
Abstract
Background
Open total arch replacement is one of the most challenging procedures in cardiothoracic surgery and is the gold standard treatment for aortic arch pathology. Total arch replacement is associated with high rates of mortality and neurological morbidity. Using 14 years of data, we studied postoperative, in-hospital mortality, major complications, and examined associated risk factors.
Materials and method
Medical records of patients who underwent open, total arch replacement surgery at Siriraj Hospital from 2006 to December 2019 were reviewed. Demographic data, clinical factors, preoperative status, intraoperative data, and postoperative data were analyzed.
Result
A total of 330 patients were included and 36 (10.9%) died in the hospital. More than one concomitant operation (odds ratio (OR) 5.16, p < 0.001) and emergency operation (OR 3.45, p = 0.003) were risk factors for in-hospital mortality. Major postoperative morbidity occurred in 124 (37.7%) patients (124 of 329). Emergency operation (OR 2.88, p <0.001), preoperative creatinine clearance < 60 ml/ min/ 1.73 m2 (OR 2.04, p = 0.004), and aortic cross-clamp time > 180 min (OR 1.75, p = 0.022) were risk factors for major postsurgical complications.
Conclusion
In-hospital mortality after total arch replacement was 10.9% compared to international reports. Emergency operation was a major risk factor for both mortality and major complications. More than one concomitant operation, especially coronary artery bypass graft, more than doubled the risk of major complications.
Background
Open total arch replacement (TAR) is one of the most challenging procedures in cardiothoracic surgery and is the gold standard treatment of aortic arch pathology, including dissection and aneurysm. Unavoidable interruption of normal blood flow to the brain and lower body makes TAR a high mortality and high neurological morbidity operation. However, due to recent advances in cerebral protection techniques, TAR outcomes have improved.1,2
With improvement in surgical and brain protection techniques, TAR is now a common operation with reduced mortality occurring in 0%–18.9% of patients.1–14 The reported incidence of permanent neurological deficit (PND) and neurological deficits persisting at discharge is between 1.4% and 14.5%.1–4,6,7,9–13 Postoperative kidney failure requiring hemodialysis occurs in 6.7%–21.4% of patients.1,4,6,7,13
Okita Y. et al. published a single-center study of 423 Japanese patients and reported early postoperative mortality to be 4.5%. The incidence of PND and transient neurological deficits (TND) were 5.4% and 8.7%, respectively. The study demonstrated that cardiopulmonary bypass time (CPB time), age over 80 years, and preoperative stroke were risk factors for mortality. Finally, shaggy aorta (diffuse, irregularly shaped atherosclerotic changes in the aorta) and poor cardiac contraction were risk factors for neurological deficits. 7
At Siriraj Hospital, the largest tertiary hospital with an aortic center in Thailand, the first TAR was performed nearly 20 years ago, however, TAR data is available beginning in 2006. The primary objective of this study was to measure early (in-hospital) postoperative mortality. The secondary objective was to determine the rate of major complications such as neurological deficits, and to explore the associated risk factors.
Materials and methods
We conducted a retrospective review of patients who underwent TAR at Siriraj Hospital from 2006 to December 2019. Patients who underwent TAR together with other operations, including aortic root replacement, and frozen elephant trunk were included. Patients that underwent hemiarch or partial arch replacement were excluded. Demographic data, clinical factors, preoperative status, intraoperative data, and postoperative mortality and complications were reviewed. Ethical approval was granted by the human research protection unit of Siriraj Hospital.
Surgical technique
Patients were placed in the supine position with a minimum of two arterial lines, usually at both radial arteries, to monitor pressure during antegrade cerebral perfusion. We used a nasopharyngeal probe and a rectal probe for body temperature monitoring, and kept the temperature difference between the two sites at less than 5°C during the cooling and rewarming periods to avoid air bubble formation in the blood. We used near-infrared spectroscopy (NIRS) applied to the bilateral forehead to monitor frontal brain regional tissue perfusion.
We carefully studied the preoperative computed tomography angiography (CTA) to choose the optimal arterial cannulation site. We preferred to use the right axillary artery first but if the patient was hemodynamically unstable, the femoral artery was used first. Most patients underwent operation through median sternotomy, while others with combined descending thoracic aortic aneurysm were approached through thoracotomy or clamshell incision.
To minimize bleeding due to the systemic heparinization effect, all arch branches and the proximal aortic arch were dissected free from the surrounding tissues before beginning CPB. After patients were placed on CPB, we inserted a left ventricular vent through the right superior pulmonary vein for cardiac protection. After the nasopharyngeal temperature dropped to 18–23°C, circulation was stopped, and direct antegrade cerebral perfusion was given at a rate of 15 ml/kg/min. If the patient had right axillary artery cannulation, cerebral perfusion catheters were inserted into the left common carotid artery and the left subclavian artery. In the case of femoral artery cannulation, cerebral perfusion was given directly through all tree arch branches. We used NIRS and perfusion pressure from both arterial lines to monitor the adequacy of cerebral perfusion.
A four-branch graft (10, 8, 8, 8 mm) was routinely used. Distal anastomosis to the descending thoracic aorta was created using 4-0 continuous or horizontal mattress suture with pledged support inside and strip support outside. After complete distal anastomosis, body perfusion was restarted through a side branch of the graft. Flow was increased up to 2 l/min/m2 to check for bleeding from the distal anastomosis and then rewarming was started. Next, proximal anastomosis to the sinotubular junction or arch branch reimplantation was performed according to the preference of the attending surgeon. Proximal anastomosis was created with 4-0 monofilament suture using interrupted horizontal mattress sutures or continuous suture. After complete proximal anastomosis, heart de-airing was followed by cross-clamp removal to initiate blood supply to the coronary artery. Individual arch branch reimplantation was created using 5-0 or 6-0 monofilament continuous suture.
