistula. The volume flow measurement function of the duplex instrument was used to evaluate the blood flow. A minimum venous diameter of >4 mm or greater and flow volume equal or exceeding 500 ml/min was taken to confirm patency of the fistula at 6 weeks.
The vein diameter at the time of access was measured using duplex ultrasonography before the procedure and was planned for using a PBA Intraop. Measurement was taken at 3 levels: at cubital fossa where anastomosis was performed, mid-arm, and upper arm.10,12
Statistical analysis
With reference to a previous study, 8 we defined a clinically relevant difference of 38% in patency rates of AVF between PBA of small cephalic veins versus HD. Using a two-tailed alpha value of 5% with a power of 90%, a total sample size of 73 was obtained. Hence, in our study, 40 patients were allotted in each group.
Statistical analysis was done using SPSS 17.0. Continuous variables were depicted as mean ± SD or median in case of unevenly distributed data. Categorical variables were expressed as percentages. The comparison of normally distributed continuous variables between the groups was performed using Student's t test Nominal categorical data between the groups were compared using the chi-squared test or Fisher's exact test as appropriate. Non-normal distribution continuous variables were compared using the Mann-Whitney U test. For all statistical tests, a p-value less than 0.05 were taken to indicate a significant difference.
Results
The baseline characteristics of patients in both groups are as given in Table 1. Most patients in either group were aged between 51 and 60 years, with male predominance. The variables, i.e., gender, age, hypertension, hyperlipidemia, tobacco use, coronary artery disease, peripheral artery disease, chronic obstructive pulmonary disorder, diabetes mellitus, and dialysis were comparable between the two groups, with no differences of statistical significance. Most patients in either group had hypertension, hyperlipidemia, diabetes mellitus, and underwent dialysis.
Patient characteristics in both the study groups.
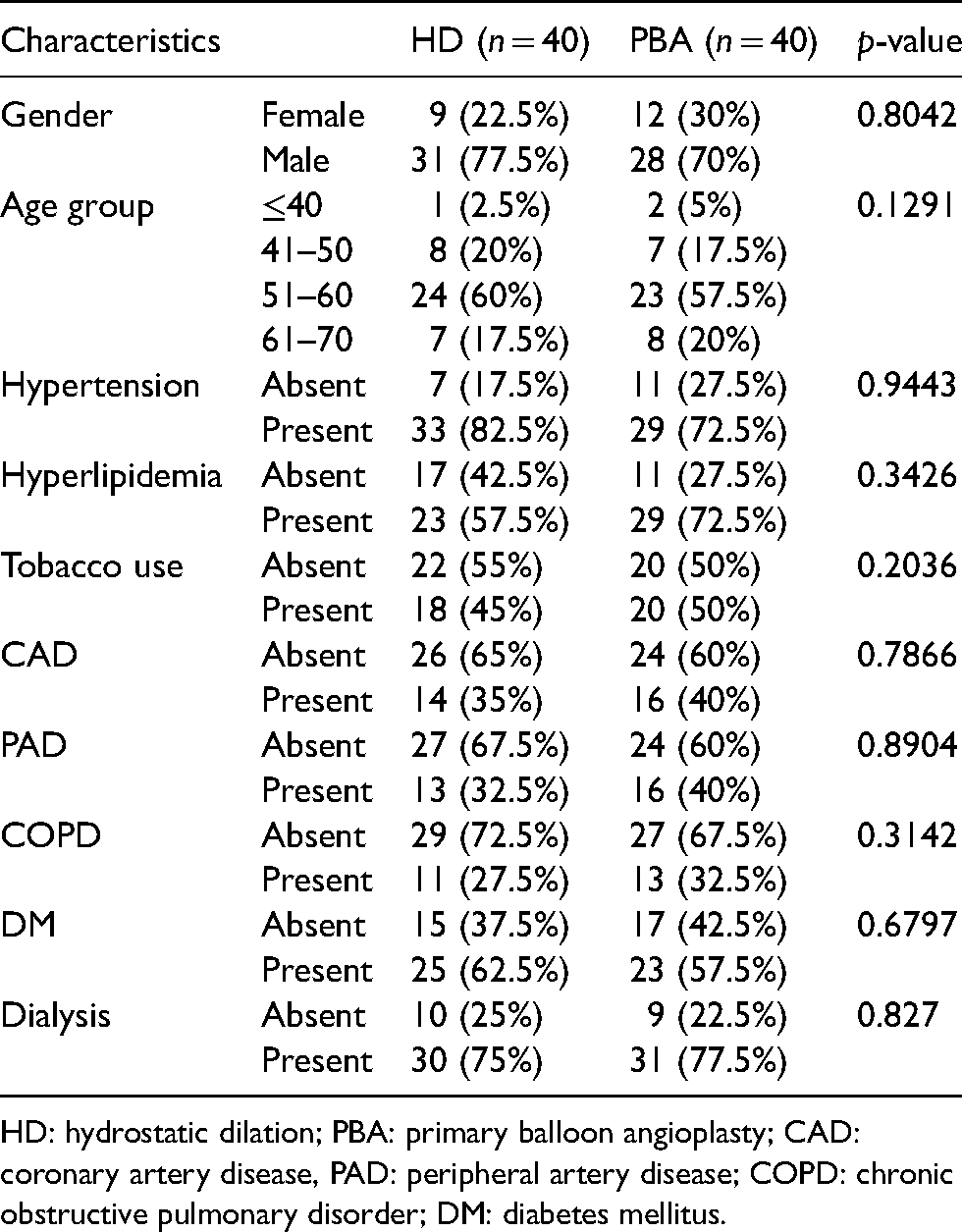
HD: hydrostatic dilation; PBA: primary balloon angioplasty; CAD: coronary artery disease, PAD: peripheral artery disease; COPD: chronic obstructive pulmonary disorder; DM: diabetes mellitus.
The vessel characteristics of patients in both groups are as given in Table 2. None of the factors, arterial diameter, vein diameter, vein diameter at the time of access, were statistically significant. The mean arterial diameter of patients in the HD group was 3.36 ± 1.47 mm while in the PBA group, the mean arterial diameter was 3.33 ± 0.16 mm; however, the difference was insignificant (P = 0.46). The mean vein diameter (mm) was comparable in both groups (2.22 ± 0.12 vs 2.21 ± 0.21; P = 0.65), while vein diameter (mm) at the time of access was significantly greater in the PBA group as compared to HD (6.01 ± 0.63 vs 4.80 ± 0.45; P < 0.001).
Vessel characteristics of the study subjects.
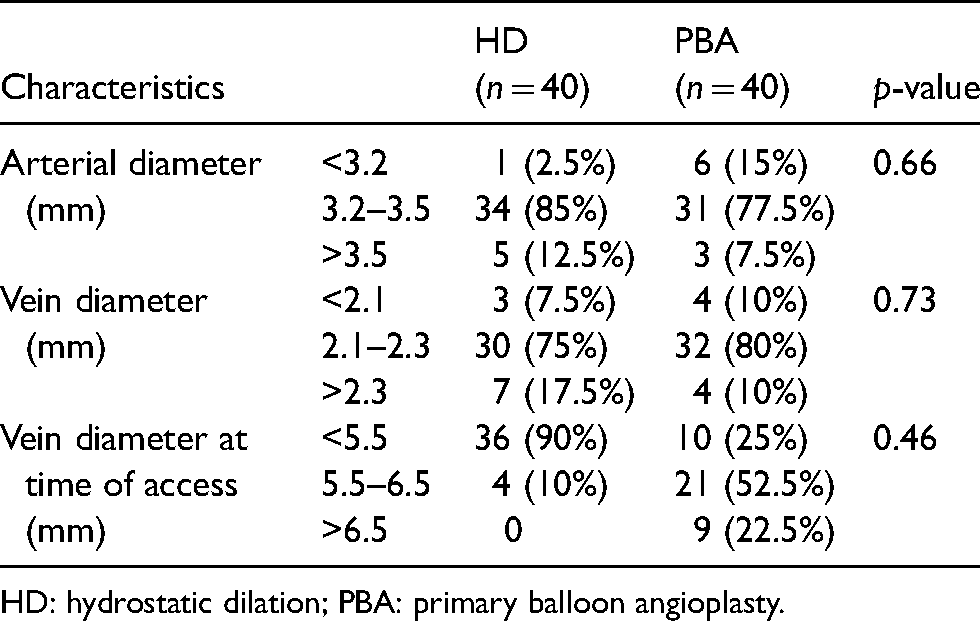
HD: hydrostatic dilation; PBA: primary balloon angioplasty.
