
Abstract
Background
This study aimed to compare early results in patients who underwent subxiphoid wedge resection with those operated on using a multiportal approach.
Methods
We retrospectively evaluated 151 patients who underwent diagnostic wedge resection for suspected interstitial lung disease. Patients who underwent wedge resection via subxiphoid video-assisted thoracoscopic surgery and conventional video-assisted thoracoscopic surgery were compared.
Results
The study included 90 men (59.6%) and 61 women (40.4%) with a mean age of 54.8 ± 12 years. Of these, 127 patients underwent conventional video-assisted thoracoscopic surgery and 24 patients underwent subxiphoid video-assisted thoracoscopic surgery. Postoperative complications occurred in 13 patients (8.6%), with no significant difference according to surgical technique. Sex was a significant factor in the rate of complications (12.2% in men vs. 3.2% in women). There was no intraoperative mortality; the 30-day mortality rate was 4% (n = 6). Five nonsurviving patients were in the conventional video-assisted thoracoscopic surgery group and 1 was in the subxiphoid video-assisted thoracoscopic surgery group (p = 0.95).
Conclusion
The results of this study indicate that the subxiphoid approach reduced procedure time and length of hospital stay in the early period, while there was no significant difference between the techniques in terms of complications or mortality. Based on these findings, we conclude that surgical outcomes were as successful with the subxiphoid approach as with conventional video-assisted thoracoscopic surgery.
Keywords
Introduction
Developments in surgical technology and techniques have led to changes in the field of thoracic surgery. Video-assisted thoracoscopic surgery (VATS) was performed through multiple ports in the 1990s, whereas today, lung resections are performed using a single incision.1–3 In particular, technological advances have begun to reduce the problem of movement restriction in VATS. Therefore, surgeons are now trying methods that use different incisions and approaches that will allow patients to be discharged earlier.4,5
Uniportal surgery has become a widespread practice in modern thoracic surgery. Surgical approaches performed through incisions of just a few centimeters in length yield better early results compared to the multiportal approach. These procedures avoid entering the intercostal area and are believed to cause minimal nerve damage. Some publications have also argued that the subxiphoid approach is as successful as the uniportal approach.6,7 Regarding the subxiphoid VATS technique, it has been reported in the literature that patients are discharged earlier, have shorter hospital stays, and, most importantly, their postoperative quality of life is better than with the conventional intercostal technique.5,8,9 In our clinic, we performed wedge resections using the subxiphoid VATS technique, in addition to the standard VATS wedge resection technique, in patients we operated on for diagnostic surgery from our interstitial lung diseases council who had a preliminary diagnosis of interstitial lung disease. We determined the advantages of this procedure to be a shorter hospital stay and less postoperative pain, and we aimed to evaluate whether this technique is reliable and superior as there are a limited number of studies available in the literature. Sihoe 10 stated that there are not enough publications in the literature about the subxiphoid approach. There may be bias in studies, mainly due to the practice of the subxiphoid technique by experienced surgeons. However, some surgeons still doubt the necessity and safety of the subxiphoid approach. 10 Concern has been raised that reports on these cases may be biased, as they have been published from limited centers. 10
Our aim in this study was to evaluate whether the subxiphoid VATS technique could be safely applied as an alternative to the conventional VATS technique for interstitial lung disease diagnosis. For this reason, we compare the postoperative morbidity and mortality of these techniques.
Materials and methods
Patients with interstitial lung disease who underwent diagnostic wedge resections between January 2012 and July 2021 were retrospectively evaluated. Between these dates, 314 patients were operated on for interstitial lung disease. In our clinic, subxiphoid resections are performed only on the right side. The left-sided approach is not preferred in our clinic because of excessive cardiac compression in left-sided subxiphoid wedge resections. Therefore, only right wedge resections were included to ensure the homogeneity of the study. One-hundred thirty-one patients were operated on the left side, 29 patients started with VATS and converted to thoracotomy, and 3 patients with missing data were excluded. In the subxiphoid group, no patients were converted to thoracotomy. The study included a total of 151 patients who were divided into 2 groups for comparison: patients who underwent subxiphoid VATS (sVATS) wedge resection and those who underwent conventional VATS (cVATS) wedge resection (Figure 1).