Definition of postoperative complications
PND are complications with abnormal brain imaging due to hemorrhage or infarction. The brain computed tomography (CT brain) was sent if patients didn't gain conscious after 6 h after the operation or those who have abnormal neurological sign, alternation of conscious, or seizure postoperatively. TND are neurological deficits that have normal brain imaging, such as seizures and alterations of conscious without focal neurological deficits. We categorized patients with neurological complications into permanent and transient deficit groups. Acute kidney injury (AKI) was defined as new-onset kidney injury that was recorded in the patient discharge summary and/or required hemodialysis support. We defined major complications such as pneumonia, pulmonary hemorrhage, respiratory failure, acute respiratory distress syndrome (ARDS), reoperation in the same admission, postoperative myocardial infarction or heart failure, new-onset postoperative hemodialysis, PND (stroke), and sepsis. The document of major complications was based on the patient discharge summary.
Statistical analysis
Descriptive statistics were used to describe baseline characteristics. Data are presented as medians with minimum and maximum values, means with SD, or frequencies with percentages as appropriate. Univariate analysis to detect an association between two variables used the chi-square or Students’ t-test/Mann–Whitney U test, as appropriate. For continuous data such as bypass time, cross-clamp time, the optimal cut-point value was selected by receiver operating characteristic (ROC) curve analysis. The value whose sensitivity and specificity were closest to the value of the area under the ROC curve and the absolute value of the difference between the sensitivity and the specificity value was minimal, was selected. Variables that had p-value < 0.05 in univariate analysis were assessed by Spearman's rank correlation test before variables were included in multivariate analysis. For multivariate analysis, the forward stepwise binary logistic regression analysis was used to select potential variables in the final model. A p-value <0.05 was set as the threshold for statistical significance. SPSS program version 18 was used for all statistical analyses.
Results
Patient characteristics
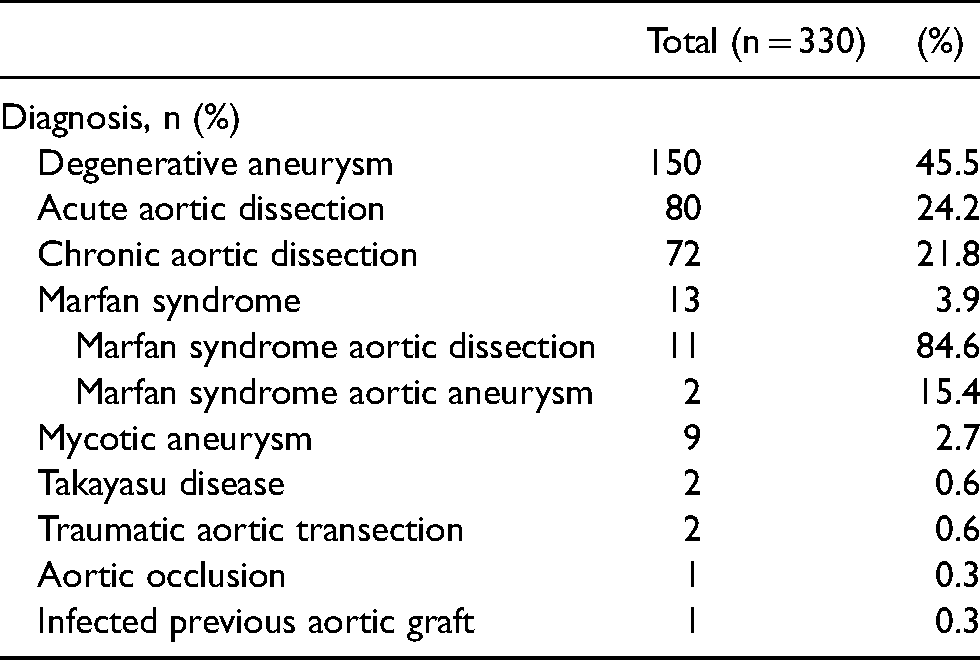
From June 2006 to December 2019, 330 patients underwent TAR. The mean age of patients was 63 years and 222(67.3%) patients were male. Degenerative aneurysm was the most common diagnosis (150 cases, 45.5%), followed by acute (80 cases, 24.2%) and chronic (72 cases, 21.8%) aortic dissection (Table 1). We performed emergency operations in 138 (41.8%) patients. Thirty-two (9.7%) patients underwent repeated surgery through a healed incision. Essential hypertension, history of smoking, and preoperative poor glomerular filtration rate (GFR), defined as a creatinine clearance less than 60 ml/min/1.73m2, were common concomitant conditions (Table 2). One hundred and twenty patients had poor preoperative GFR. One hundred and eighty-seven (56.7%) patients had concomitant operations and 50 (15.15%) patients underwent 3 or more operations simultaneously. The most common concomitant operation was coronary artery bypass graft (CABG) (90 cases, 27.3%), followed by frozen elephant trunk (67 cases, 20.3%), and aortic root surgery (33 cases, 10%).
Diagnosis.
Operative data
The average operative time was 503.3 ± 189.2 min and the average CPB time was 230 ± 107.8 min. The average aortic cross-clamp time was 186.1 ± 98.7 min and the average lower body ischemic time was 75.6 ± 41.7 min. In most cases, we used moderate hypothermia according to the definition by consensus on hypothermia in aortic arch surgery. The average lowest body temperature was 21.3 ± 2.6 °C. Selective, antegrade cerebral perfusion was applied in 306 (92.7%) patients (Table 3).
Outcomes
The in-hospital mortality rate was 10.9% (36 patients) (Table 4). In emergency cases, the mortality rate was 15.2% (21/138). In elective cases, the mortality rate was 7.8% (15/192), (p = 0.011). The mortality rate in aortic dissection cases was 12.9% (21/163), and the mortality rate in aortic aneurysm cases was 9.1% (15/165). Analysis demonstrated that the risk of in-hospital mortality increased with two or more concomitant operations (univariate OR 3.37 (1.56–7.30); p = 0.001) (multivariate OR 5.16 (2.08–12.82); p < 0.001) and emergency operation (2.12 (1.05–4.28); p = 0.030) (multivariate OR 3.45 (1.50–7.92); p = 0.003) (Table 5). The median hospital stay was 12 days. The median ICU stay was 4 days, and the median intubation time was 29 h. One case was excluded from the analysis of complications due to death on the table. Major complications occurred in 37.7% (124/329). Aortic aneurysm cases had more major complications than aortic dissection cases (42% vs. 32.7%) (p = 0.08). Emergency cases had significantly more major complications (51.8% vs. 27.6%; p < 0.001). Risk factors for major complications included emergency operation (univariate OR 2.82 (1.78–4.47); p < 0.001) (multivariate OR 2.88 (1.79–4.62); p < 0.001), preoperative creatinine clearance < 60 m/min/1.73 m2 (univariate OR 2.21 (1.39–3.51); p = 0.001) (multivariate OR 2.04 (1.26–3.30); p = 0.004, and an aortic cross-clamp time > 180 min (univariate OR 1.75 (1.11–2.76); p = 0.015) (multivariate OR 1.75 (1.09–2.82); p = 0.022) (Table 6).
