
Abstract
This review discusses the management of acute Type A aortic dissection (ATAAD) complicated by cerebral malperfusion (CMP). While prompt surgical repair is the accepted standard of care for ATAAD, there remains uncertainty and debate about the optimal management of the subgroup of ATAAD patients with CMP. Examined topics include overall survival and neurologic outcomes after surgical repair of ATAAD with CMP, how the severity of presenting neurologic deficits impacts the decision and timing of operation, predictors of postoperative neurologic recovery, and a suggested management algorithm for ATAAD with CMP based upon the best available clinical evidence.
Keywords
Introduction
Acute Type A Aortic Dissection (ATAAD) is a surgical emergency that requires immediate operative correction for ensuring optimal patient outcomes and survival. Dissections involving the head vessels can lead to cerebral malperfusion (CMP), which can subsequently result in transient neurologic dysfunction, as well as irreversible ischemia, permanent neurologic deficits, coma, or death. Thus, the presence of CMP in a patient with ATAAD is associated with particularly poor postoperative outcomes. The optimal management of these patients (i.e. the decision to operate and the appropriate timing of surgical intervention) has not been completely investigated and therefore remains unclear.
This review will address several areas of ongoing debate that arise when managing patients with ATAAD complicated by CMP. The topics of discussion will include the appropriate patient population with CMP who will benefit from surgical intervention, the optimal timing of operation, and lastly the predictors of recovery of neurologic function and long-term survival.
Background
Several of the earliest studies examining management of patients with ATAAD complicated by CMP suggested that immediate surgical repair in these patients could lead to hemorrhagic stroke conversion due to the anticoagulation required for cardiopulmonary bypass.1–3 For this reason, it was hypothesized that patients with CMP would have improved clinical outcomes if surgical repair of dissection was delayed.1,4
One of the first studies to challenge this hypothesis, by Tanaka et al. in 2005, was a single-center study on 63 patients undergoing surgical repair of ATAAD, of whom 25% had CMP. 5 In-hospital mortality was notably higher for patients with CMP than neurologically intact patients (44% vs. 17%). Multivariate analysis demonstrated that CMP was the sole significant risk factor for in-hospital death (hazard ratio 4.25, p = 0.033). Patients who were neurologically intact at presentation also trended towards better 4-year survival, although this difference did not reach statistical significance (75.5% vs. 50.1%, p = 0.091). However, of the 7 patients with CMP who survived to discharge, 3 of them (42%) had no residual neurologic deficit, while the others had either improved or unchanged postoperative neurologic function. The authors therefore conclude that certain ATAAD patients with CMP may be suitable candidates for prompt surgical intervention.
Subsequent studies from the International Registry of Acute Aortic Dissections (IRAD) further supported these conclusions. 6 Of 2202 ATAAD patients between 1996 and 2012, 132 of them (6%) presented with CMP. These patients were significantly more likely to present with syncope (43.5% vs. 15.3%, p < 0.001), as well as other indicators of compromised end-organ perfusion, including hypotension, tamponade, shock (37.4% vs. 26.5%, p < 0.009), or a pulse deficit (50.5% vs. 28.5%, p < 0.001). Patients presenting with CMP had worse in-hospital survival than neurologically intact patients (42.4% vs. 24.1%, p < 0.001), but had a similar 5-year mortality (24.1% vs. 17.2%, p = 0.30). Multivariate analysis demonstrated that surgical correction of ATAAD was a significant and independent protector against in-hospital patient death, regardless of the presence of CMP (odds ratio 0.015, U < 0.001). The authors therefore recommend early surgical intervention and reestablishment of cerebral perfusion.
A more recent IRAD study investigated outcomes on 2402 patients who underwent surgery for ATAAD, of whom 362 (15.1%) had CMP at presentation. 7 Common patient demographics and comorbidities such as age, gender, BMI, and incidence of Marfan's disease were not significantly different between the two cohorts. As with the results of the initial IRAD study, CMP patients were significantly more likely to present with syncope (48.4% vs. 10.1%, p < 0.001), shock (16.2% vs. 4.1%, p < 0.001), and pulse deficits (52.7% vs. 38%, p < 0.001). They were also more likely to require CRRT or prolonged intubation.