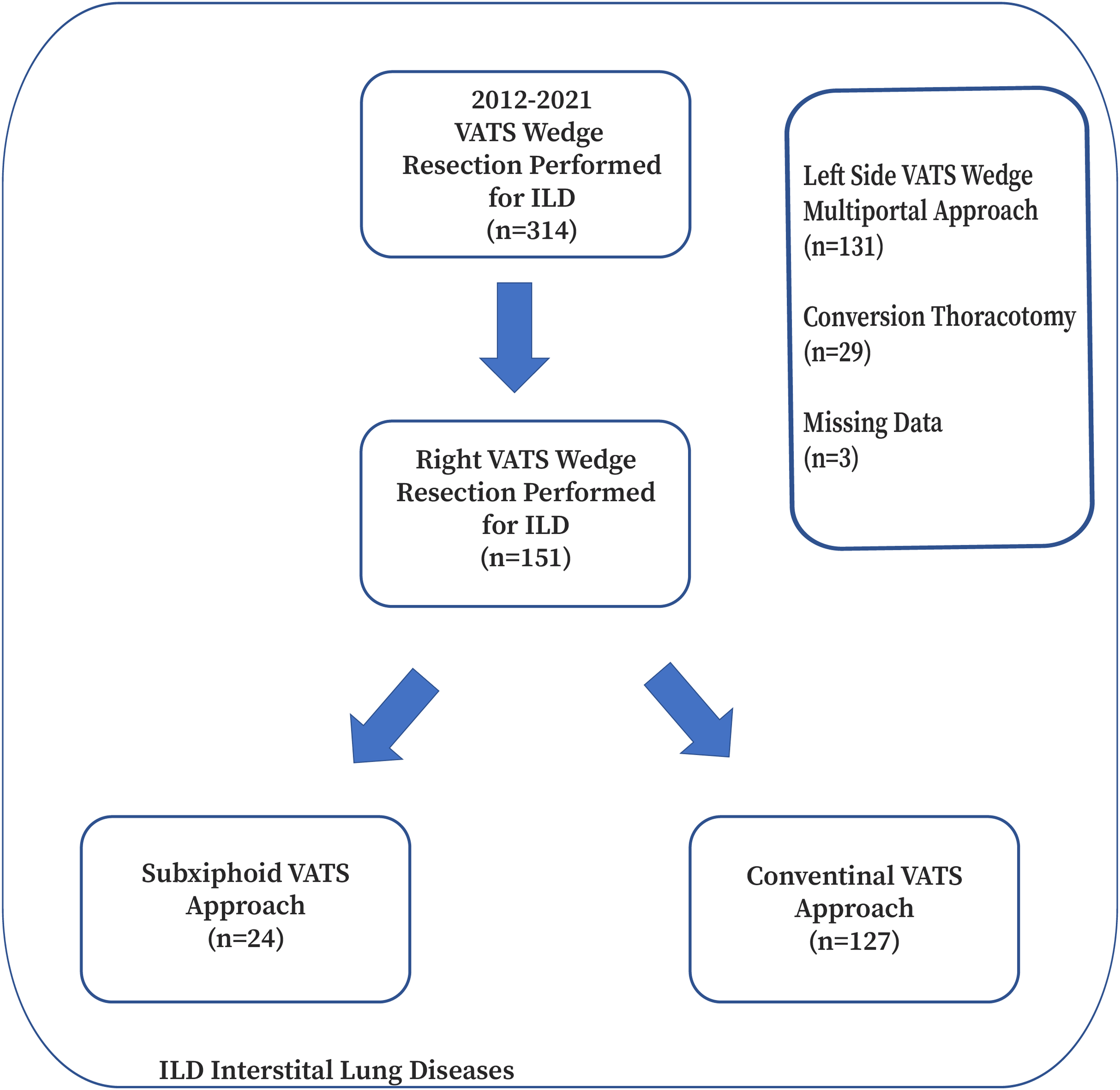
Flow diagram of the study.
Our institution is the reference center for interstitial lung diseases and lung cancers. For this reason, all patients were discussed in our interstitial lung council. At this council, pulmonologists, radiologists, and thoracic surgeons evaluate the patients. After obtaining fiber-optic bronchoscopy (FOB) and bronchoalveolar lavage (BAL) samples during the preoperative period, all patients underwent bronchial mucosal biopsy, transbronchial lung biopsy, and transbronchial needle aspiration (TBNA) in selected cases according to radiological and bronchoscopic appearance. Lung biopsy sides were also selected at the interstitial lung council.
The study was approved by our institutional review board and conducted according to the Declaration of Helsinki principles.
Surgical technique
Thoracic pathologies, adhesions, and diaphragm levels were evaluated using a 30-degree 10-mm thoracoscope (Logic HD, Storz, Germany). In the conventional VATS technique, after induction of anesthesia and intubation with a double-lumen endotracheal tube, the patient was placed in a lateral decubitus position, and a 10-mm camera port was placed in the eighth intercostal space on the anterior axillary line. A 5-cm utility incision was made in the fourth or fifth intercostal space at the anterior border of the latissimus dorsi muscle. Pleural adhesions were severed using ultrasonic shears (Harmonic, Ethicon, Raritan, NJ, USA). Wedge resection was performed in two different lobes (upper and lower) using an endoscopic closure device (endoGIA, Covidien Plc, Norwalk, CT, USA).
Since 2019, patients with interstitial lung disease undergoing diagnostic procedures in the right lung via the subxiphoid approach have been operated on in a 60–70° lateral position. A 4-cm midline incision was made to access the infrasternal area. After separating the subxiphoid adhesion of the rectus abdominis muscle, blunt finger dissection was used to advance to the infrasternal area. Paracardiac fatty tissues were removed with the help of a 30-degree camera (Logic HD, Wolf, Knittlingen, Germany) (Figure 2a,b). After enlarging the mediastinal pleura, the surgical field was enlarged with a wound-protective retractor. Wedge resection was performed by placing endoscopic ring forceps in the middle with the camera at the top and the stapler at the bottom (Figure 3). In our clinic, the subxiphoid approach is applied by only two surgeons. Other surgeons routinely prefer intercostal VATS approaches to interstitial lung diseases.