The outcome in both study groups is as given in Table 3. However, none of the factors, immediate success, primary patency, AVF functioning, maturation time, SSI, were found to be statistically significant.
Outcome of the techniques in both the study groups.
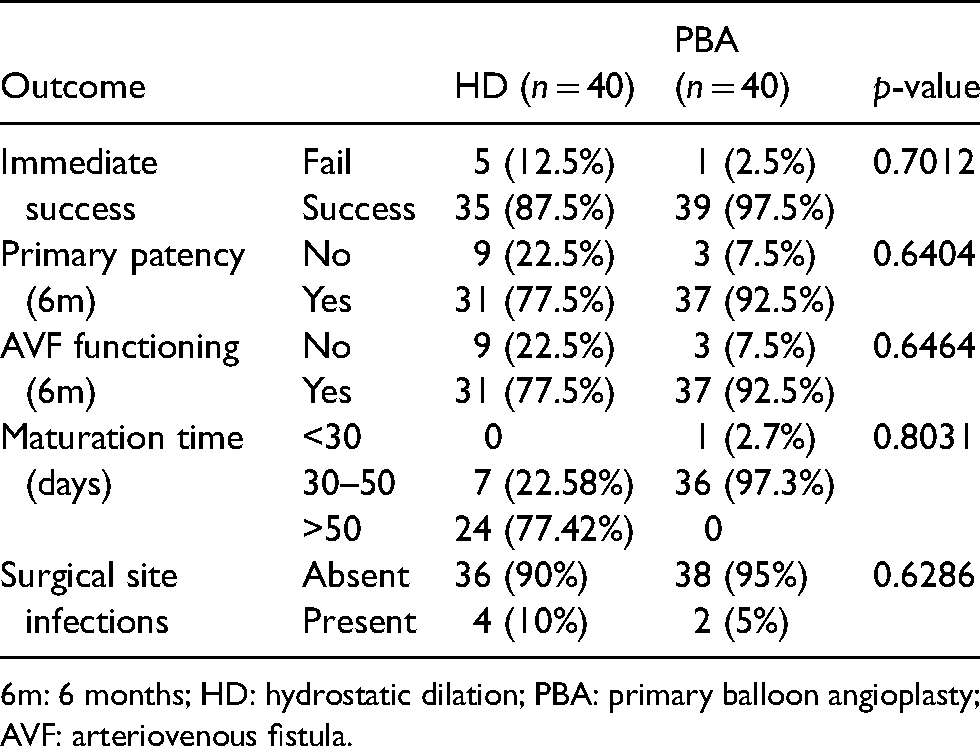
6m: 6 months; HD: hydrostatic dilation; PBA: primary balloon angioplasty; AVF: arteriovenous fistula.
Dialysis was a statistically significant factor associated with primary patency and AVF functioning rate in the HD group and 100% immediate success in both primary patency and AVF functioning rate (Table 4).
Factors associated with primary patency and AVF functioning in hydrostatic dilation.