Furthermore, patients with CMP had double the in-hospital mortality of neurologically intact patients (25.7% vs. 12.0%, p < 0.001). This survival difference persisted on Kaplan-Meier analysis out to 1 year (62.6% vs. 81.3%, p < 0.001). Cardiac tamponade, myocardial infarction, and CMP were the three strongest predictors of in-hospital mortality. Since all patients underwent surgical correction for ATAAD, this study could not determine whether surgery decreased mortality risk. However, nearly 75% of CMP patients survived to hospital discharge, with an estimated 84% of these patients surviving to 1 year. The authors therefore concluded that these statistics demonstrate a legitimate role for immediate surgery in selected ATAAD patients with CMP.
Does neurologic injury severity affect the decision to repair ATAAD?
Initial studies of ATAAD patients with CMP focused on the impact of surgery on survival. The next appropriate question would therefore be whether preoperative neurologic injury severity should impact decision-making on appropriateness of ATAAD repair, and whether operative intervention will ultimately result in recovery of neurologic function.
Estrera et al. investigated neurologic outcomes on a subset of 16 ATAAD patients who presented with preoperative stroke. 2 Of the 14 patients who underwent surgery, 13 survived (93%). Furthermore, no patient had worsened postoperative neurologic status: 8 patients (57%) either fully recovered or improved, while 6 patients (43%) had no change. These results indicate that surgical repair of ATAAD in the setting of CMP can be performed with acceptable operative mortality and can lead to improvement in neurologic function. Based on these data, the authors recommended prompt ATAAD repair in patients presenting with CMP.
Postoperative outcomes in the subset of ATAAD patients complicated by CMP to the point of coma have also been examined. ATAAD patients who are comatose on presentation have understandably poor outcomes, even when compared to patients with less severe CMP. In the study by Tanaka et al. patients who were comatose for more 3 hours after onset of symptoms had 100% mortality. The authors therefore recommend endovascular stenting of the dissected head vessels in patients presenting with more than 3 hours of severe neurologic compromise. 5 Bossone et al. noted coma to be a significantly negative prognostic factor for patient survival and conclude that comatose patients may not be optimal candidates for emergent repair. 6 These recommendations are consistent with the lower rates of nonoperative management in such patients.
However, in a much larger study, Di Eusanio et al. stratified 1873 IRAD patients into three cohorts: neurologically intact, stroke, and comatose patients. 8 The stroke/comatose cohorts had significantly higher incidences of syncope, hypotension/shock/tamponade, myocardial infarction/ischemia, and pulse deficit at presentation, as previously noted by others.6,7 Neurologically intact patients were most likely to undergo surgery, followed by stroke patients, with comatose patients having the lowest incidence of surgery (86.3% vs. 72.4% vs. 66.7% respectively, p < 0.001).
Independent analysis showed surgical intervention to be universally protective for in-hospital mortality across all three patient cohorts, including coma (odds ratio 0.058, 95% confidence interval 0.018–0.192, p < 0.001). Renal failure, hypotension, shock, and tamponade were significant risk factors for in-hospital mortality. Most notably, patients with major brain injury who were treated surgically had significantly higher 5-year survival than patients treated medically (62.6% vs. 12.2%, p < 0.001). In other words, while comatose patients have worse postoperative outcomes than patients with stroke alone, surgical intervention nonetheless improved in-hospital mortality. The authors therefore conclude “in patients with [ATAAD] and neurologic injury, intervention should always be considered.”
Tsukube et al. reported detailed outcomes on 27 ATAAD patients presenting with coma, defined as a Glasgow Coma Score (GCS) less than 11. 9 Patients presenting within 5 hours of symptom onset (21, 77.8%) underwent immediate surgery, while the remainder (6, 22.2%) were initially managed medically, with 3 eventually undergoing delayed surgical repair. Full recovery was noted in 86% patients, and delayed recovery in 17%. Patients with delayed presentation had a higher incidence of shock and pericardial effusion on presentation, although the cohorts were underpowered for this to be a significant difference. Additional analysis showed that comatose patients who were promptly repaired had significantly higher 5-year survival than those who underwent medical management alone (60% vs. 17%, p < 0.0001). 10 Cox regression analysis indicated that surgical intervention was the only significant predictor of 5-year survival, even after adjusting for severity of presentation. These remarkable results argue for immediate surgical repair, even in the ATAAD patient population presenting with coma due to severe neurologic injury.
Predictors of postoperative neurologic recovery
The best extant clinical evidence supports surgical intervention in the majority of ATAAD patients with CMP, even in the setting of coma. However, the ultimate decision to operate should incorporate patient comorbidities, clinical presentation, and a realistic assessment for postoperative survival and neurologic recovery. It would therefore be important for a clinician to have complete understanding of the potential predictors of postoperative neurologic improvement.
