
Abstract
Background
The revascularisation strategy for concomitant carotid and coronary disease is unknown. Simultaneous or stage coronary artery stenting and carotid endarterectomy are the most common revascularisation approach in the CABG population. This study aimed to evaluate long-term results after simultaneous carotid artery stenting or carotid endarterectomy in patients who underwent coronary artery bypass surgery.
Methods
This is a prospective cohort non-randomised single-institution study. During the period from 2012 to 2015, sixty consecutive patients (65.9 ± 7.41 mean) underwent simultaneous carotid artery stenting and coronary artery bypass surgery (n = 30) or simultaneous carotid endarterectomy and coronary artery bypass surgery (n = 30). The primary endpoints were short- and long-term rates of adverse events (transient ischemic attack, stroke, myocardial infarction, and death). The mean follow-up was 62.05 ± 11.12 months.
Results
In-hospital mortality was insignificantly higher in the carotid endarterectomy, and coronary artery bypass surgery group (6.6% vs. 0%), the rate of stroke and myocardial infarction was similar (13.3% and 0% in the carotid endarterectomy and coronary artery bypass surgery group vs. 6.6% and 3.3% in the carotid artery stenting and coronary artery bypass surgery group, respectively). The intensive care unit readmission was significantly higher in the surgical revascularisation approach; it was an independent predictor of hospital mortality. The overall mortality during the follow-up period was 14.28% in both groups. Freedom of the composite adverse outcomes (stroke, myocardial infarction, and death) was 78.55%.
Conclusion
Comparing two revascularisation strategies is not straightforward due to different anatomical indications for carotid artery stenting and endarterectomy. We consider that each technique has an essential role in carotid revascularisation. Good selection of patients, according to indications, contributes to satisfactory short- and long-term results.
Introduction
The carotid artery (CA) disease significantly increases perioperative morbidity and mortality in patients who underwent coronary artery bypass surgery (CABG). 1 Concomitant carotid and coronary diseases were revealed in 8–14% of patients. 2 Untreated CA disease increased the rate of cerebrovascular events after the CABG procedure.3,4 The standard surgical treatment of carotid disease is carotid endarterectomy (CEA). Procedures could be performed as a staged (CEA followed by CABG) or simultaneous (CEA and CABG at the same time) approach. Surgical revascularisation reduces stroke incidence but increases trauma and adverse events during the perioperative period. 5 In an attempt to reduce postoperative complications and decrease perioperative morbidity, carotid artery stenting (CAS) was implemented as a less invasive procedure and an alternative approach to traditional CEA.2,6 The short-term results of major adverse events (death, stroke, and myocardial infarction [MI]) were similar for staged CAS, and CEA performed concomitantly with cardiac surgery. 7 The simultaneous CAS and open-heart surgery (hybrid procedures) showed satisfactory short- and long-term results in patients with concomitant carotid and coronary diseases.1,5,8 Our study analyzed the feasibility and safety of CAS or CEA simultaneously performed with the CABG procedure in patients with significant carotid and coronary disease.
Patients and methods
A prospective study was carried out in a single institution from April 2012 to February 2015. Before entering the study, patients signed informed consent. The study included sixty patients with severe concomitant coronary and carotid disease who underwent simultaneous revascularisation procedures.
Inclusion criteria
Significant CA disease in patients who underwent CABG. All patients admitted to our Institute due to ischemic heart disease were examined. The CA's colour duplex scan was performed in patients with a history of cerebrovascular events or auscultatory registered carotid bruit. Asymptomatic carotid disease with a stenotic grade of more than 80% (the patients were considered asymptomatic if they did not have a cerebrovascular event six months before the procedure) and symptomatic patients (the patients with a confirmed diagnosis of stroke and transient ischemic attack [TIA] in history were considered symptomatic) with carotid stenosis more than 50% were indicated for revascularisation. Patients indicated for CA treatment were evaluated by computed tomographic (CT) angiography due to anatomical analysis of the ascending aorta, supra-aortic vessels, cerebral circulation and carotid plaque characteristics.
Exclusion criteria
REDO cardiac and carotid surgery, heart valve surgery, ascending aorta aneurysm and aortic dissection surgery, intolerance to aspirin and clopidogrel; ischemic stroke within six weeks; severe renal impairment (serum creatinine >300 µmol/L); the presence of intraluminal CA thrombus; emergent and urgent patients; patients who underwent to coronary angioplasty; and CA disease unsuitable for CAS or CEA.
The radiologist and vascular and cardiac surgeons were giving the final approval regarding the anatomical suitability of the carotid lesion for stenting or endarterectomy.
Unfavourable characteristics for CAS included: low bifurcation/short common carotid artery (CCA), tortuous CCA, diseased CCA, diseased/occluded external CA, severe aortic arch calcification, significant disease at the origin of the great vessels, type III arch, bovine arch, pinhole stenosis, circumferential calcification of CA (>2/3rd the circumference of the vessel at the lesion site), angulated internal CA (ICA) origin, and angulated distal ICA.
Unfavourable characteristics for CEA included: total occlusion of CA, a lesion that extends above C2, prior irradiation of the neck, prior neck operation, CA tandem lesion, and restenosis of CA. Cardiac catheterisation and echocardiography examination are performed in all patients preoperatively.
Indications for the CABG procedure were left main disease, a significant multivessel coronary disease with circumferential lumen reduction of more than 50%, or functional flow reserved test value less than 0.75 for borderline stenosis. The flow chart of the clinical protocol is described in Figure 1.