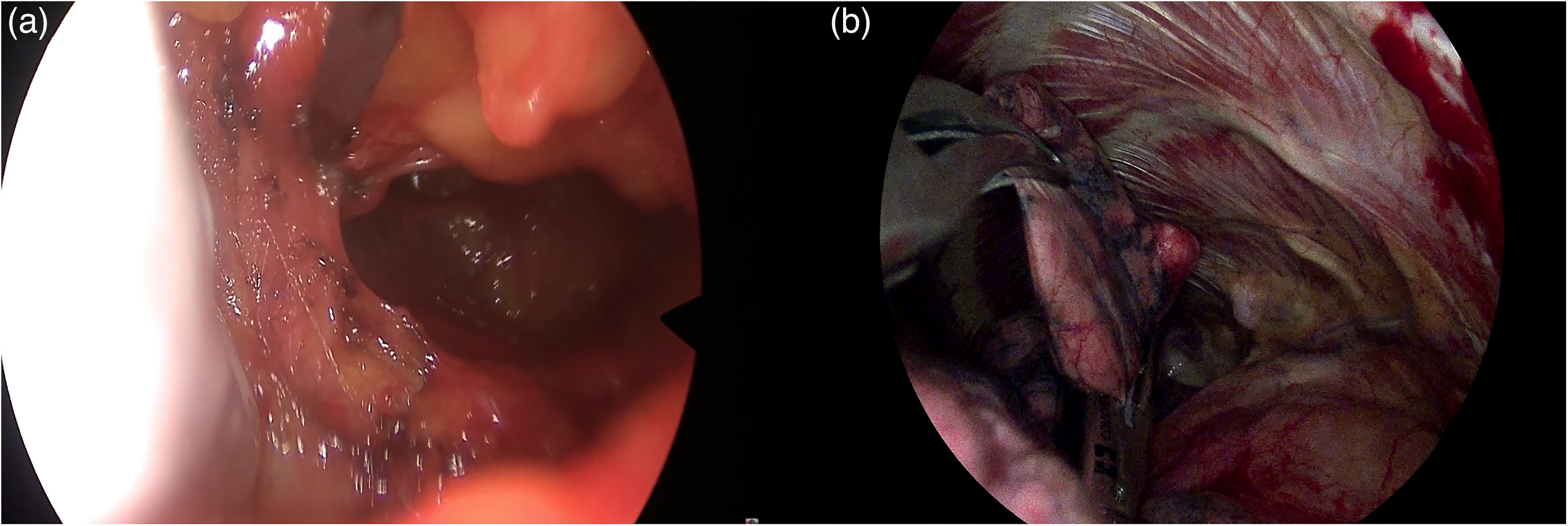
(a) After the mediastinal pleura is opened by blunt finger dissection, the surrounding paracardiac fatty tissues are removed with a cautery or energy device. (b) Lung retraction is performed with an endoscopic oval or banana clamp and wedge resection is also performed with an endolinear stapler.
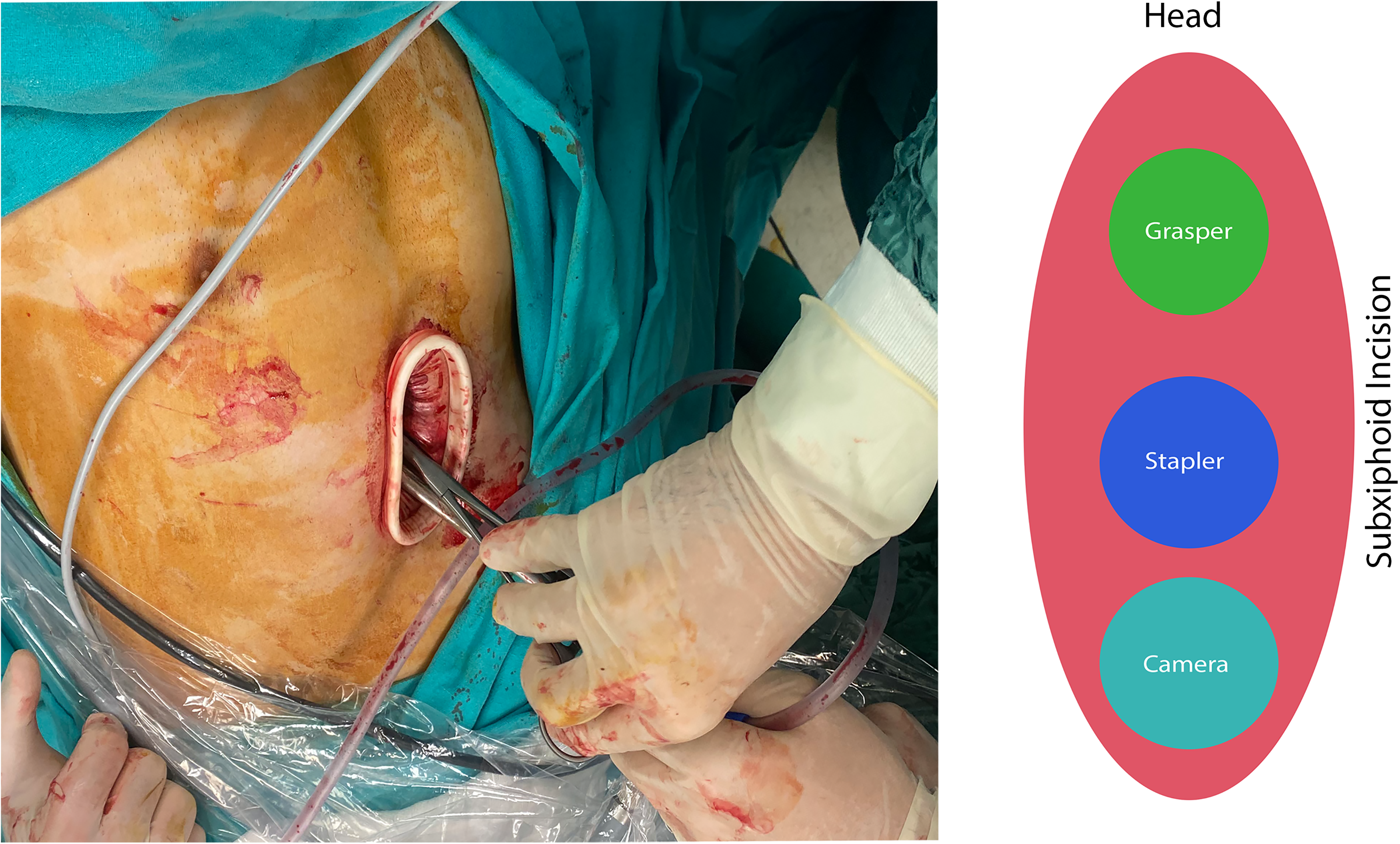
Intraoperative view of the subxiphoid technique (in the subxiphoid technique, a 4-cm midline incision is made to access the infrasternal area). Surgical instruments are arranged with the camera at the bottom, an endoscopic endolinear stapler on top, and endoscopic oval clamp at the top.
Postoperative follow-up
Patients with no cardiac or respiratory problems were monitored postoperatively in the ward. Morbidity was defined as complications that occurred in the hospital, including pneumonia, respiratory failure, pneumothorax after drain removal, prolonged air leak (>7 days), infections requiring surgical site revision, and postoperative hemorrhage.
Mortality was defined as death that occurred in a hospital or within the first postoperative month, including intraoperative death. The hospital information system obtained the patients’ demographic, clinical, and histopathological data. The pulmonologist determined medical treatment based on the patient's postoperative pathology results. Comorbidity was evaluated using the Charlson Comorbidity Index (CCI) and was classified as 0 or ≥1.
Statistical methods
Numerical variables were evaluated using the mean and SD or median, minimum, and maximum values; categorical variables were evaluated using numbers and percentages. Parametric assumptions (normality and homogeneity of variances) were tested before comparing the numerical variables between the groups. Continuous variables were compared using the Mann–Whitney U test. Statistical analyses were performed using IBM SPSS for Windows version 22.0. The level of significance was accepted as p < 0.05.