Multiple studies, beginning with Tanaka in 2005, have identified a clear association between rapid surgical intervention and improved postoperative neurologic outcomes. Morimoto et al. reported outcomes on 41 patients with ATAAD and CMP who underwent surgery. 11 Nearly two-thirds of patients (63%) had improved neurologic function postoperatively (defined as an increase of 4 points or more on the 42-point NIH Stroke Scale, or NIHSS). Predictors of postoperative recovery included a preoperative NIHSS score greater than 11, surgical intervention within 9 hours of symptom onset, and lack of brain infarction on postoperative imaging.
Tsukube et al. assessed the preoperative neurologic deficit of 53 ATAAD patients by the Glasgow Coma Scale (GCS) and modified Rankin Scale (mRS). 12 More than half of the patients (54%) showed complete postoperative neurologic recovery. A high preoperative mRS (indicating more severe neurologic injury) was significantly associated with persistent postoperative neurologic deficit (p = 0.007), while a lower GCS score, indicative of more severe neurologic injury, showed a similar association but did not reach statistical significance. Patients demonstrating neurologic recovery had a lower incidence of obesity and a higher rate of smoking, although these factors did not predict neurologic recovery. The operations conducted between the groups were not significantly different.
Fukuhara et al. examined the significance of carotid artery dissection on postoperative outcomes of 59 patients with CMP secondary to ATAAD. 13 Occlusion of the internal carotid artery (ICA) was uniformly fatal; however, unilateral or even bilateral common carotid artery (CCA) occlusion was not associated with an increased risk of death (79% of patients survived to discharge). The study notes that while ICA occlusion strongly correlated with patient mortality, there was no correlation with ischemic findings on non-contrasted head CT or clinical exam, as nearly half of patients with ICA occlusion were conscious. The authors conclude that additional studies are needed to investigate these findings.
Preoperative considerations in ATAAD patients with CMP
The time to operation is a key risk factor affecting patient survival and neurologic recovery and is also a variable that lies within a clinician's control once the appropriate diagnosis is made. Therefore, any patient presenting with evidence of neurologic injury or syncope in conjunction with hypotension, shock, a pulse deficit, or aortic regurgitation should raise immediate suspicion for ATAAD with CMP. These patients must have prompt diagnosis or rule-out of aortic dissection, as delay in diagnosis can be lethal. 7 Furthermore, the role of lytic agents such as tissue plasminogen activator (TPA) in this population is not clear, and may be contraindicated if the patient is a candidate for immediate surgical repair.
In an ATAAD patient with CMP, clinical assessment tools such as the GCS, NIHSS, and mRS scales can be useful when predicting postoperative neurologic recovery. The absence of findings on CT or MRI does not rule out acute ischemia/infarction, and their presence does not preclude surgery. 9 Cerebral hemorrhage is an exception that should be stabilized before proceeding with systemic anticoagulation and surgical repair. The surgeon should also consider dedicated angiography of the head and neck vessels, as the presence of ICA occlusion is a potentially poor prognostic factor; however, performing this study must be weighed against any possible resulting delay in operative intervention. Finally, targeted endovascular revascularization of the head/neck vessels represents a potential option for patients with CMP who are deemed too unstable for immediate aortic repair.
Conclusions
Prompt surgical repair is the standard of care for acute Type A aortic dissection. The median survival of patients treated successfully with surgery is greater than 10 years, while virtually no patients treated nonoperatively will survive past 1 year. However, ATAAD patients with CMP have historically presented a special challenge, given the theoretical risk of hemorrhagic conversion, as well as the known associated poor prognosis of severe ischemic brain injury. This has traditionally resulted in a strategy of delayed surgical management when treating this particular cohort of ATAAD patients.