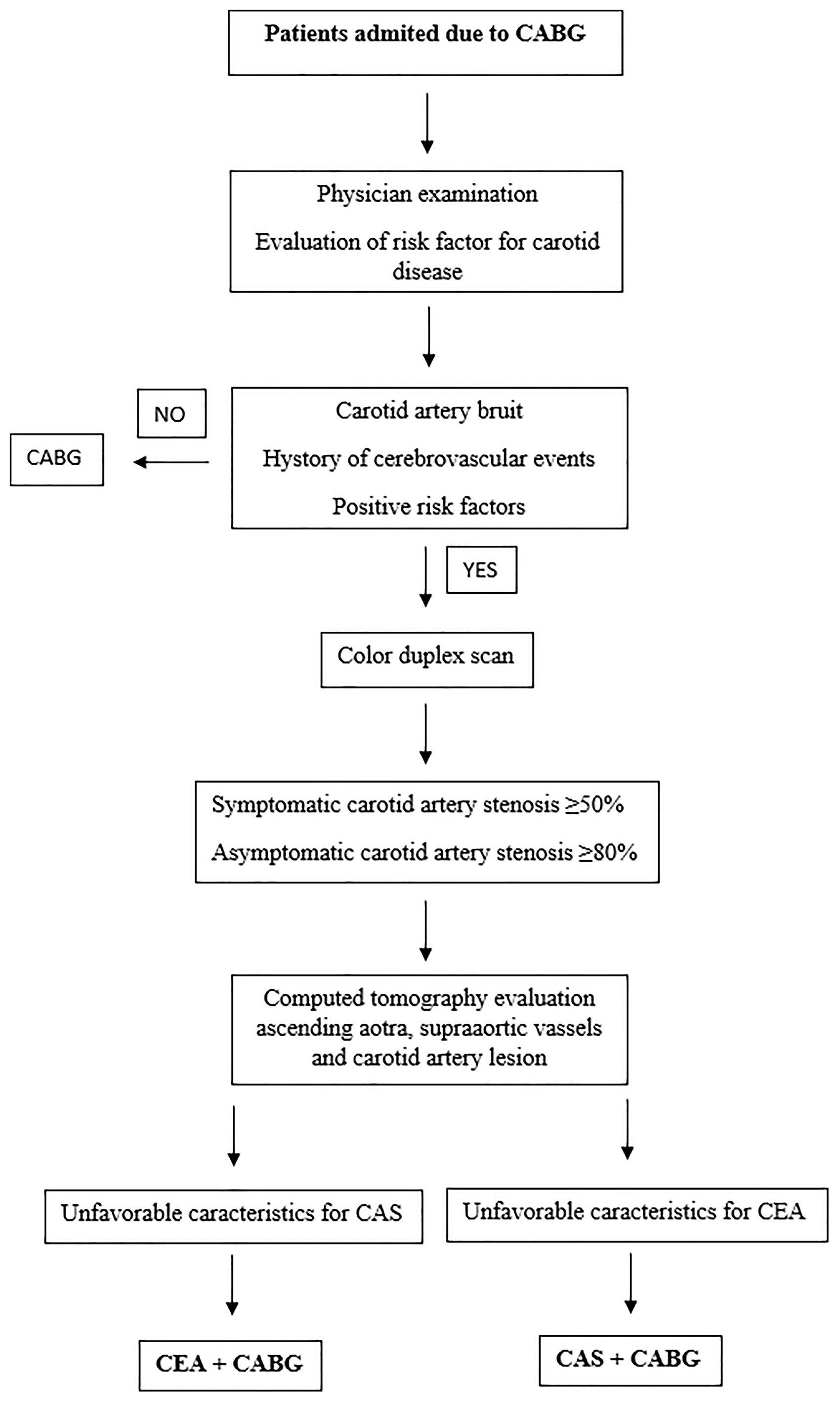
The flow chart shows the treatment algorithm for patients with carotid and coronary diseases. (CAS, carotid artery stenting; CEA, carotid endarterectomy; CABG: coronary artery bypass grafting.).
The local institutional ethics committee approved the study's protocol, and all the patients provided written informed consent (Document number 1407, approved date 3 April 2012).
CAS procedure protocol
CAS is performed in the catheterisation laboratory by an interventional radiologist under local anaesthesia before cardiac procedures. CAS and CABG procedures were performed on the same day. After the procedure, neurological status was evaluated and eventuality proceeds with CABG. All patients received 100 mg of aspirin starting two days before the procedure. The percutaneous transfemoral approach was used. Heparin was administered at a dose of 1 mg/kg. In all of the patients, distal cerebral protection device was used. The distal cerebral protection Emboshield system (Abbot Vascular) was used in all the patients. Predilatation of the stenosis was done before placement and final stent expansion. Balloon expandable stents were deployed into the common CA. In our series, three different types of carotid stents were used: Xact (Abbot Vascular), Cristallo (Invatec), and Carotid WALLSTENT (Boston Scientific). The CAS results were considered successful if residual stenosis was ≤20% and if complications such as stroke or TIA did not occur. Within 1 h of completion of the procedure, patients were transferred to the cardiac surgery operating theatre. During that period, patients received intravenous heparin via infusion pump according to the activated clotting time (ACT) value, which was measured on an hourly basis. The aim was to maintain ACT for approximately 200 s.
