
Abstract
Background
This retrospective propensity matched study investigated the impact of age on the survival benefit from a second arterial conduit to the left-sided circulation.
Methods
Data for isolated coronary artery bypass surgery were collected from October 2004 to March 2014. All patients with an internal mammary artery graft to left anterior descending artery and additional arterial or venous graft to the circumflex circulation were included. Propensity matching was used to balance co-variates and generate odds of death for each observation. Odds ratios (venous vs. arterial) were charted against age.
Results
The in-hospital mortality rate was 1.12% (arterial) vs. 1.24% (venous) (p = 0.77). The overall 10-year survival was 74.6% (venous) vs. 82.6% (arterial) (p = 0.001). A total of 1226 patients were successfully matched to the venous or arterial (second conduit to circumflex territory after left internal mammary artery to left anterior descending artery) cohorts. Odds ratio for death (venous to arterial) showed a linear decremental overall survival benefit for the second arterial graft to circumflex circulation with increasing age.
Conclusions
The survival benefit of a second arterial graft persists through all age groups with a gradual decline with increasing age over the decades. Elderly patients should not be denied a second arterial graft to the circumflex circulation based on age criterion alone.
Introduction
Arterial grafts have been associated with better survival after coronary artery bypass surgery (CABG). A number of previous observational studies have shown the benefit of two and more arterial grafts on long term survival.1,2 The survival advantage depends on the age of the patient and time variable incremental benefit associated with the second arterial graft. Previous studies have shown that survival benefit of a second arterial graft may be confined to only younger patients. Further, the radial arteries are associated with a very early survival benefit that persists and then dissipates after 10 years. This is different from the survival benefit seen with a second internal thoracic artery which becomes apparent only after six to seven years and seems to persist over the life of the grafts.
There is varying consensus regarding the use of additional arterial grafts among patients over 60 years of age. The Society of Thoracic Surgeons clinical practice guidelines for arterial conduits specify that a second arterial graft should be considered in appropriate patients (Class of Recommendation IIa, Level of Evidence B). 3 Similarly, the NICE, UK guidance remains ambiguous regarding the use of additional arterial grafts in older patients.
This aim of this retrospective propensity matched analysis was to study the impact of age on the survival benefit from a second arterial conduit to the left-sided circulation, to ascertain which patient groups might benefit from additional arterial grafts.
Patients and methods
Data for isolated CABG were retrospectively collected from October 2004 to March 2014 from the hospital database (PATS, Dentrite Clinical Systems Ltd, Henley-on-Thames, UK). Inclusion criteria were (1) an internal mammary artery (IMA) to the left anterior descending artery (LAD), (2) double or triple vessel disease, (3) at least one additional conduit (venous or arterial) to the circumflex circulation, in addition to an IMA graft to left anterior descending artery. Single vessel disease and those with other concomitant procedures were excluded. Approval was obtained from the departmental review committee. Consent for individual use of data was waived off due to the nature of the study and prior approval for use of such data at the time of consent for operation. Long-term survival statistics were collected from NICOR (National Institute of Cardiac Outcomes Research, UK) database (release June 2015) which is linked to Office of National Statistics, UK for mortality data.
Data analysis
Patients were stratified into two groups, those with at least one arterial conduit to the obtuse marginal territory (Group 1) or those with only vein grafts to this territory (Group 2). Baseline demographic characteristics were compared for those with at least one arterial conduit or all venous conduits to the circumflex territory in addition to an arterial graft (left internal mammary artery (LIMA) or right internal mammary artery (RIMA)) to the LAD system. Distributions from each variable were visually inspected and normality was tested by a Shapiro-Wilcoxon W test. Categorical and continuous variables were compared using a χ2 and Mann-Whitney test, respectively. A value of p ≤ 0.05 was considered statistically significant.
Propensity score matching
The propensity score was estimated by logistic regression (p1 for venous and p2 for arterial). Propensity matching was used to balance the co-variates in the nonrandomized, observational data. Covariates used in the propensity match are listed on Supplemental Table 1. The definitions used for these risk factors were as previously described for the calculation of Euroscore (EUROpean System for Cardiac Operative Risk Evaluation) by Roques et al.