Results
The study included 90 men (59.6%) and 61 women (40.4%) with a mean age of 54.8 ± 12.5 years. Of the total, 124 patients (82.1%) were under the age of 65 years, and 27 patients (17.9%) were aged 65 years or older. Sixty-seven patients (44.4%) had a history of smoking. The patients’ mean forced expiratory volume in the first second (FEV1) was 1.9 ± 0.7 L, and their mean forced vital capacity (FVC) was 2.2 ± 0.8 l. CCI was 0 in 69 patients (45.7%) and ≥ 1 in 82 patients (54.3%). The mean length of hospital stay was 3.46 ± 2.25 days. There were 127 patients in the cVATS group (84.1%) and 24 patients in the sVATS group (15.9%). When the demographic characteristics were compared with the surgical technique, the median age was 62 years in patients with sVATS and 56 years in patients with cVATS (p < 0.001). In addition, while the hospitalization period of patients who underwent cVATS was 2.5 days, the median length of stay of patients who underwent cVATS was 3 days. While the duration of the operation was 31.4 ± 8.5 min. in patients who underwent sVATS, it was 36.6 ± 11.0 min. in patients who underwent cVATS (p = 0.03). The demographic characteristics and early postoperative outcomes of the subxiphoid and conventional VATS approaches of patients with interstitial lung disease who underwent lung biopsies have been compared in Table 1. The most common pathology found in the study was usual interstitial pneumonia. Usual interstitial pneumonia was detected in 53 patients (35.1%). Table 2 shows the postoperative histopathological features of patients with interstitial lung disease who underwent lung biopsies patients between the groups.
Comparison of demographic characteristics and early postoperative outcomes in subxiphoid and conventional VATS approaches of the patients with interstitial lung disease who underwent lung biopsies.