CEA procedure protocol
The vascular team performed CEA just before myocardial revascularisation during the same deep general anaesthesia. In the case of bilateral disease, an intervention was done on the CA with a more critical lesion. Antiplatelet therapy was not given preoperatively, and a heparin bolus (5000 IU) was given immediately before the procedure. All patients underwent eversion endarterectomy without the shunt; the artery's proximal and distal part was clamped. Wound closure was done by the end of the cardiac intervention. CAS or endarterectomy was performed simultaneously with myocardial revascularisation. There was not staged procedure.
CABG protocol
Cardiac surgery procedures were performed using cardiopulmonary bypass in general anaesthesia. The left internal mammary artery, radial artery, and great saphenous vein were used as a conduit for revascularisation. The surgery was done under general heparinisation (aiming for the ACT of >480 s) using extracorporeal circulation in mild hypothermia and using crystalloid or blood cardioplegic solution. We tried to keep mean pressure during cardio-pulmonary bypass on a higher level due to carotid disease. After completing the intervention and coming off the cardiopulmonary bypass, a complete reversal of heparin was done by infusion of full-dose protamine and antifibrinolytic agent.
Periprocedural pharmacological protocol
Dual antiplatelet therapy was administered early after the procedure. Clopidogrel 300 mg as a loading dose, followed by 75 mg/day for six months postoperatively, was started in the intensive care unit (ICU) via nasogastric tube 6 h after the surgical procedure. Aspirin 100 mg/day was continued from the first morning after the procedure for the remainder of the patient life.
Endpoints and follow-up
The primary endpoints were major events (TIA, stroke, MI, and death) during hospitalisation and long-term periods. The stroke was defined as a new focal neurologic deficit that persisted >24 h. TIA was diagnosed if the duration of symptoms lasted <24 h. Neurologist and CT scan examination evaluated patients with neurological events. The diagnosis of MI was based on the presence of increased cardiac-specific enzymes more than twice the upper limit of regular, new Q waves on the electrocardiogram (ECG), new regional wall motions abnormality on transesophageal echocardiogram or chest pain duration more than 30 min.