Demographic data.
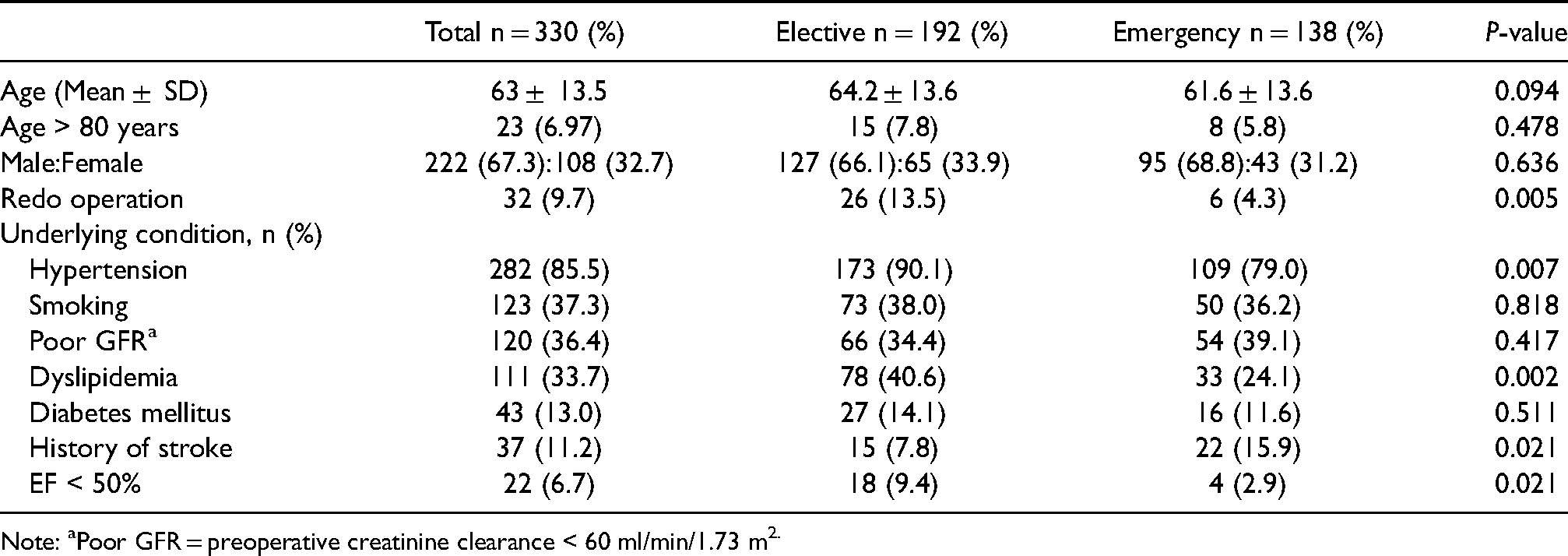
Note: aPoor GFR = preoperative creatinine clearance < 60 ml/min/1.73 m2.
Operative data.
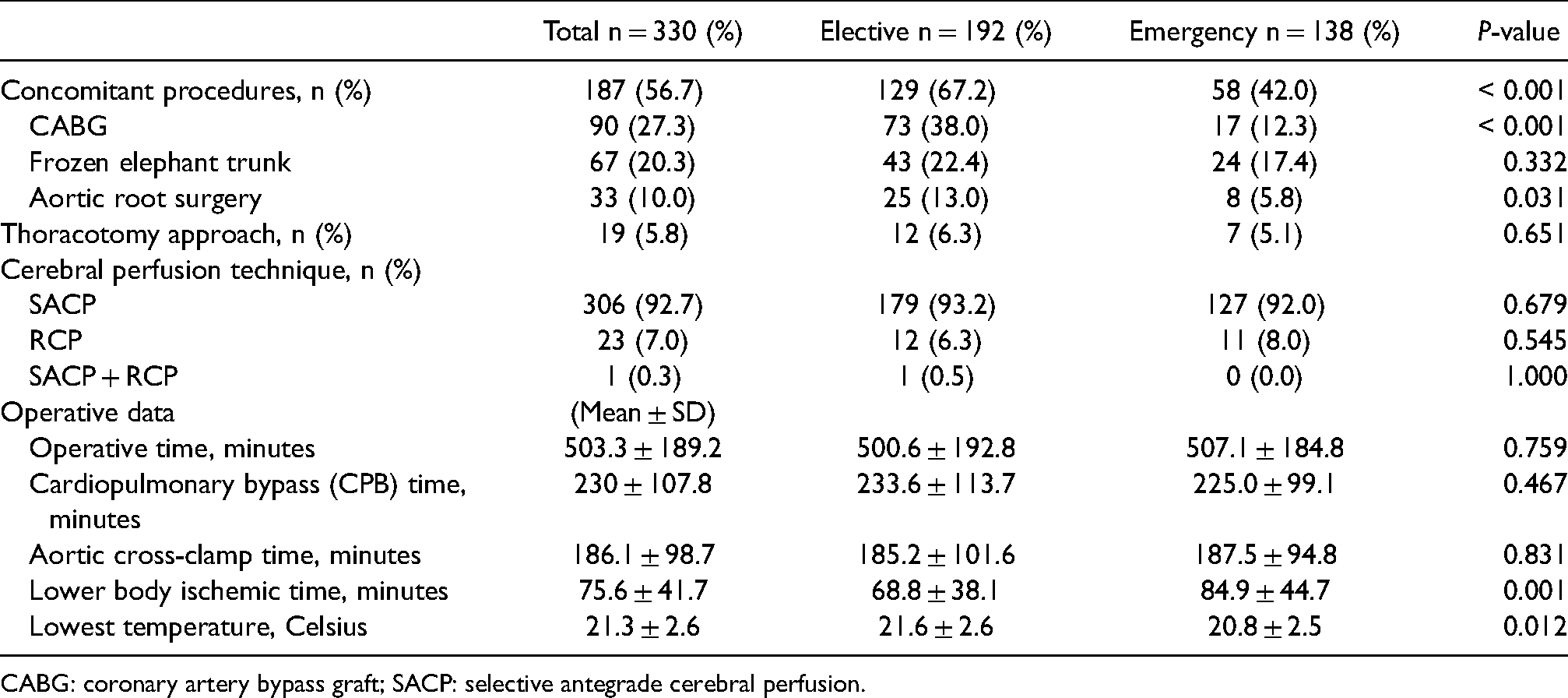
CABG: coronary artery bypass graft; SACP: selective antegrade cerebral perfusion.