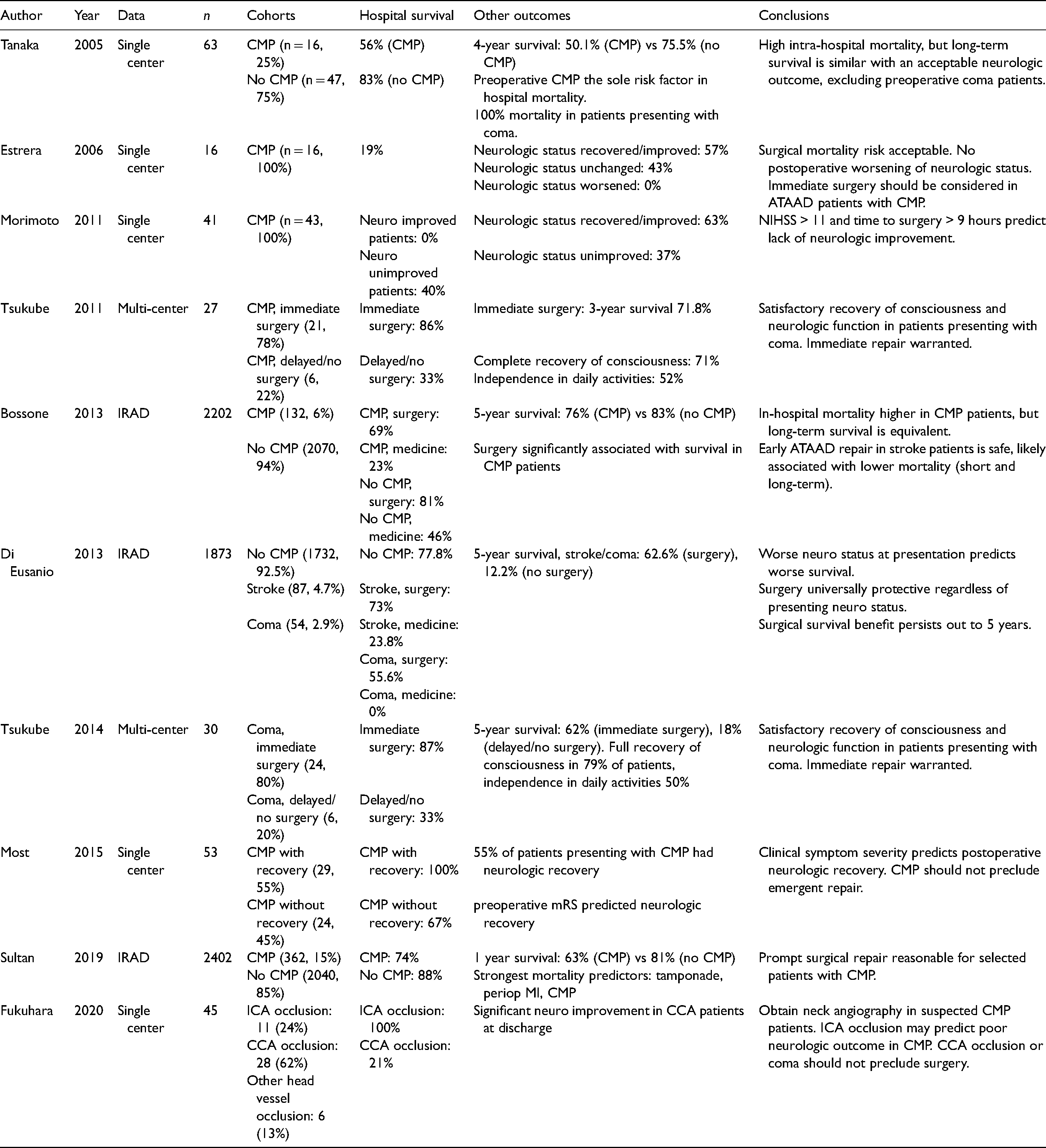
However, there is now a growing body of evidence (summarized in Table 1) that supports immediate operative intervention in ATAAD patients presenting with CMP in a similar manner to neurologically intact patients presenting with ATAAD. Conversely, delays in surgical repair have been shown to be associated with worse outcomes. While outcomes are generally worse for ATAAD patients with CMP, multiple reports associate immediate surgery with a beneficial reduction in patient mortality, which also includes patients who present with coma. Multiple studies have demonstrated increased overall survival, neurologic improvement, or even recovery in a substantial portion of ATAAD patients presenting with CMP.
Summary of reviewed studies. ATAAD = acute type A aortic dissection, CCA = common carotid artery, CMP = cerebral malperfusion, ICA = internal carotid artery, IRAD = International Registry of Acute Aortic Dissections, MI = myocardial infarction, mRS = modified Rankin score, NIHSS = National Institutes of Health Stroke Scale.
The presence of CMP in ATAAD patients, including profound neurologic dysfunction and coma, is not an absolute contraindication for prompt surgical correction. An individualized approach, as demonstrated in the algorithm in Figure 1, may allow clinicians to appropriately triage patients with CMP into immediate or delayed operative repair. Balancing patient comorbidities, neurologic status, and likelihood for recovery ultimately remains the optimal treatment strategy for this complex patient population.