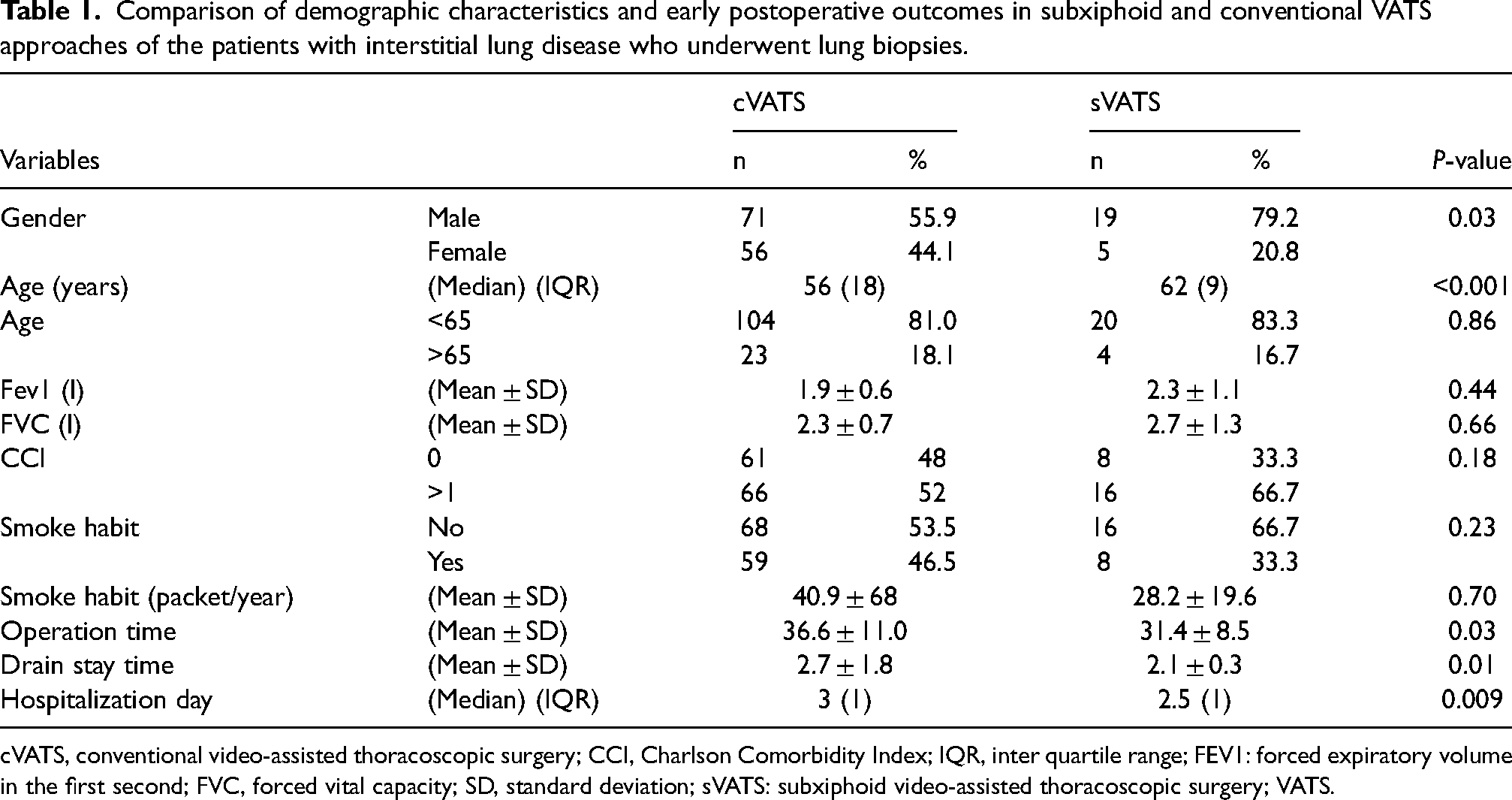
cVATS, conventional video-assisted thoracoscopic surgery; CCI, Charlson Comorbidity Index; IQR, inter quartile range; FEV1: forced expiratory volume in the first second; FVC, forced vital capacity; SD, standard deviation; sVATS: subxiphoid video-assisted thoracoscopic surgery; VATS.
Pathologies of patients operated on for postoperative interstitial lung disease between the groups.