Perioperative outcomes.
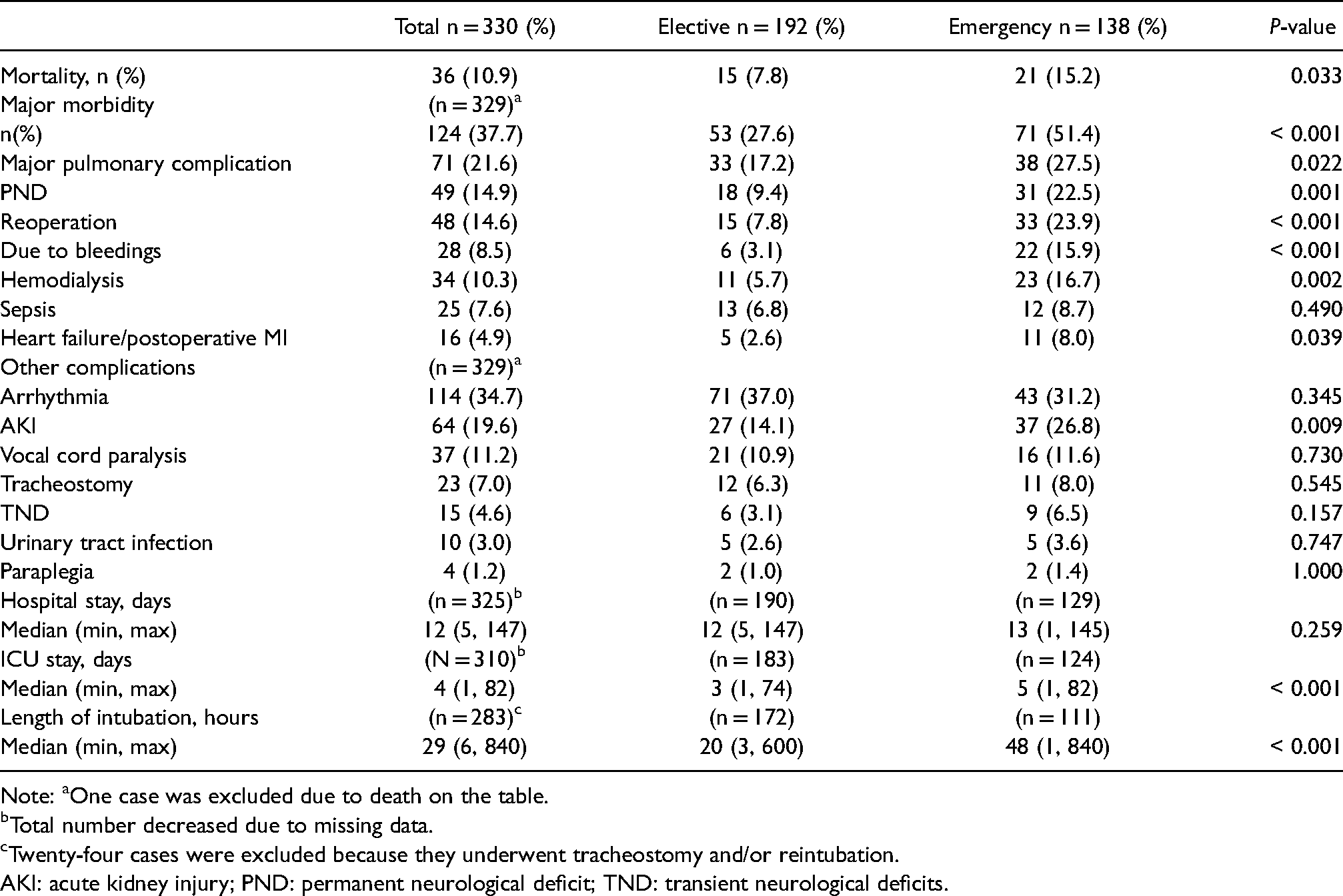
Note: aOne case was excluded due to death on the table.
Total number decreased due to missing data.
Twenty-four cases were excluded because they underwent tracheostomy and/or reintubation.
AKI: acute kidney injury; PND: permanent neurological deficit; TND: transient neurological deficits.
Common major complications included pulmonary complications (71 cases, 21.6%), PND (stroke) (49 cases, 14.9%), reoperation (48 cases, 14.6%), and new-onset kidney failure requiring hemodialysis (34 cases, 10.3%). Seventy-one (21.6%) patients had major pulmonary complications including pneumonia, pulmonary hemorrhage, respiratory failure, or ARDS. Prolonged operation > 500 min (univariate OR 2.43 (1.42–4.14); p = 0.001) (multivariate OR 2.41 (1.40–4.15); p = 0.002), emergency operation (univariate OR 1.85 (1.09–3.14), p = 0.022) (multivariate OR 1.89 (1.10–3.26); p = 0.022), and smoking (univariate OR 1.75 (1.03–2.97); p = 0.039) (multivariate OR 1.77 (1.02–3.06); p = 0.041) significantly increased the risk for pulmonary complications. Major pulmonary complications were more likely in patients who underwent operation through thoracotomy (36.8% vs. 20.6%; p = 0.145).