Follow-up was performed by telephone interview and clinical examination (CA colour doppler scan evaluating the treated and contralateral CA, ECG, and physical examination).
Statistical analysis
Descriptive statistics included mean values, standard deviations, median, and interquartile range of monitored parameters. Besides, the difference in the distribution of specific characteristics among the groups was discovered using χ2 or Fisher's test The normality of the distribution of numerical variables was examined by applying the Shapiro–Wilk and Kolmogorov–Smirnov tests. The comparison between the groups was made using the Student t test, Mann–Whitney test, and Kruskal–Wallis test Binominal and multinomial logistic regression analyses were utilised to define the relationship between the dependent binary variable and independent variables. Kaplan–Meier curve was used to estimate the survival rate and major events during the follow-up period. All statistical methods were significant if the p-value was ≤0.05. Data processing was done using statistical software SPSS 25.0 for Windows 10.
Results
Our study included 60 patients divided into two groups. Simultaneous CEA and CABG were performed in 30 patients, the other group in whom the hybrid procedure was performed included 30 patients. Statistical analysis showed that groups were homogenous, except in the degree of CA stenosis and bilateral CA disease involvement. The preoperative history of stroke was registered in 18.3% of patients. The preoperative characteristics of the patients are shown in Table 1. CEA was performed significantly more in patients with bilateral carotid disease
Preoperative characteristics of patients.
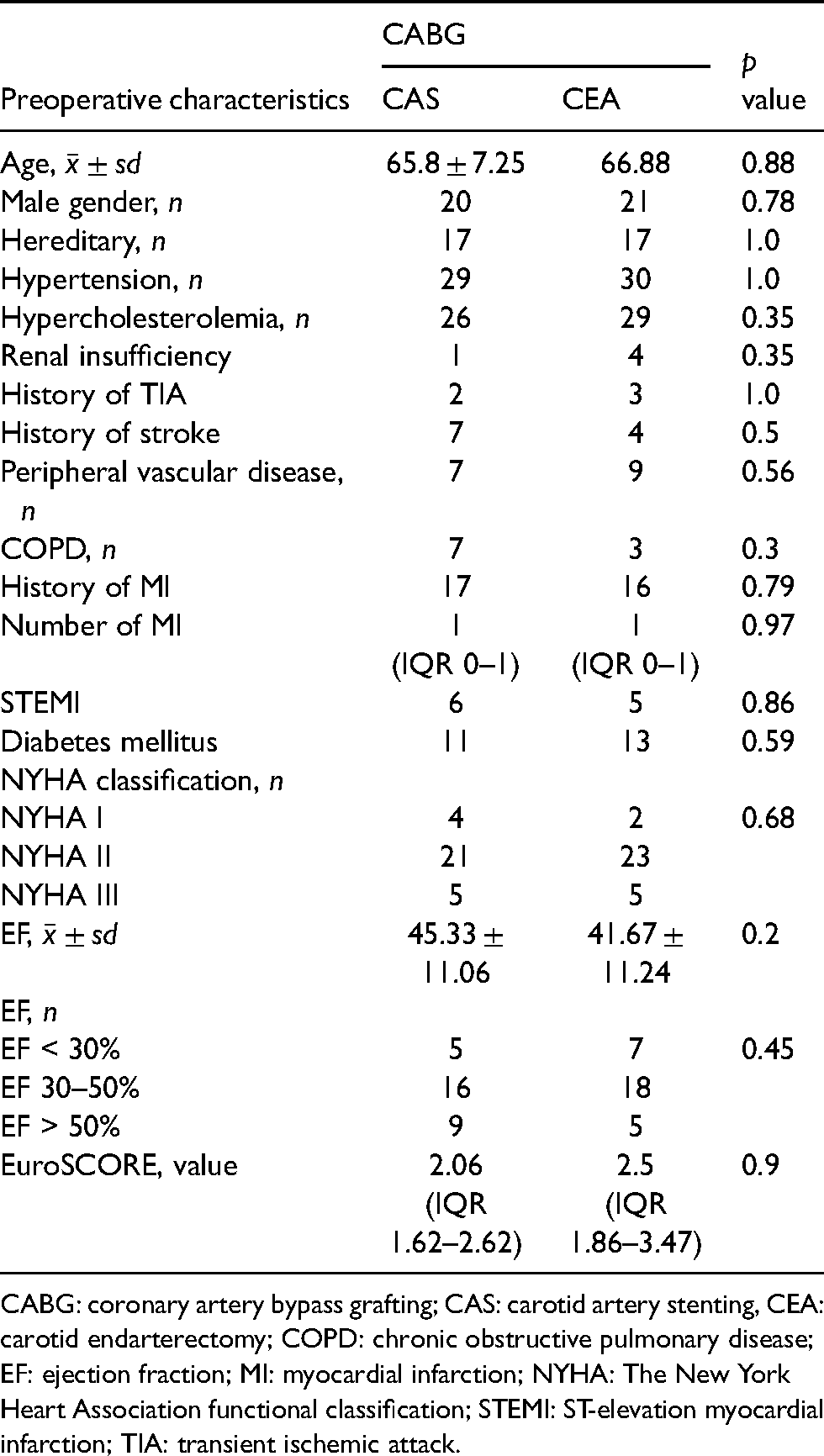
CABG: coronary artery bypass grafting; CAS: carotid artery stenting, CEA: carotid endarterectomy; COPD: chronic obstructive pulmonary disease; EF: ejection fraction; MI: myocardial infarction; NYHA: The New York Heart Association functional classification; STEMI: ST-elevation myocardial infarction; TIA: transient ischemic attack.
Diagnostic characteristics of patients.
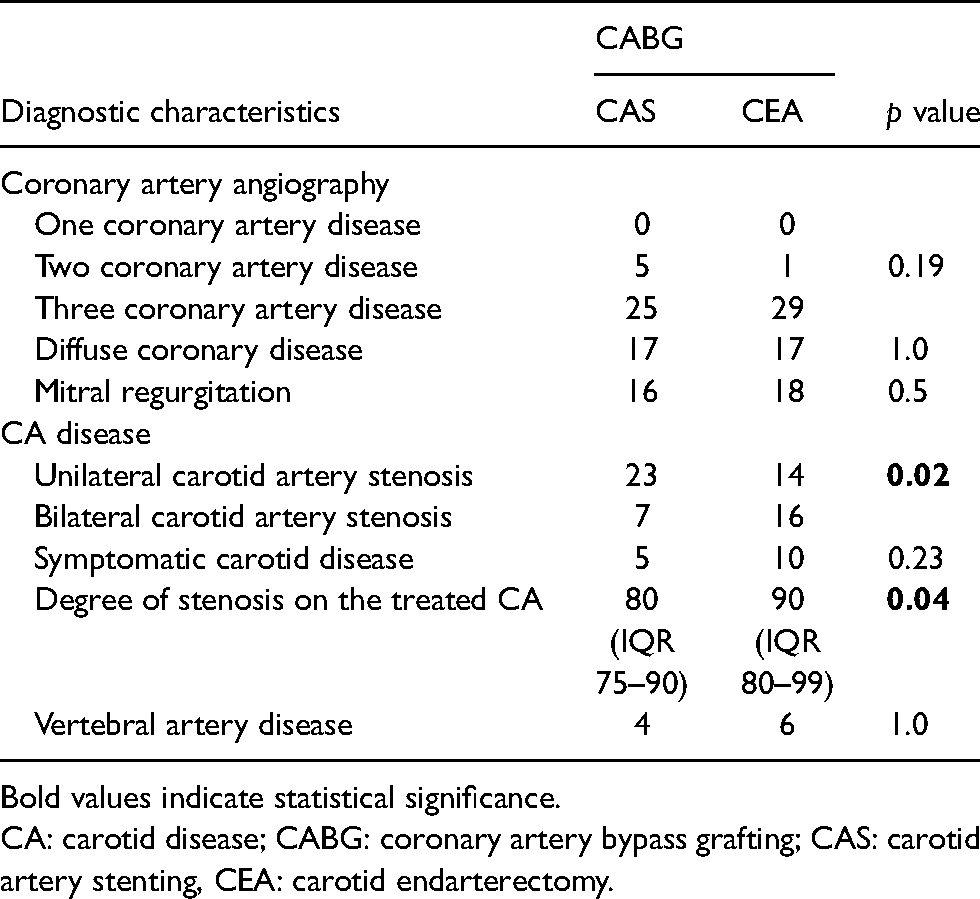
Bold values indicate statistical significance.
CA: carotid disease; CABG: coronary artery bypass grafting; CAS: carotid artery stenting, CEA: carotid endarterectomy.
Intraoperative characteristics of patients.