4
Treated observations were posteriorly matched in a 1:1 ratio using the nearest-neighbour method (0.2 times caliper width of standard deviation of the propensity score logit). Balance was assured using a Wilcoxon signed-ranks paired test or McNemar’s test for continuous and categorical variables, respectively. The odds of death for each group were calculated p1/(1-p1) for venous and p2/(1-p2) for arterial from the respective propensity scores. Propensities for death calculated for the venous (p1) and arterial (p2) groups using logistic regression for the matched pairs were used to calculate the odds ratio as follows:

Polynomial charts for Odds ratio (odds of death – venous to arterial) against age (abscissa) for the propensity matched pairs were obtained to study the impact of age.
Results
In total, 3995 patients with primary CABG were included over 10 years (2004–2014). These included 1238 patients in Group 1 and 2757 patients in Group 2. The mean follow-up period was 74.5 months (group 1) vs. 64.5 months (group 2) (Figure 1). The in-hospital mortality rate was 1.12% (arterial) vs. 1.24% (venous) (p = 0.77). The overall 10-year survival was 74.6% (venous) vs. 82.6% (arterial) (P = 0.001).
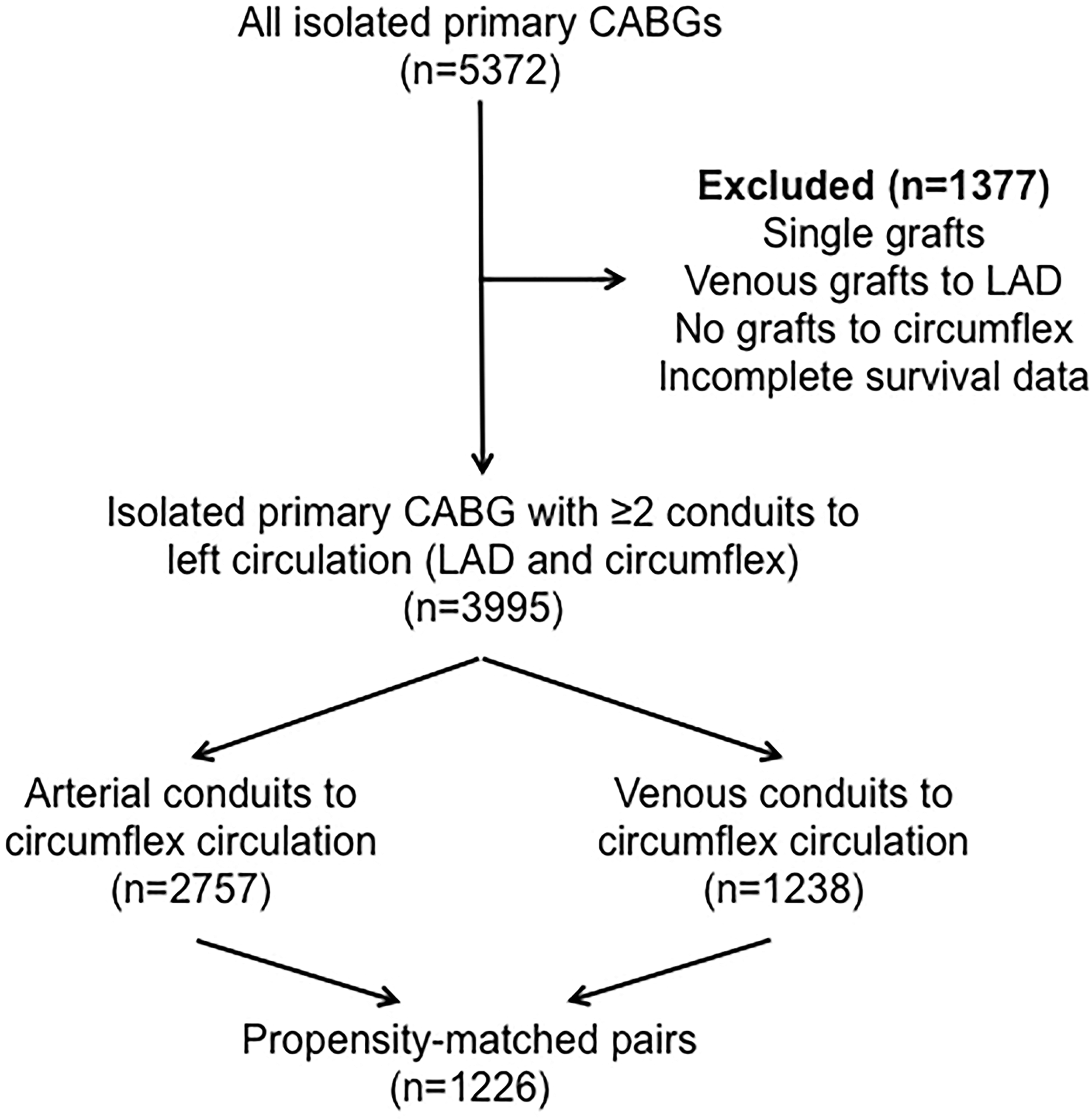
Flow chart for study design. CABG: coronary artery bypass graft, LAD: left anterior descending.
A total of 1226 patients were successfully matched to the venous or arterial (second conduit to circumflex territory after LIMA to LAD) cohorts. The demographic characteristics of the matched cohort and types of conduits per group are given in Supplemental Tables 1 and 2. A second arterial conduit, NYHA Class III–IV, logistic EuroSCORE, diabetes, left ventricular ejection fraction <30%, and previous MI as significant predictors of survival in regression analysis among the matched cohort (Supplemental Table 3).
Odds ratio (odds of death – venous to arterial) plotted against age for the propensity matched pairs (Figure 2) showed a linear decrement in survival benefit for the second arterial graft to circumflex circulation with increasing age. The survival benefit persisted up into the seventh decade of life (OR: 1.09, 95% CI: 1.00–1.17). The survival benefit was present