Forty-nine (14.9%) patients developed PND. Twenty-eight patients (8.51%) had ischemic stroke, 17 patients (5.17%) had intracranial hemorrhage (ICH), and 4 patients (1.22%) had mixed pathology including both infarction and hemorrhage. Eleven patients (5.7%) of elective patients and 17 patients (12.4%) of emergency patients had an ischemic stroke, while 5 from 28 (17.9%) patients had hemorrhagic transformation. Seventeen (5.17%) patients had SDH, one patient had epidural hemorrhage, and one patient had intracerebral hemorrhage. All patients with mixed pathology had acute SDH with ischemic stroke. No patients with SDH had a midline shift and none required surgical evacuation. Risk factors for PND included emergency operation (univariate 2.83 (1.51–5.30; p = 0.001) (multivariate OR 2.62 (1.36–5.05); p = 0.004), preoperative creatinine clearance < 60 m/min/1.73 m2 (univariate 2.20 (1.19–4.06); p = 0.010) (multivariate 2.26 (1.20–4.28); p = 0.012, and a lower body ischemic time > 70 min (univariate OR 2.44 (1.29–4.61); p = 0.005) (multivariate OR 2.10 (1.08–4.05); p = 0.028) (Table 7).
Risk factors for in-hospital mortality.
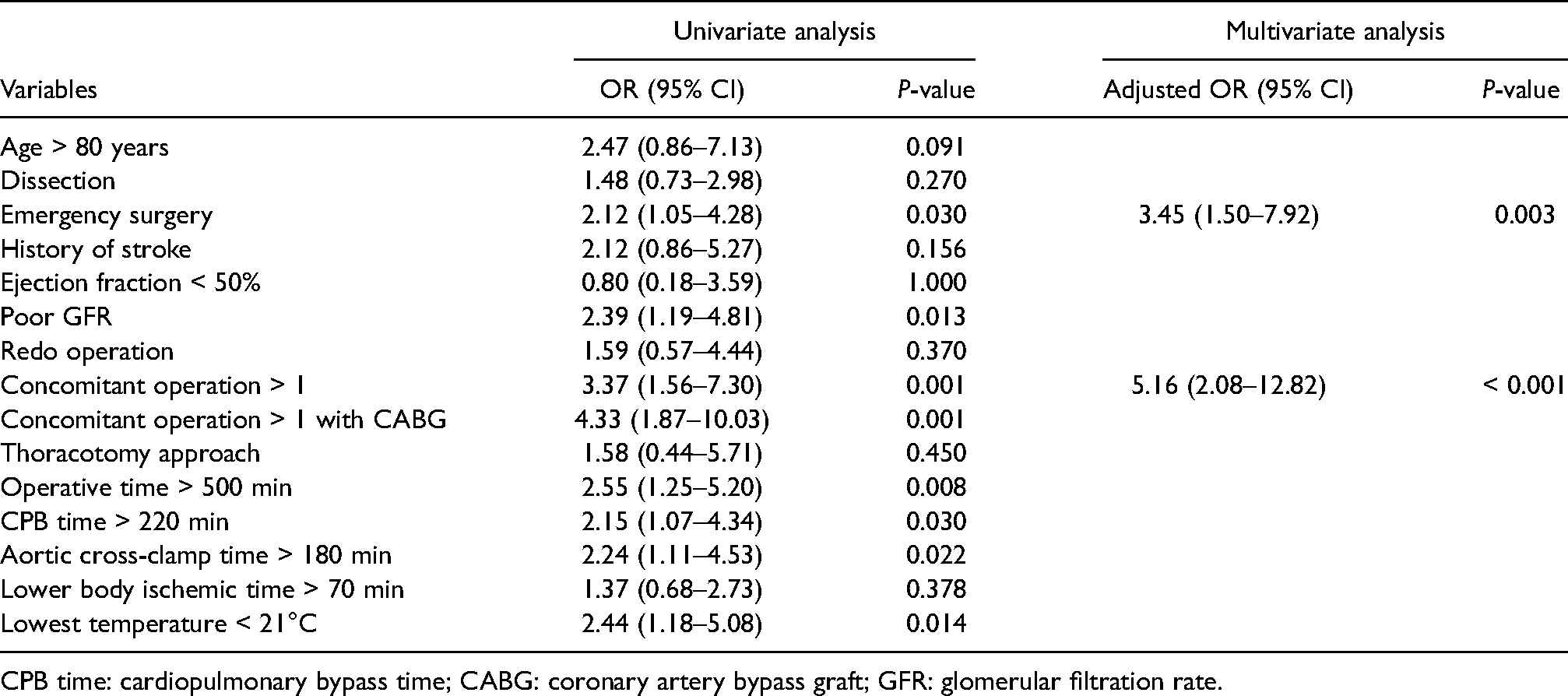
CPB time: cardiopulmonary bypass time; CABG: coronary artery bypass graft; GFR: glomerular filtration rate.
Risk factors for major morbidity.