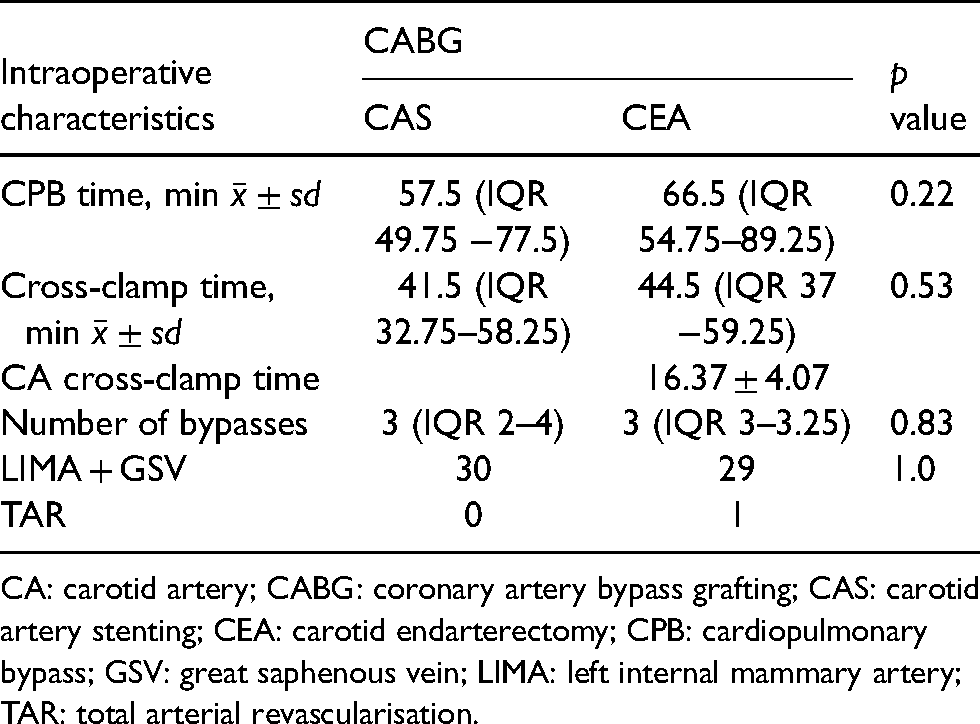
CA: carotid artery; CABG: coronary artery bypass grafting; CAS: carotid artery stenting; CEA: carotid endarterectomy; CPB: cardiopulmonary bypass; GSV: great saphenous vein; LIMA: left internal mammary artery; TAR: total arterial revascularisation.
Perioperative characteristics of patients.
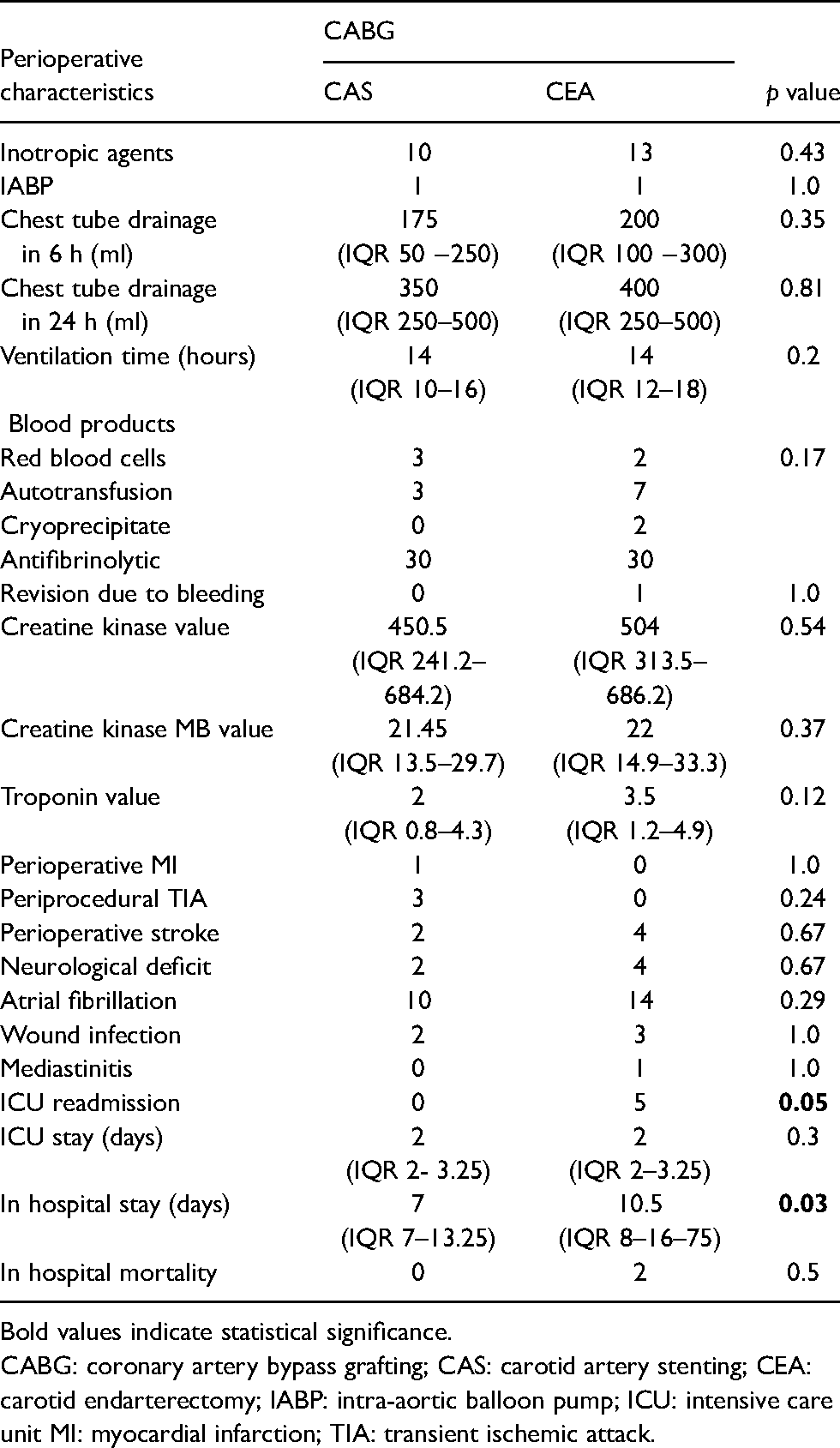
Bold values indicate statistical significance.