within each of the quartiles of age within our cohort (Figure 3). Additional arterial conduits to the left circulation did not confer an increased survival to a single arterial conduit (p = 0.196) (Figure 4).
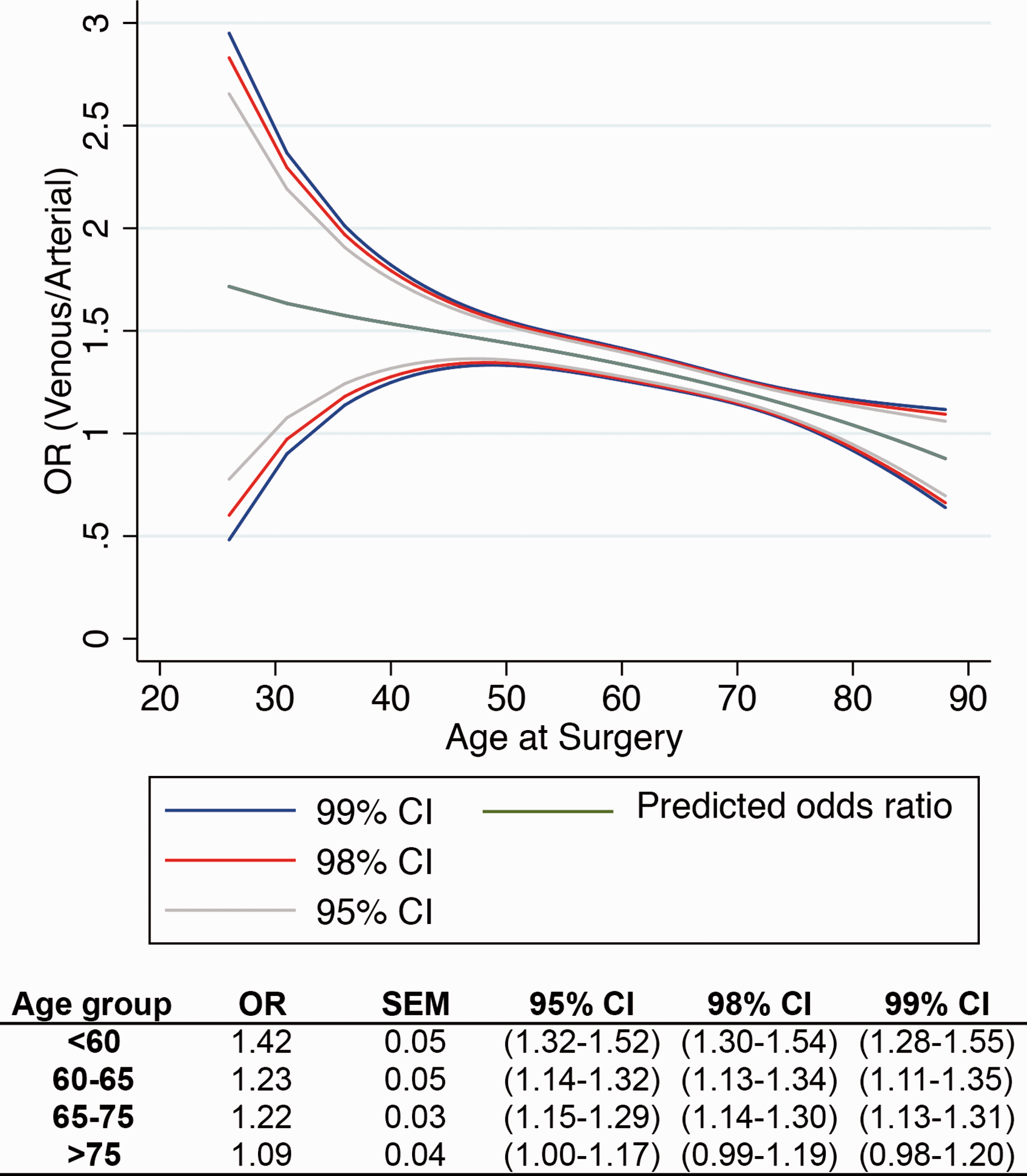
Odds ratio (odds of death venous to arterial) charted against age (abscissa). Table below provides the odds ratios for each age group. OR: odds ratio, CI: confidence interval, SEM: standard error of the mean.
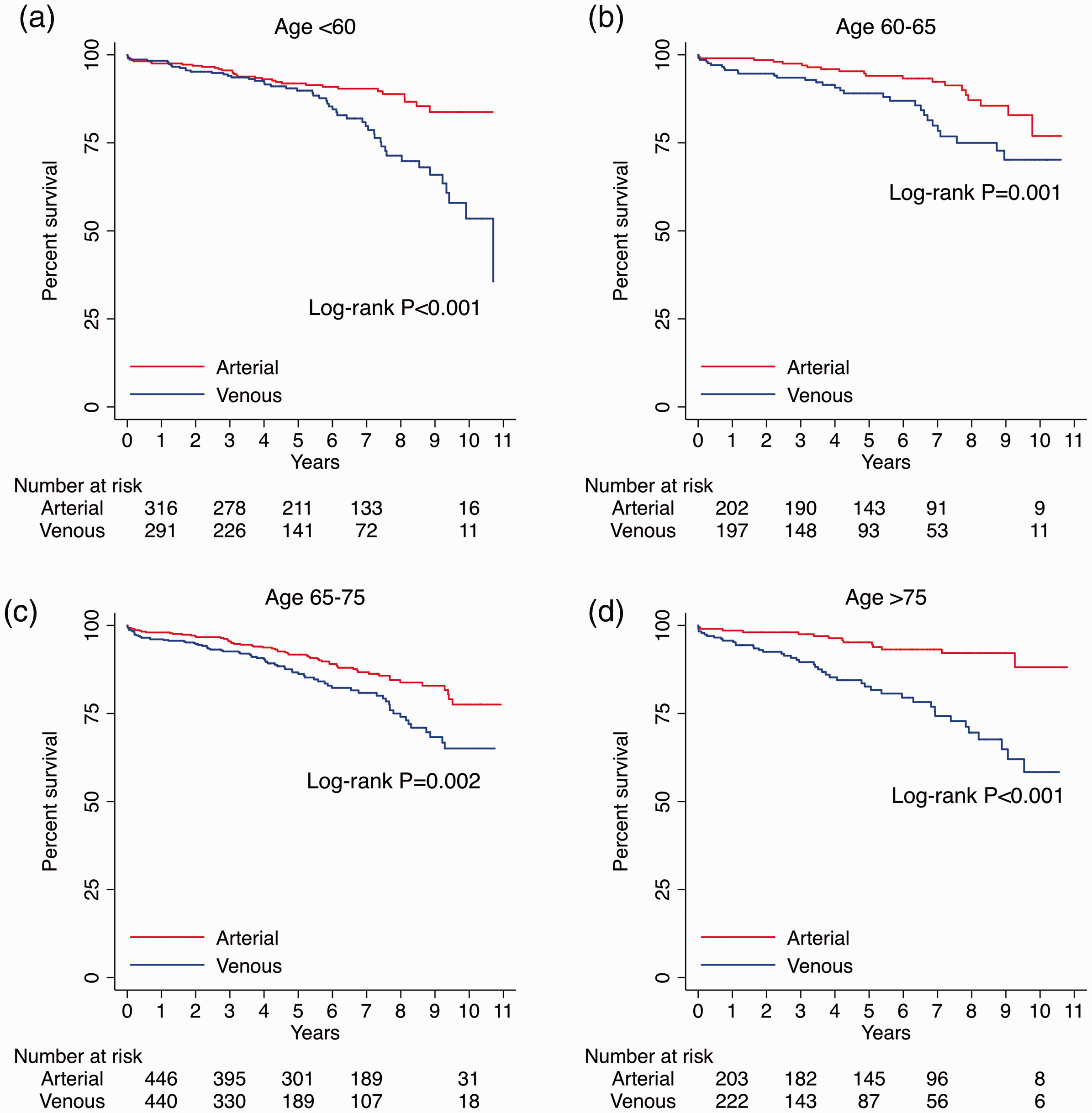
Survival by age group and type of conduit to the left circulation: (a) <60, (b) 60–65, (c) 65–75, and (d) >75 years of age.
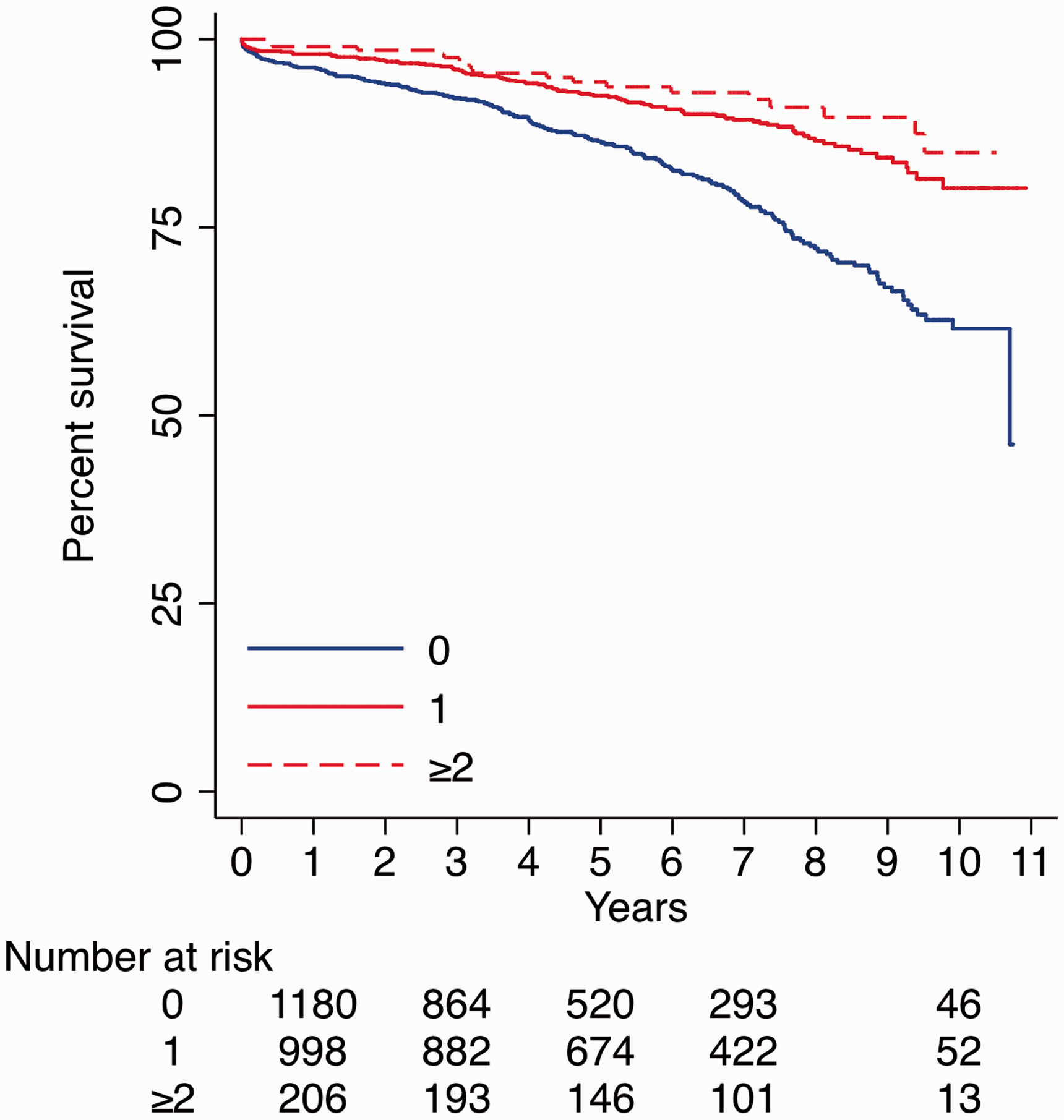
Survival by number of arterial grafts to the left circulation.
Discussion
The present analysis tries to define the age cut off at which the benefits of a second arterial graft are seen. We had earlier shown that the second arterial graft to the circumflex circulation significantly improves both early and late survival, although these benefits did not extend to the use of additional arterial grafts to the right-sided circulation.5,6 Other groups