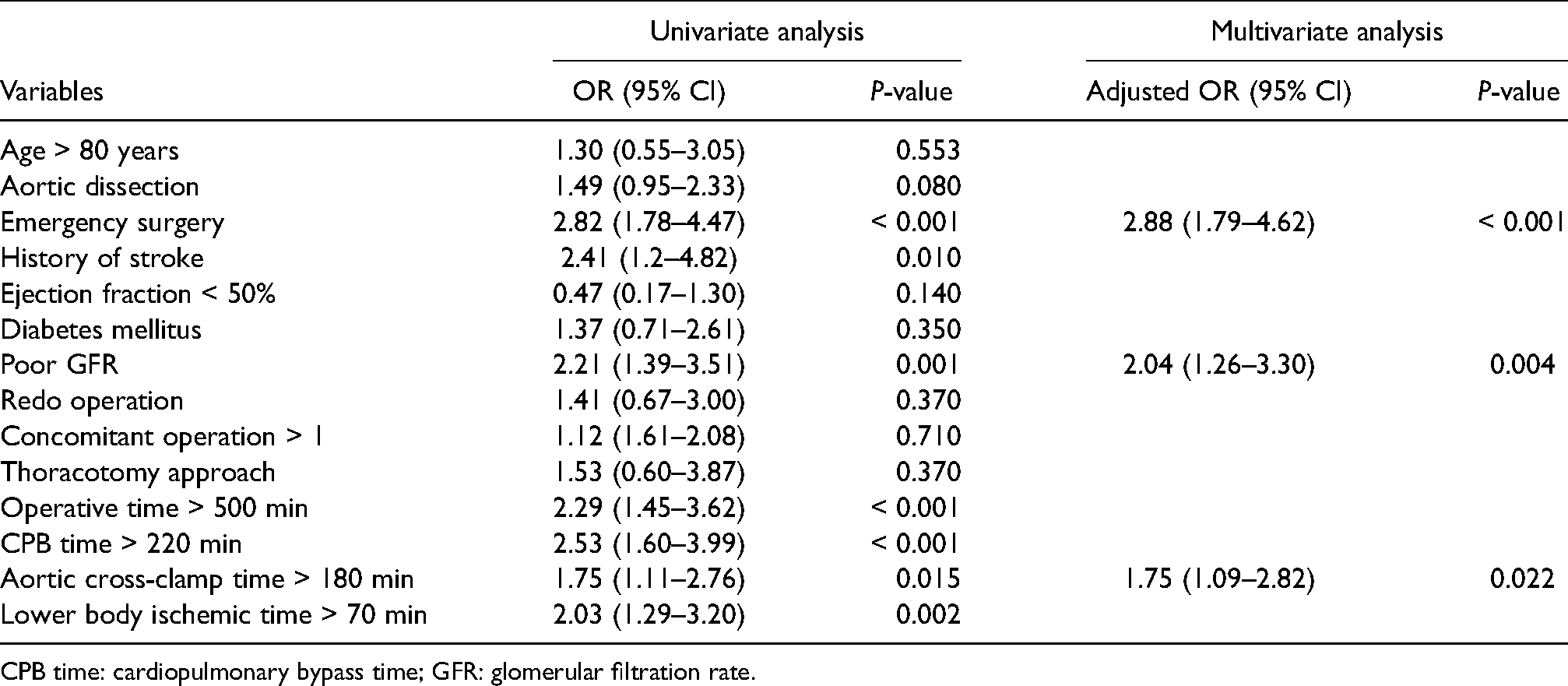
CPB time: cardiopulmonary bypass time; GFR: glomerular filtration rate.
Risk factors for permanent neurological deficit (PND).
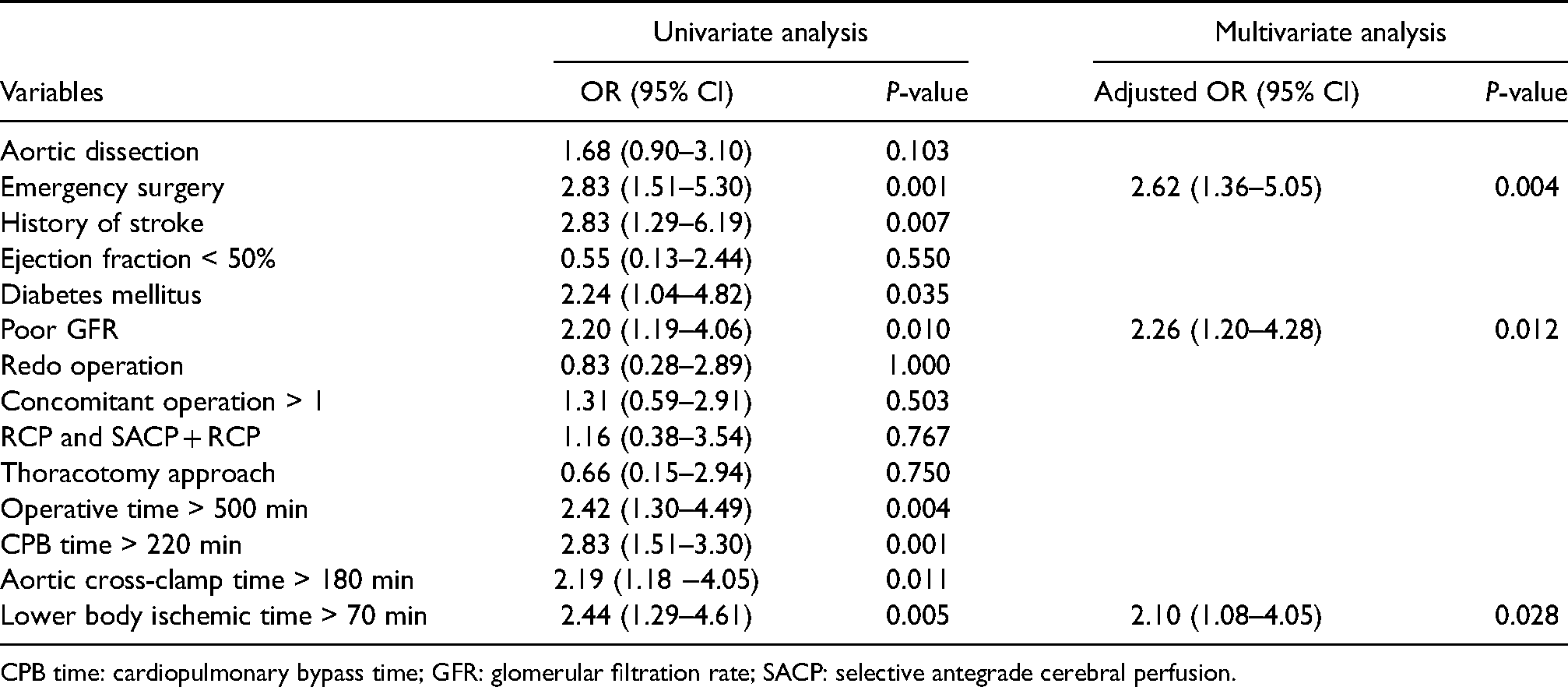
CPB time: cardiopulmonary bypass time; GFR: glomerular filtration rate; SACP: selective antegrade cerebral perfusion.
Forty-eight patients (14.6%) required a second operation caused by bleeding (28 of 48 cases; 8.51%), or postcardiotomy syndrome (3 cases; 0.9%) that needed pericardial drainage and arch branch stent in 3 (0.9%) cases. Other causes of reoperation included gauze packing removal, blood clot removal, CABG due to postoperative myocardial infarction, venovenous extracorporeal membrane oxygenator (ECMO) insertion due to ARDS, and wound dehiscence.