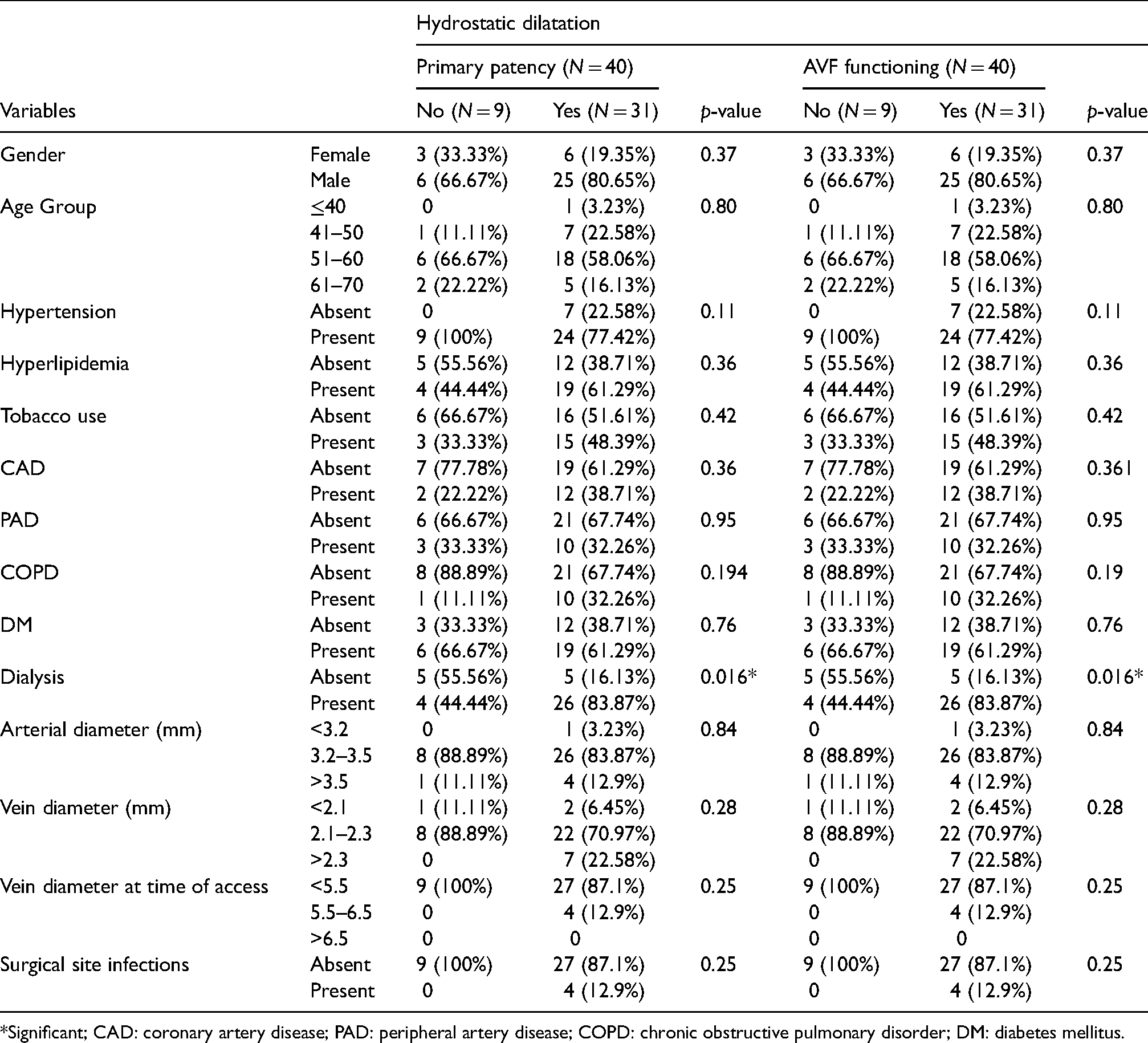
Significant; CAD: coronary artery disease; PAD: peripheral artery disease; COPD: chronic obstructive pulmonary disorder; DM: diabetes mellitus.
Vein diameter was the statistically significant factor associated with primary patency and AVF functioning in the PBA group. Minimum vein diameter of 5.5–6.5 mm at the time of access was significantly associated with better primary patency and AVF functioning (Table 5).
Factors associated with primary patency and AVF functioning during primary balloon angioplasty.