CABG: coronary artery bypass grafting; CAS: carotid artery stenting; CEA: carotid endarterectomy; IABP: intra-aortic balloon pump; ICU: intensive care unit MI: myocardial infarction; TIA: transient ischemic attack.
The stroke did not register during the CAS procedure. On the other side, the stroke rate was insignificantly higher in the CEA and CABG groups (4/30; p = 0.67). Three patients in this group had contralateral CA occlusion and postoperative contralateral ischemic stroke.
The ICU readmission due to worsening conditions was higher in the CEA and CABG groups (p = 0.05). The most common reasons for ICU readmission were cardiac decompensation, respiratory failure, and multiorgan failure. Two patients died during hospitalisation in CEA and CABG groups (one case due to a fatal stroke and the second due to respiratory failure). Fatal outcome was more frequently described in patients with symptomatic CA disease (p = 0.5). In-hospital mortality did not register in the hybrid group. Multinomial logistic regression showed that readmission in the ICU was an independent risk factor for a fatal outcome (OR 21.24, 95% CI 0.9–497.59, p = 0.05).
The follow-up period was 62.05 ± 11.12 months. One patient in the CEA and CABG groups had MI (p = 1.0). TIA did not register during the follow-up period, but the stroke was registered in three patients, two in hybrid and one in CEA and CABG groups (p = 0.6). In each group, four patients died. In the hybrid group, two patients died due to fatal stroke, and one patient had MI infarction, with consequently heart decompensation a fatal outcome. One patient died due to renal insufficiency. In the CEA and CABG groups, one patient died due to a fatal stroke. Heart failure with a fatal outcome was registered in one patient. Two patients died due to other reasons (Figure 2A and B).
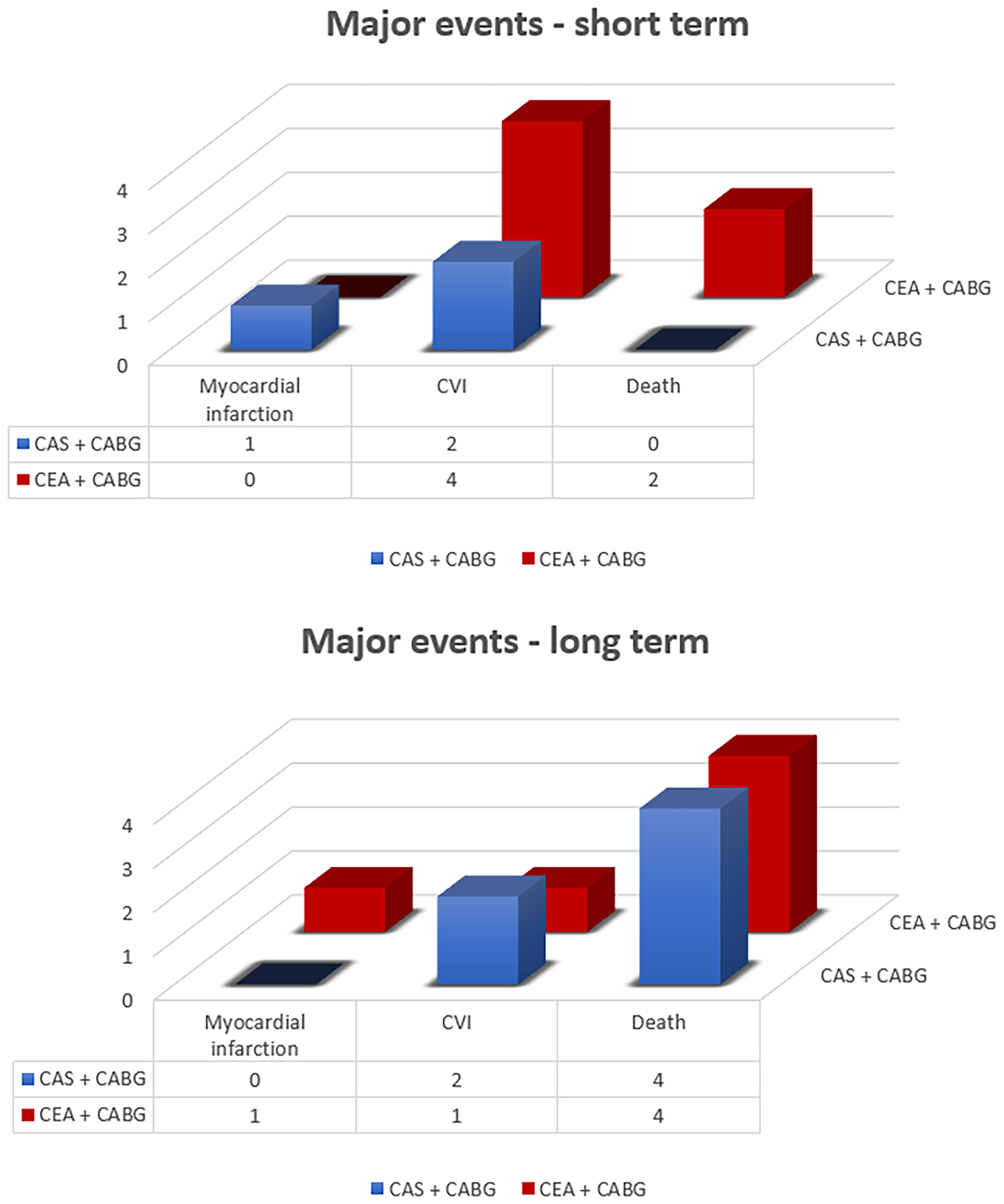
The absolute number of adverse events in both groups of patients. A) Short-term period. B) Long-term follow-up period.