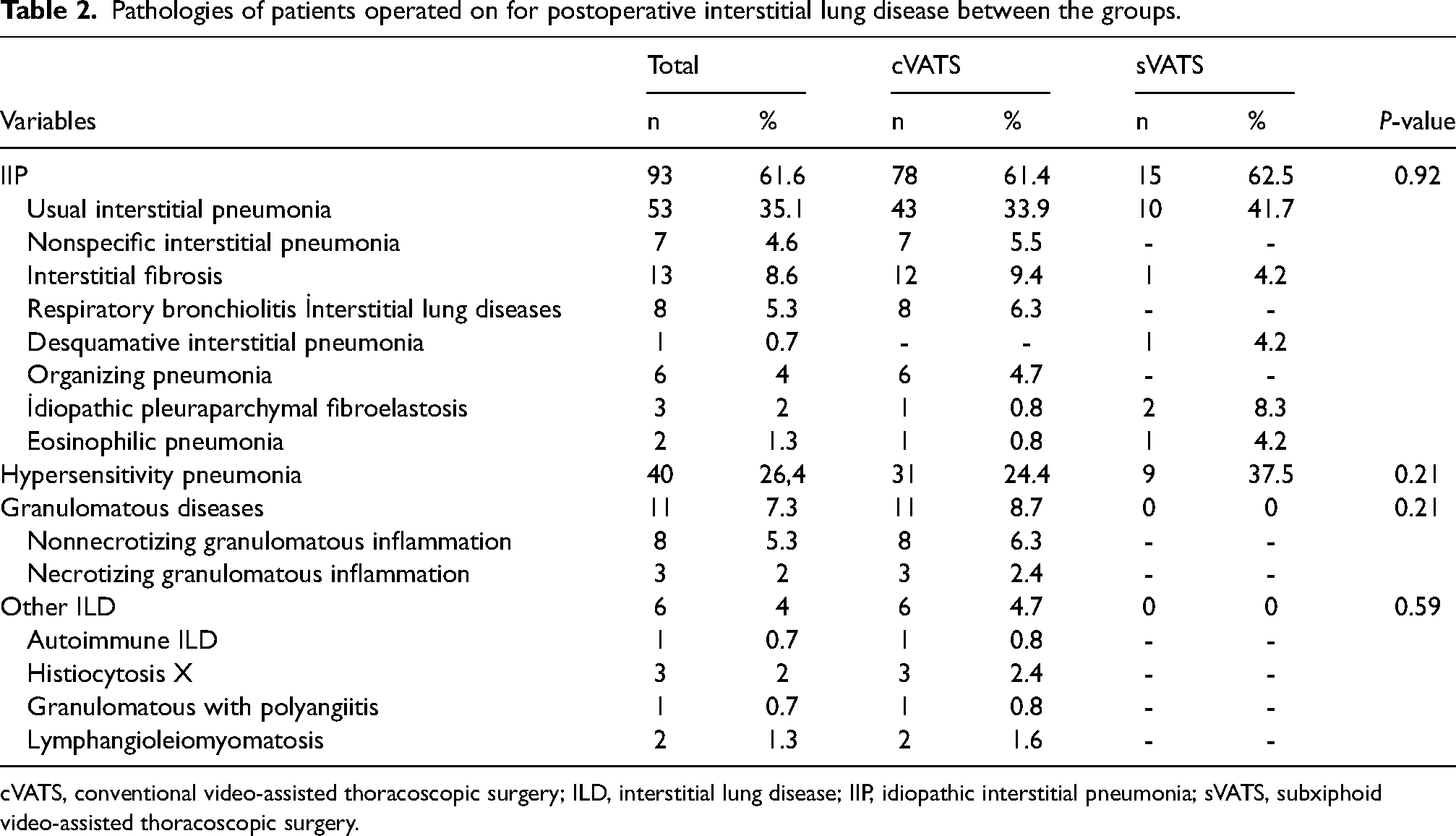
cVATS, conventional video-assisted thoracoscopic surgery; ILD, interstitial lung disease; IIP, idiopathic interstitial pneumonia; sVATS, subxiphoid video-assisted thoracoscopic surgery.
Thirteen patients (8.6%) had postoperative complications. One patient in the sVATS group developed postoperative surgical site infection. In the cVATS group, two patients developed surgical site infection, three patients required mechanical ventilation due to postoperative respiratory failure and developed pneumonia, and three patients experienced prolonged air leaks. Blood pleurodesis was performed in all three patients with prolonged air leaks. Two patients underwent repeated VATS due to bleeding. Two patients underwent repeated tube thoracostomy due to expansion failure after drain removal. Sex was found to be a significant factor associated with postoperative complications, as the complication rate was 12.2% among males and 3.3% among females (p = 0.05). There was no statistically significant difference in complications according to surgical technique (p > 0.05). Factors associated with complications of the patients with interstitial lung diseases who underwent lung biopsies are shown in Table 3.
Prognostic factors affecting complications of the patients with ınterstitial lung disease who underwent lung biopsies.