Discussion
Between 2006 and 2019, the number and complexity of TAR cases increased each year (Figures 1 and 2). About 20% of TAR patients had frozen elephant trunk and 10% were combined aortic root surgery. Approximately 42% of patients were operated on under emergency conditions. Our strategy is to avoid complex operations like TAR in emergency conditions and, when it is necessary, we try to limit the extent of the operation as much as possible. For example, in acute type A aortic dissection, ascending and hemiarch replacement is preferable to TAR.
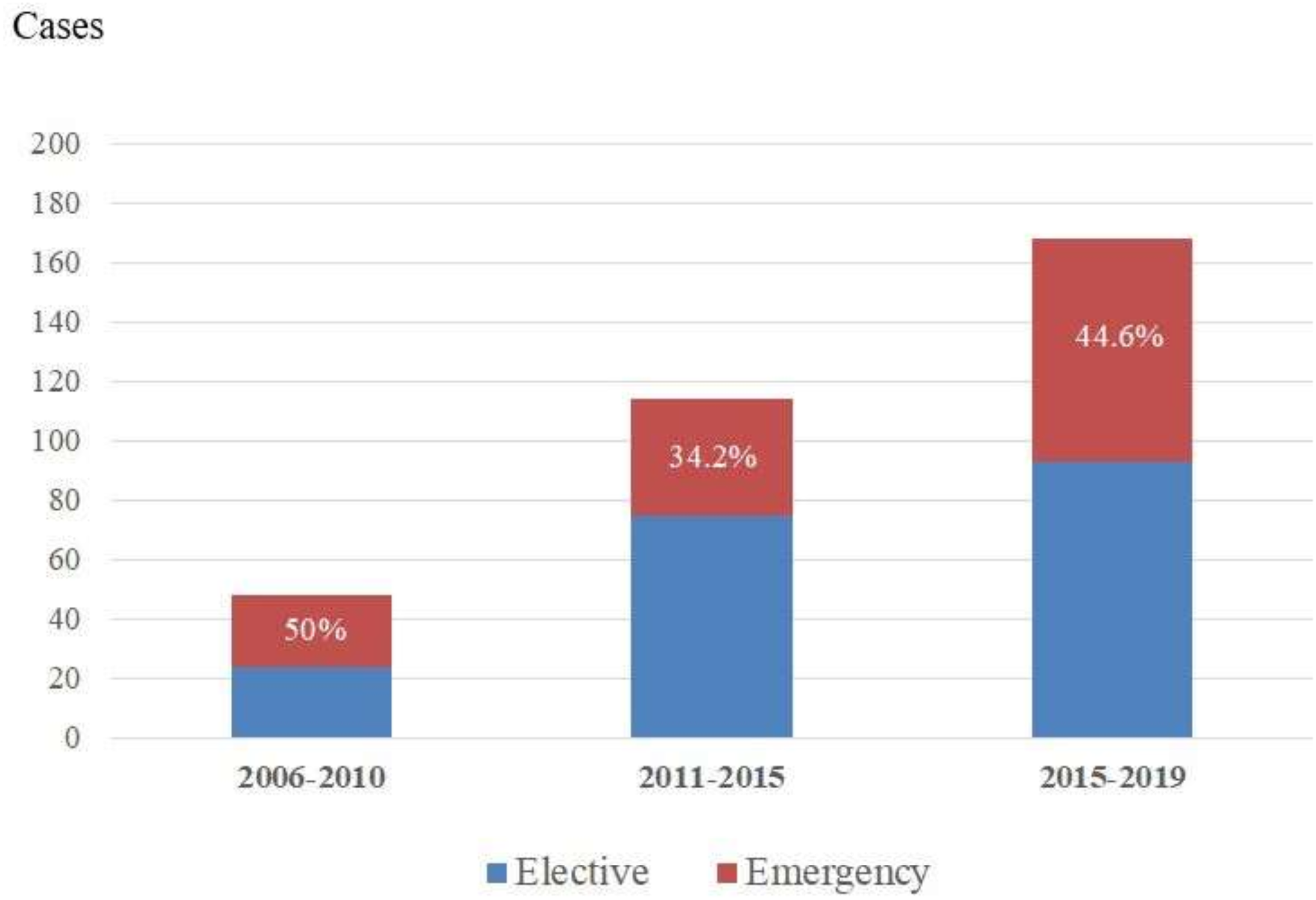
Proportion of emergency versus elective cases during three time periods.