An equal number of adverse events was registered (5/28 in hybrid; 5/28 in CEA + CABG). The onset of the major events in the follow-up period was shown in the Kaplan–Meier curve (Figure 3). Three patients in the CEA and CABG groups had a surgical intervention on the contralateral CA. The long-term survival rate was 85.7%. Two patients were lost during follow-up, which was 96% completed.
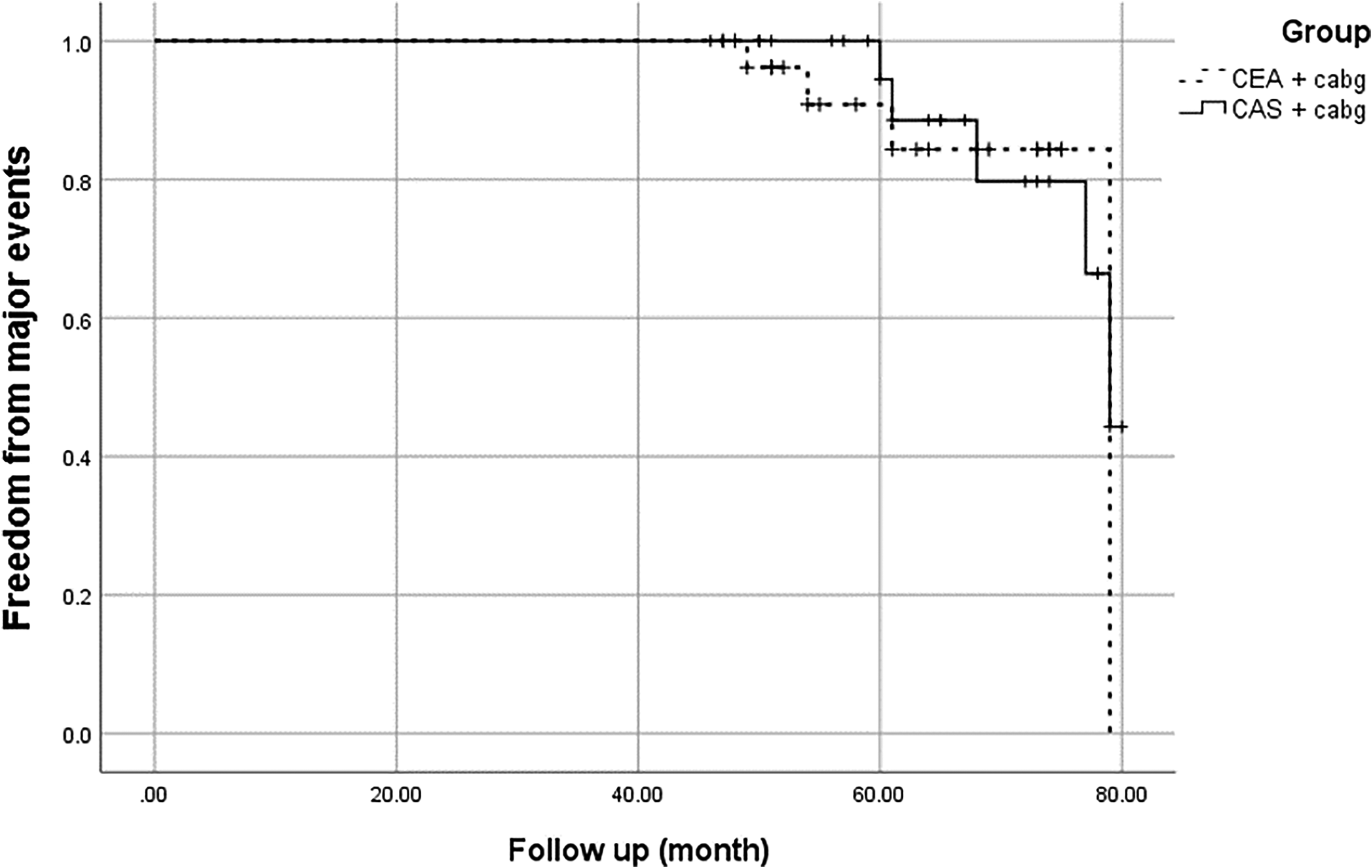
Kaplan–Meier curve represented freedom from major events during follow-up period in both groups.