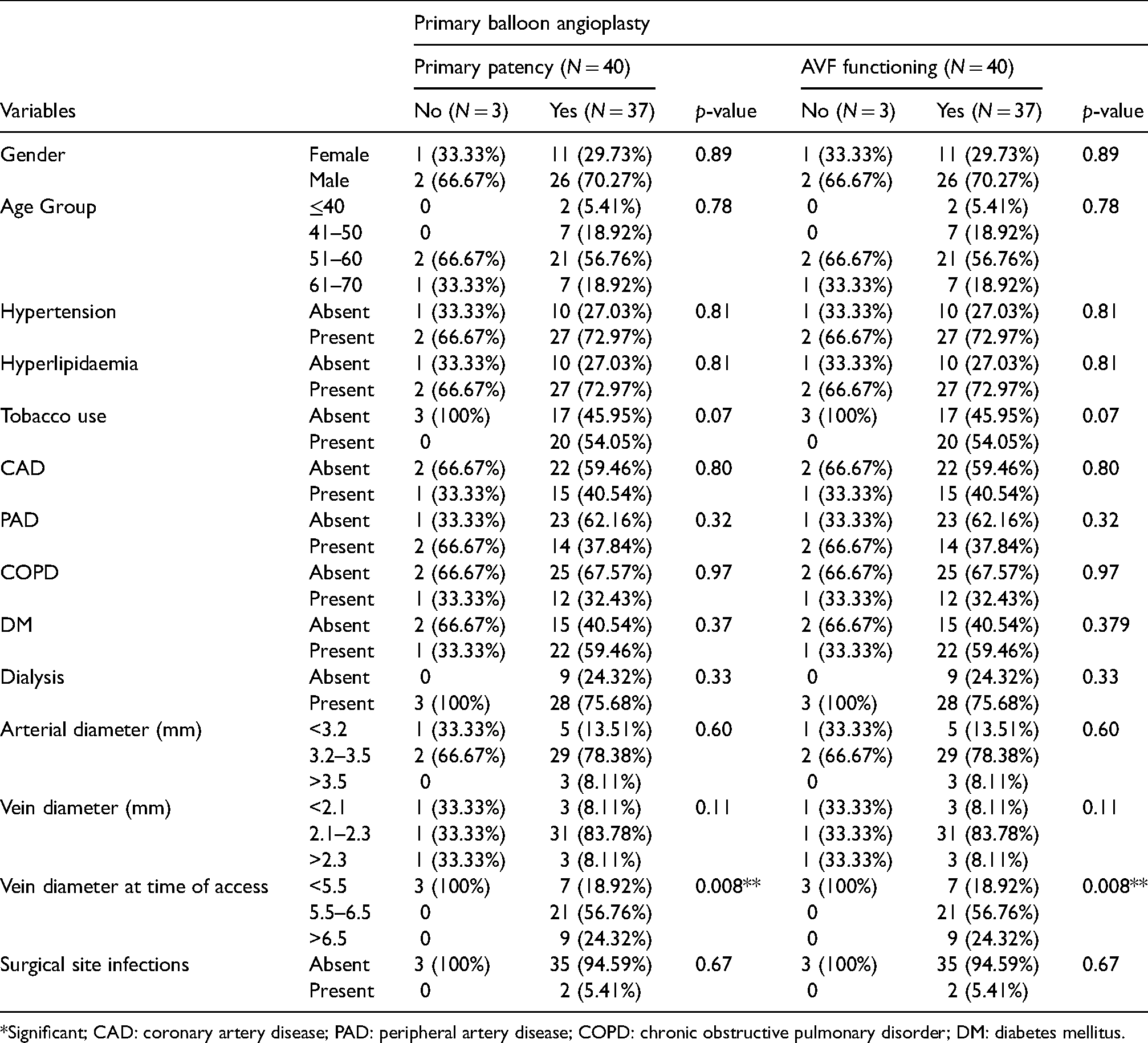
*Significant; CAD: coronary artery disease; PAD: peripheral artery disease; COPD: chronic obstructive pulmonary disorder; DM: diabetes mellitus.
The maturation time of AVF in the PBA group was lower than in the HD group, i.e., the PBA group took 45 days for AVF maturation for dialysis as compared to 60 days in the HD group, although not to a statistically significant degree (P = 0.09; Figure 2).