have similarly shown late survival benefits from bilateral internal thoracic arteries and total arterial revascularization in retrospective, observational studies.7,8 ART (Arterial Revascularization Trial) is a randomized control trial that has recently failed to show a survival benefit of bilateral internal thoracic arteries at 1, 5 and 10 years of follow-up.9,10,11 There was however an additional benefit of a radial artery in 20% of the patients in the single internal thoracic artery group. 12 The trial failed to show any differences, even at 10 years. 13 The trial may not have been adequately powered for differences to emerge in the intention-to-treat analysis due to large number of cross overs and high attrition.13,14 Hidden confounders and methodological flaws of randomized controlled trials and forward frequentist analysis may explain some of the discrepancies between the trial results and observational data.15,16 The ROMA trial which is underway may be able to address some of the weaknesses of the ART trial.17,18
There is no consensus on the age at which the survival benefits of additional arterial grafting diminish. Venous grafts have been shown to undergo late accelerated degeneration from the third to fourth year onwards due to progressive atherosclerosis.11,19–21 The potential survival benefits of a second arterial graft are possibly from improved patency compared to venous grafts. Theoretically at least, patient cohorts with a life expectancy of at last seven to eight years should potentially benefit from absence of a failed second venous graft-related morbidity and mortality. It is also likely for these reasons that any potential survival benefits, even in the young, are unlikely to be realized before this late accelerated inflection point in vein graft patency at four to five years. Similar considerations may apply to further arterial grafts to the circumflex and right coronary circulations where larger cohorts and longer studies in more elderly age groups may be needed to demonstrate any further benefits. 22 As seen in this analysis, these survival benefits are much greater in younger patients but persist in other age groups albeit with progressively diminishing magnitudes.