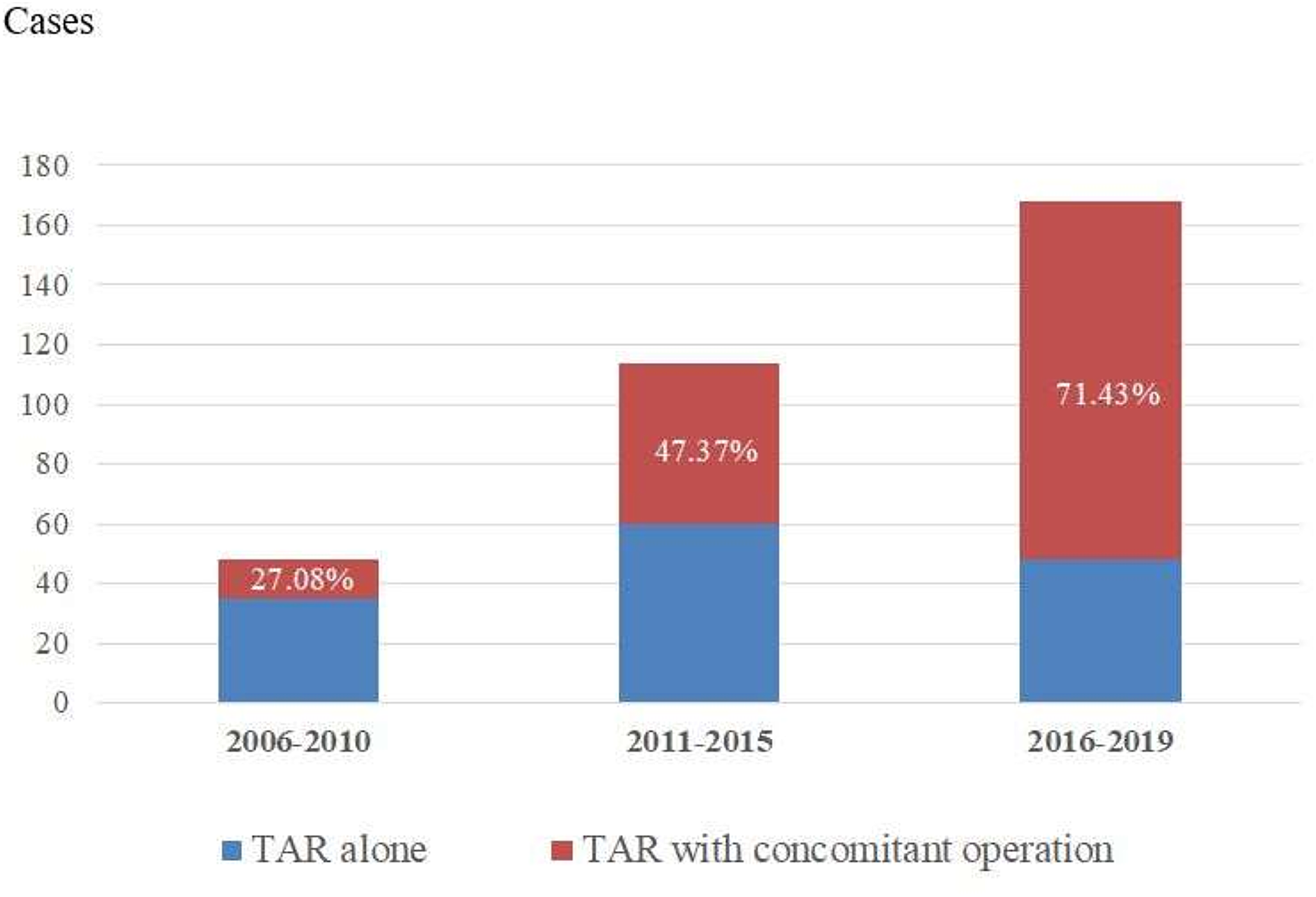
Proportion of concomitant operation during three time periods.
Our 10.9% in-hospital mortality rate was a little higher than in some other reports.1–7,10,13 This could be due to the high proportion of emergent cases and the complexity of these cases. More than half (56.7%) of our patients had a concomitant operation and about 10% of cases were repeated surgeries. The in-hospital mortality rate for elective cases was 7.8%, which is compared with other studies. 3
Patients that underwent two or more concomitant surgeries had higher in-hospital mortality. This could be explained by the increased CPB time and prolonged duration of surgery, as reported by Okita Y. et al. 7 Furthermore, if one of the concomitant operations was a CABG, the OR increased to 4.33 (Table 5), consistent with a report by Tanaka and colleagues. 13 Patients with underlying coronary artery disease have lower cardiac reserves and are more vulnerable to prolonged, complex operations. Patients undergoing emergency surgery had higher mortality as has been reported in several studies.7,10,11,13 Patients in emergency conditions are often more sick than elective cases. Emergencies also often occur after midnight and so the surgical team may be faced with fatigue and staff shortages.
Patients who were > 80 years of age, had a history of stroke, poor preoperative GFR, and thoracotomy approach to surgery had nonsignificant increases in mortality, a finding that was different from other studies.7,13 Unrecognized confounding bias and a small sample size may have contributed to this result.
Neurologic complications are the Achilles’ heel of TAR. We observed higher rates of stroke (PND) than reported by other studies.7,10,11,13 However, nearly 35% of PND patients had ICH, which was different from other reports. PND after TAR is usually due to ischemic stroke that can be explained by embolism or low cerebral blood flow phenomenon.7,15,16 Among ICH patients, 12 cases (57%) had a mean cerebral perfusion pressure (monitored through the radial arteries) during selective antegrade cerebral perfusion (SACP) of > 70 mmHg and/or a > 20% increase of regional brain oxygenation from baseline. We hypothesize that ICH may be caused by high cerebral perfusion pressure or flow through SACP simultaneously with lower body perfusion. This is difficult to control after restarting body circulation if separate pumps are not used for brain perfusion. Overflow of cerebral perfusion as a cause of SDH has been reported. Using a separate pump to precisely control cerebral blood flow during SACP might mitigate postoperative SDH. Another possible explanation is that some patients may have had an undetected preoperative SDH as 5 from a total of 19 patients who had SDH were subacute or acute on top chronic SDH from postoperative imaging. After excluding ICH, the ischemic stroke rate was 8.5%, which is compared to other studies.3,7,11 About the risk factor of PND, the first emergency operation was a significant risk factor for PND (13.8% of cases) that was similar to reports from other studies.17–20 Second, poor preoperative kidney function might be related to atherosclerosis which could cause cerebral embolism. Cerebral embolism is one of the major causes of postoperative stroke in aortic arch surgery. 21 Lastly, prolonged circulatory arrest time > 70 min was also one of the risk factors in our study despite using bilateral SACP. In contrast to other studies, SACP is believed that provides better cerebral protection and provides more time for circulatory arrest which was reported safe up to 90 min. 20 However, there is no solid data about the safe duration of SACP. So from our study, SACP should be applied with caution when circulatory arrest time is longer than 70 min. Acute aortic dissection, underlying diabetes mellitus, and concomitant valve operation have been reported to be risk factors, 22 but we did not find a significant association in this study. Our study has limitations. First, because this was a 14-year retrospective review some of the data were missing. Second, we did not collect some data that are related to PND, such as preoperative imaging, to search for atherosclerotic aorta/shaggy aorta, regional cerebral oxygenation values.
Conclusion
In-hospital mortality after TAR at Siriraj Hospital was compared to international reports. Emergency operation was a risk factor for both mortality and morbidity. Two or more concomitant operations also increased the risk of death, especially in patients who received concomitant CABG. Pulmonary complications, PND, and reoperation were common major morbidities. Emergency surgery, preoperative GFR <60 ml/min/1.73 m2, and aortic cross-clamp time >180 min were important morbidity risk factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research had ethical approved by Siriraj human research protection unit.
Informed consent
This research is retrospective observational study so the consents were omitted.