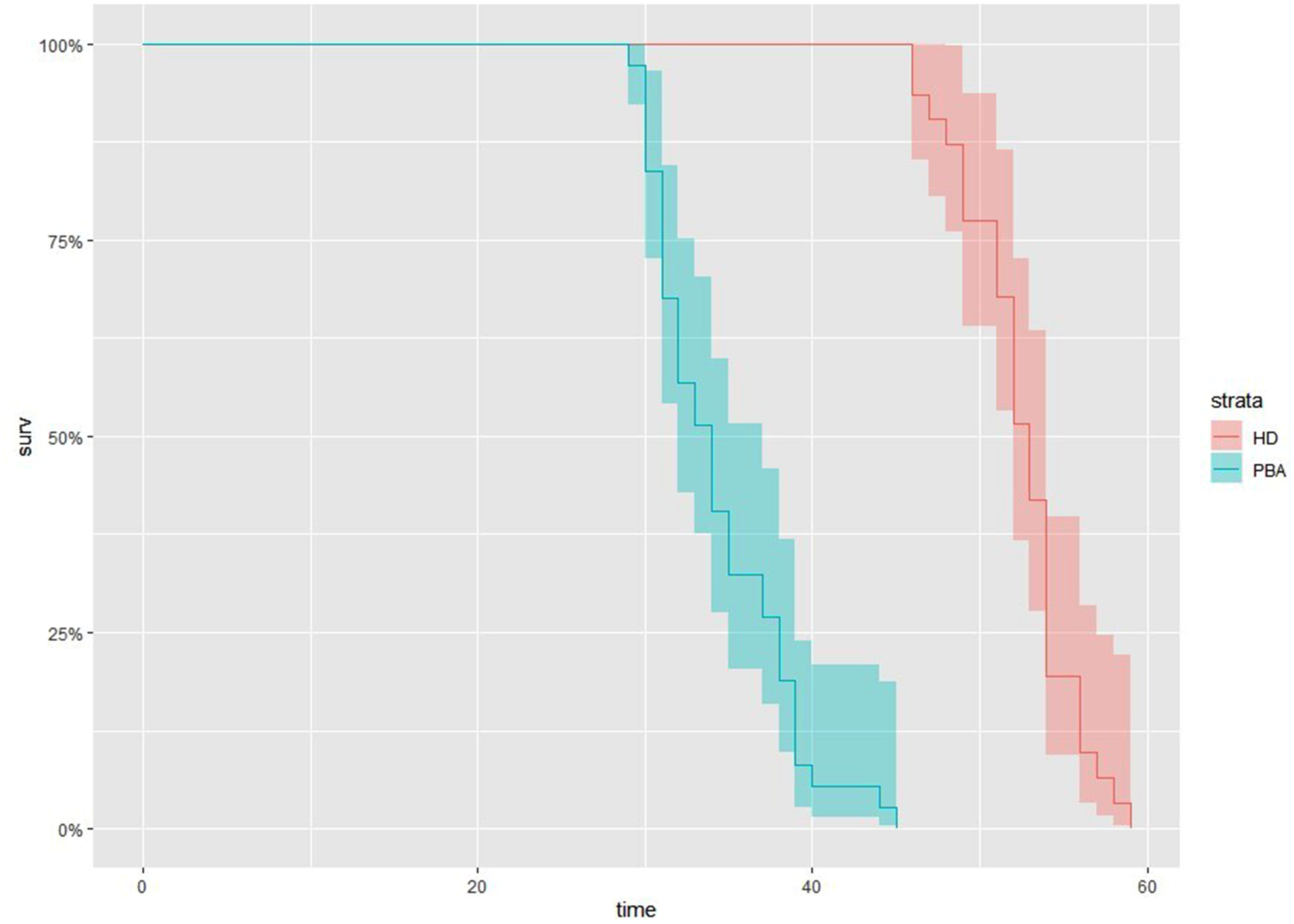
Maturation time at six months of 40 patients undergoing primary balloon angioplasty (PBA; n = 37) or hydrostatic dilatation (HD; n = 31) to mature enough for dialysis.