Kurlansky et al. found significant survival benefit with bilateral IMA (BIMA) in all groups <65 years, 65–70, and >65 years in their retrospective analysis of 4503 consecutive isolated coronary artery bypass grafting operations (SIMA, n = 2340 and BIMA, n = 2163). 23 Actuarial curves after 23,593 patient-years of follow-up demonstrated improved long-term survival for BIMA vs. SIMA patients at 12 years (51.0 ± 1.5% vs. 39.0 ± 1.5%) and at 24 years (3.5 ± 0.7% vs. 4.5 ± 0.7%; p < 0.001). Similarly, in matched groups of patients age 70 and older, overall survival was also enhanced with BIMA grafting (p < 0.005). In contrast, the APPROACH investigators in the Canadian cardiovascular registry of 5601 patients (mean follow-up 7.1 years) could not show any statistically significant benefits of BIMA grafting in patients older than 70 years (HR, 0.87; 95% CI, 0.69 to 1.08; p = 0.2). 24 In an older study (1992–2005), Mohammadi et al. similarly found age to be a significant covariate in their statistical model. 25 The cardiac-related survival benefit with BIMA was superior to that of SIMA grafting up to 60 years of age. This benefit decreased over time. Compared to only vein grafts, use of a single ITA was superior for cardiac-related survival in all age groups, including octogenarians.
Benedetto et al. used spline analysis to demonstrate the age cut off for benefit from additional arterial grafts in their single institution study. 26 Their analysis was confined to radial artery as a second graft as opposed to saphenous vein grafts. Most of their patients had conventional on-pump CABG. They however did not specify if the radial artery was used as a second conduit to the right or the left coronary circulation (86% had obtuse marginal grafts and 73% had right coronary grafts in the unmatched radial artery group). The benefit was maximum in patients aged 60 years or younger (upper limit of 95% CI, <1). The survival advantage conferred by radial artery use gradually declined with increasing age, and it was no longer present beyond 70 years of age.
The use of BIMA for left-sided grafts in completely an-aortic off-pump technique has previously been shown to confer a small survival advantage especially in high-risk and elderly patients possibly from prevention of adverse neurological sequelae.27,28
The age range for the ‘elderly’ has gradually increased as the results of cardiac surgery have improved over the last few decades. The average life expectancy has increased in the developed nation and the demographics of patients referred for CABG has changed over the last few decades. An increasing number of ‘elderly’ patients now have a longer expectant life ahead of them after CABG. Our matched data show that these survival benefits gradually diminish with increasing age but they are seen across all age groups up to 80 years of age. Elderly patients are also likely to benefit and should not be denied a second arterial graft to circumflex circulation based on sole considerations of age.
Limitations
This is a retrospective single center study. The nature of grafts and their patency were not examined for any of the left- or right-sided grafts. The results would need to be interpreted cautiously due to the small number of cases at risk in the cohorts. Larger cohorts and longer follow-up is required to further substantiate these findings.
Conclusions
The survival benefit of an additional arterial graft to the circumflex circulation is seen in all age groups. Elderly patients should not be denied the benefits of second arterial grafts based on age criteria alone.
Supplemental Material
sj-pdf-1-aan-10.1177_0218492321997077 - Supplemental material for Survival benefit from a second arterial conduit to the circumflex circulation persists in elderly after coronary artery bypass surgery
Supplemental material, sj-pdf-1-aan-10.1177_0218492321997077 for Survival benefit from a second arterial conduit to the circumflex circulation persists in elderly after coronary artery bypass surgery by Suvitesh Luthra, Miguel M Leiva-Juárez Pietro G Malvindi, John S Billing and Sunil K Ohri in Asian Cardiovascular & Thoracic Annals
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.