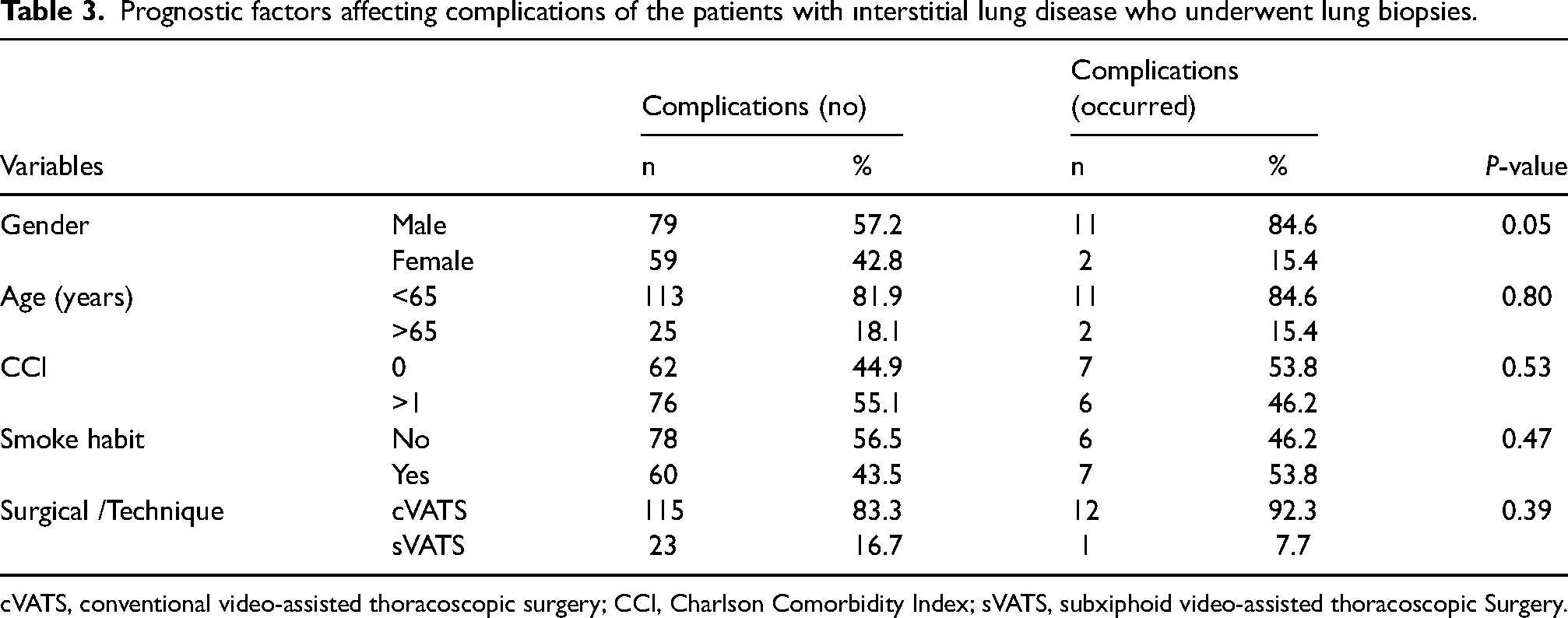
cVATS, conventional video-assisted thoracoscopic surgery; CCI, Charlson Comorbidity Index; sVATS, subxiphoid video-assisted thoracoscopic Surgery.
There was no intraoperative mortality among the patients in this study. Six patients (4%) died within the first 30 days. All of the 6 patients who died had postoperative complications; there was no mortality among the patients who did not develop complications (p < 0.001). Five (83.3%) of the nonsurviving patients were in the cVATS group, and 1 (16.7%) was in the cVATS group (p = 0.95). No statistically significant relationship was observed between demographic characteristics and mortality. Three of the nonsurviving patients underwent invasive mechanical ventilation due to postoperative respiratory failure. All patients who developed pneumonia after intubation died. Myocardial infarction occurred in one patient at postoperative week 3. One patient in the sVATS group and 2 patients in the cVATS group died at postoperative 1 month due to COVID-19. Factors associated with mortality of the patients with interstitial lung diseases who underwent lung biopsies are shown in Table 4.
Prognostic factors affecting mortality of the patients with interstitial lung disease who underwent lung biopsies.
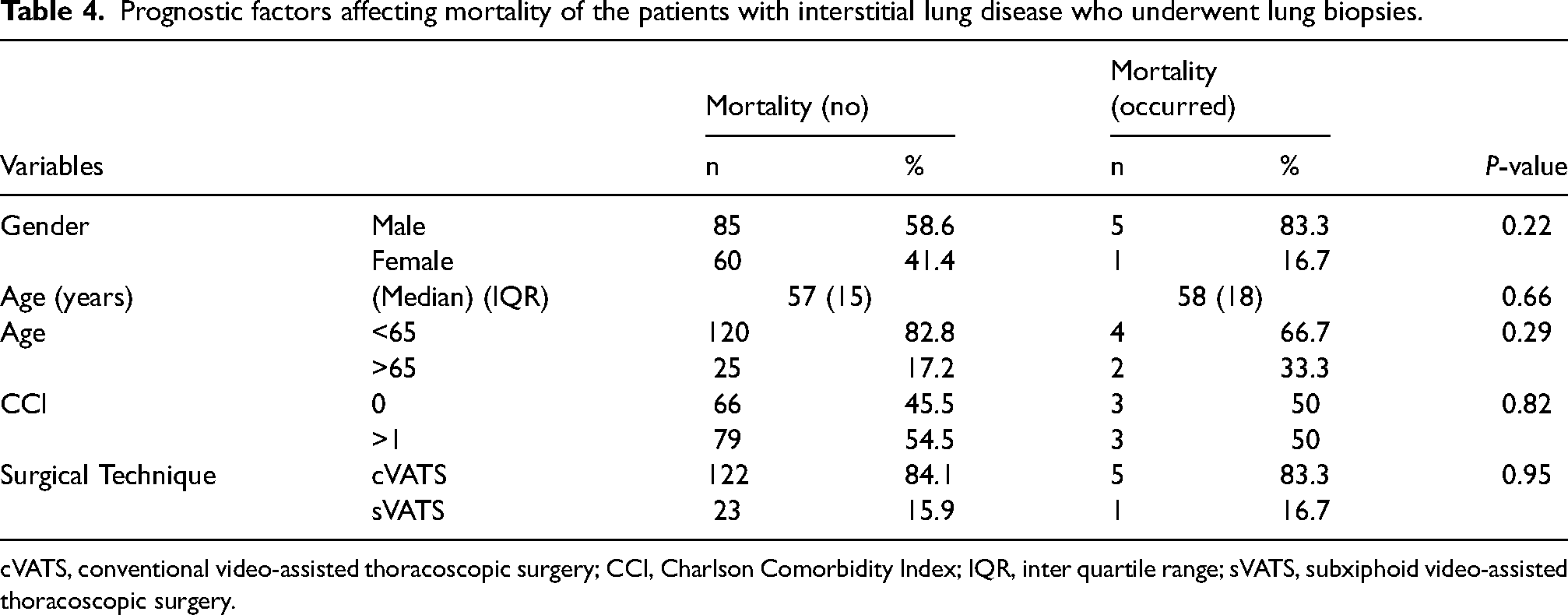
cVATS, conventional video-assisted thoracoscopic surgery; CCI, Charlson Comorbidity Index; IQR, inter quartile range; sVATS, subxiphoid video-assisted thoracoscopic surgery.