Discussion
Kidney Disease Outcomes Quality Initiative guidelines state that patients need to have permanent access at the time of initiation of dialysis. 13 A fistula needs to be placed six months before anticipating the hemodialysis. 3 Hence, it is important to preserve as many vessels as possible for AVF creation. 14 However, smaller diameter veins result in increased re-intervention rates and fistulae failures. 11 To tackle this issue, an interesting technique has emerged—the ballooning of small cephalic veins before fistula creation. 15 Hence, the present study utilized the same technique of PBA of small cephalic veins (≤2 mm) prior to fistula creation in one group and indicated this to be a more efficient procedure than standard HD in patients who were rejected formerly due to small cephalic veins.
CKD has been reported in all age groups including pediatric population, young adults, and elderly individuals.16,17 However, in this study, we targeted CKD patients with vein diameter ≤2.5 mm, therefore we got more number of middle-age patients than those younger. As in this study, a few studies have reported that CKD is more prevalent in the male population.18,19 The comorbidity profile in this study was similar to previous reports with hypertension, hyperlipidemia, diabetes mellitus as common causes of CKD.11,14 Brachial artery was the common site to create AVF followed by radial artery, hence the same was dissected and anastomosed with the cephalic vein in this study to create AVF.11,14
Success of AVF creation depends upon the vessel diameter (artery or vein).20,21 It has been stated that small vessel diameter/radius may cause difficulty during anastomosis and restricts the flow, which eventually leads to failure of AVF creation. Moreover, literature has reported that the size of the vessel may influence the patency rate too.11,20,22 The mean arterial diameter and vein diameter of the patients in either group of this study ranged from 3.2–3.5 mm or greater and 2.1–2.5 mm or greater, respectively. Our study also reported that vein diameter was significantly associated with primary patency rates and AVF functioning in the PBA group.
Following AVF creation, immediate success was achieved in 97.5% patients in PBA group and 87.5% in HD group. Similar studies conducted previously have reported even higher failure with HD and more success with PBA.11,23 This would indicate that PBA is an effective method when compared to HD of small diameter cephalic veins (≤2 mm) for AVF creation. Although there were no re-interventions in this study, it has been demonstrated that the re-intervention rate is also low with PBA as compared to HD. 11
The fistula maturation time among patients in the HD group was 46.18 ± 16.27 days (46 days to 59 days) and primary patency was 87.5% while in the PBA group at six months, the fistula maturation time was 34.41 ± 4.07 days (30 days to 45 days) and the patency was 97.5% at six months.
The average fistula maturation time for patients in the PBA group (34.41 days) was lesser when compared to the HD group (46.18 days) in this study. A similar study by Khan et al. 11 also testified that the maturation time was lesser in the PBA group (32.83 days) compared to the HD group (52.53 days). Moreover, the AVF functioning rate in the PBA group (100%) was found to be higher as compared to the HD group (90%), which was similar to this study too, at six months. 11 Veroux et al. 23 also reported lesser patency rates (57%) from HD of small cephalic veins, and excellent patency (95%) and AVF functioning rates (100%) in the PBA group at six months. In this study, only a few patients in both groups reported SSI. Among the six patients with SSI, it was limited to edema/swelling at suture line and serous discharge. None of the patient required re-exploration and were managed conservatively (i.e. antibiotics, antiedema measures like trypsin, bromolien, and rutoside combination, adequate and timely hemodialysis, and compression dressing of forearm to reduce the edema).
The potential shortcomings of the study are as follows. Firstly, the study sample size in both groups was low. Secondly, six-month follow-up period may not be sufficient to draw decisive conclusions. Therefore, a longer follow-up is necessary to identify impending complications. Finally, the techniques were conducted in a particular group of patients and hence may restrict the generalization of findings.
Conclusion
PBA of small caliber cephalic veins (≤2.5 mm) performed before AVF creation for hemodialysis is a beneficial and effective procedure. The technique has higher primary patency rates and requires less maturation time and is superior to the HD technique.
Footnotes
Acknowledgements
Nil.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.