Discussion
The concomitant carotid and coronary disease affect about 2.4–14% of the population who underwent to CABG procedure. 9 Significant CA disease increased the hazard of periprocedural stroke in the CABG population with a rate of events from 3% in patients with unilateral asymptomatic disease to 7–11% in patients with carotid occlusion.1,2 The most common reason for ischemic injury was hypoperfusion at the time of operation. The embolic particles (thrombi arising from unstable aortic or carotid plaque, hypercoagulation in the heart–lung machine, or gaseous due to air existing in circulation) could produce a different stage of cerebral damage. The reason for postoperative stroke in 30% of cases was a significant carotid disease; in these patients, the mortality rate was very high (21%).2,9,10 The revascularisation strategy remains controversial, especially for asymptomatic CA disease. There are two revascularisation options: CEA could be performed at the same time with CABG (simultaneous) or before CABG procedure (staged), and CAS could be performed simultaneous (hybrid) or staged with CABG procedure.2,6,7,9,11 The revascularisation in patients with high-grade carotid stenosis by stage or simultaneous with the CABG procedure is recommended to reduce the incidence of cerebrovascular events.12,13 Giannopoulos et al. presented a hybrid method as a satisfying alternative to simultaneous surgical revascularisation, especially in high-risk patients. 9 The CEA and CABG staged procedure decreased cerebrovascular events but increased the chance of myocardial events. The simultaneous approach had a lower incidence of both complications. 14 The major perioperative events (stroke, TIA, MI, and death) in the two groups were similar. In the CEA and CABG groups, the stroke rate was insignificantly higher than in the hybrid group; on the other side, the hybrid group had a higher TIA rate after the procedure. Feldman et al. presented similar rates for in-hospital stroke in the CEA + CABG and CAS + CABG (6). Naylor et al. showed a high cumulative risk of death, stroke, or MI (10–12%) in patients who underwent a concomitant surgical procedure. The same author demonstrated significantly higher mortality and stroke rate for combined CEA–CABG than a staged approach. 13 The periprocedural incidence of stroke was 13.3% in our study's simultaneous CEA and CABG. The fatal outcome was 6.6% during hospitalisation. The history of stroke was identified as a predictor of worse perioperative neurological outcomes. 15 Hybrid procedures decreased surgical procedures’ time and trauma, thus reducing cofactors known to increase morbidity and mortality. 2 Simultaneous and staged CAS and CABG represent a less invasive option for the treatment of concomitant carotid and coronary diseases. 16 Van der Heyden et al. analysed CAS and cardiac surgery results and presented 4.8% of major stroke and all deaths, a risk of 2% of MI, and 6.7% for composite outcomes (death, stroke, and MI). 17 We analysed the hybrid group results in our study and presented 3.3% of perioperative MI, 6.6% of periprocedural CVI, and all deaths.
In our study, patients were readmitted to ICU due to worsening conditions after the operation frequently in the CEA and CABG groups. It was an independent risk factor for a fatal outcome during hospitalisation. Also, the in-hospital stay was longer in the surgical approach in our research. These results confirmed that simultaneous surgical treatment increases trauma and the prevalence of adverse outcomes during the perioperative period.2,5,12,16
Sardar et al., in the meta-analysis, presented five years follow-up of patients after CAS and CEA. Overall cerebrovascular events were significantly higher in the CAS group. The associated risk of long-term mortality was similar between the two groups. 18 Micovic et al. showed a higher incidence of stroke and death during long-term follow-up in the older population (>68 years). 19 At five years, 26.3% of patients archive composite endpoint (dead, stroke, and MI), 21.7% of patients died, 5.7% stroke was registered, and 1.4% suffered from MI. 1 The overall survival in the five-year follow-up was 90 ± 3.4% presented by Chiariello et al. 5 Our study's long-term results showed equal composite outcomes between CAS and CABG versus CEA and CABG groups (21.42%). The stroke rate was insignificantly higher in the hybrid group (7.14%) versus the surgical approach (3.57%). Survival at five years was 85.72% in both groups.
The postprocedural rates of stroke were similar between CAS and CEA during ten years (6.9, 95% CI 4.4–9.7 vs. 5.6, 95% CI 3.7–7.6, respectively). The ten-year risk of death did not differ significantly between the two groups. 20 Significantly better ten years survival in the CEA was presented by Columbo et al. 21 The CAS and CABG strategy was used in higher-risk patients and was associated with a lower risk of mortality and a higher risk of stroke. 6 The ten-year survival was 81 ± 10% in the concomitant stenting and cardiac surgical procedures. 5 The literature lacks studies that compare long-term results of simultaneous CA revascularisation by stenting or endarterectomy in patients who underwent coronary artery bypass grafting.
Study limitations
A significant limitation is the small number of participants, which decreased the power of the study. Preoperative characteristics of CA stenosis are significantly different in the compared groups due to a lack of randomisation and risk-adjusted method. Comparing these two techniques is problematic because using them is different for different patients.
The concomitant carotid and coronary artery disease significantly increase the risk of adverse events. In those groups of patients, the best treatment strategy is still a matter of debate. CAS and CEA are the most common therapeutic options. The lack of postoperative results after simultaneous CAS or CEA with CABG is probably due to difficulty comparing two different options. The main guidelines for technique choice are the anatomical characteristics of the aortic arch, supra-aortic vessels, and CA plaque. Our results presented a significantly higher degree of stenosis treated CA and bilateral carotid disease in the CEA + CABG groups. We could be concluded that CEA is a feasible option in the high grade of calcified CA stenosis, where the CAS technique is inferior or impossible due to the high risk of complications. On the other side, CAS reduces postoperative complications, decreases perioperative morbidity, and increases patient recovery. It might be a good option for patients with significant comorbidities and carotid anatomy suitable for CAS (minor degree of calcifications, restenosis, or neck radiation). According to the analysis of all evidence, we consider that each technique has an essential role in CA revascularisation. Appropriate selection of patients, according to indications, contributes to satisfactory short- and long-term results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical approval
The local institutional ethics committee approved the study’s protocol, and all the patients provided written informed consent (Document number 1407, approved date 3 April).
Informed consent
Not applicable.