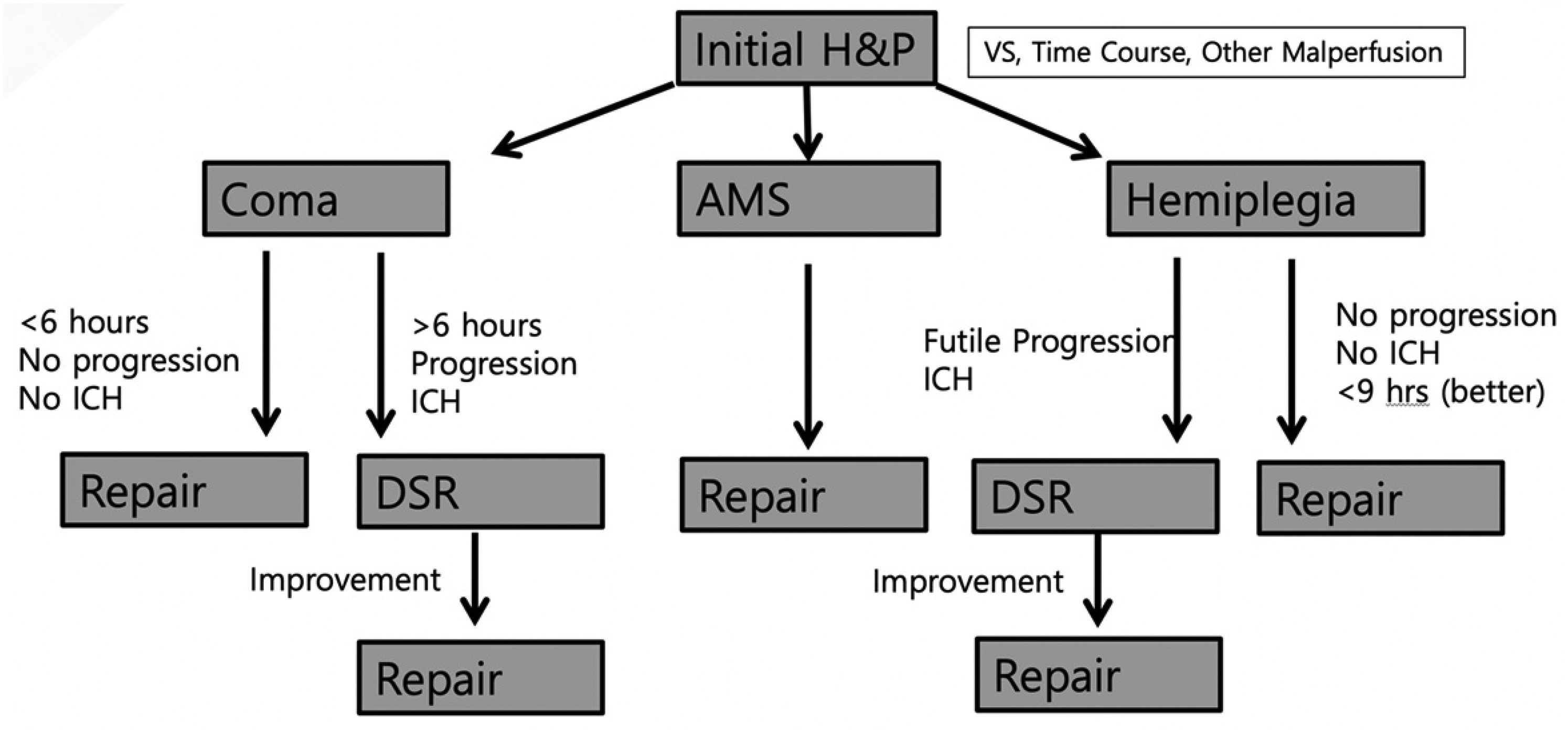
Suggested algorithm for management of ATAAD with cerebral malperfusion. 2 Initial assessment should consider the patient’s vital signs (VS), the time course/duration of disease, and the presence of other malperfused organs. Consider immediate repair in patients with altered mental status (AMS) or clinically stable coma/neurologic deficits without evidence of intracranial hemorrhage (ICH). Patients who are worsening or have evidence of ICH should be managed medically, with consideration of delayed surgical repair (DSR).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethics committee review was not applicable for this review article.
Informed consent
Informed consent was not sought for this review article because no protected health information or patient-identifiable images or information was used.