Discussion
The uniportal resection approach was first described by Diego Gonzalez-Rivas 11 and led to a different view of VATS in thoracic surgery. With the recent developments in thoracic surgery, even uniportal approaches have become inadequate for surgeons. As surgical techniques advance, subxiphoid VATS approaches are now being attempted. 12 The subxiphoid approach was initially used for thymectomy and wedge resections and was later applied in anatomical lung resections.6,13–16
Suda et al. 17 showed in their study that bilateral wedge resections (metastasectomy) could be performed safely via the subxiphoid approach in patients with bilateral lung tumors. They found that this method provided a reduction in postoperative pain, better cosmetic results, shorter hospital stays, and shorter procedure times after completing the learning curve. They proposed that the subxiphoid method, which is considered appropriate for bilateral metastasectomy and pneumothorax surgery, can also be used easily in unilateral wedge resections. In another study by the same author, a comparison of lateral VATS and subxiphoid VATS thymectomy procedures showed that patients who were operated on using the uniportal subxiphoid approach had shorter procedure time, less estimated hemorrhage, shorter hospital stay, and shorter duration of postoperative analgesia use. 18 In a report by Negi et al., 19 it was emphasized that the shorter surgery and total treatment times with subxiphoid VATS compared to the conventional method are advantageous for patients.
According to the study of Li et al.14 there is no statistical difference between intercostal and subxiphoid surgical approaches in spontaneous pneumothorax patients for hospital stay and drainage time. In addition, pain in the early postoperative period was found to be much less in the subxiphoid approach. In our study, the hospitalization period and drainage days were observed to be less in patients who were operated on using the subxiphoid approach. We think that the most important reason for this is the reduced pain in patients.
However, other authors have presented different views on the subxiphoid approach. In their study of patients who underwent wedge resection, Chen et al. 20 observed comparable length of hospital stay, duration of drain placement, and postoperative recurrence rates between conventional and subxiphoid VATS methods but significantly longer procedure time for subxiphoid VATS (p = 0.004). Cardiac complications were also reported to be more common with the subxiphoid method. In contrast to these studies, we compared conventional and subxiphoid VATS in patients who underwent wedge due to interstitial lung disease and observed a shorter length of hospital stay, drain duration, and procedure time with the subxiphoid approach (p = 0.009). In our center, operations were traditionally performed using conventional VATS and, in recent years, with uniportal VATS techniques. We believe that our shorter operative time using the subxiphoid technique can be attributed to our having considerable experience with uniportal VATS and completing the learning curve.
The rate of postoperative complications in patients using the subxiphoid VATS was similar to that in patients using the conventional method. Yang et al. 21 compared the conventional VATS technique with the subxiphoid VATS method and reported complications in 3 (8.11%) of 37 subxiphoid patients and 6 (8.8%) of 68 three-port VATS patients. There was no significant difference in complications and no mortality in either group at postoperative day 30.
Despite similar complication rates, some authors have reported that cardiac complications are more common with the subxiphoid method. In an analysis by Chen, 20 arrhythmia was significantly more frequent after subxiphoid VATS than conventional VATS (21.9% vs. 0%, p = 0.011). In contrast, a comparison of complications and mortality in our study showed that although neither technique was statistically superior, the complication rate was lower in the subxiphoid approach compared to the conventional method. Only one patient who underwent subxiphoid VATS developed complications. We attribute the lack of a statistically significant difference to the small number of patients in the subxiphoid group. Our previous study compared thoracotomy and conventional VATS techniques in patients with interstitial lung disease and observed similar postoperative complications and mortality rates. 22 As studies on wedge resection via the subxiphoid approach for the diagnosis of interstitial disease are rare in the literature, we believe that our study brings a unique perspective on this point. Given the low complication rates and shorter hospital stay, procedure time, and drain duration, we recommend the subxiphoid VATS technique to patients undergoing diagnostic VATS due to interstitial lung disease. In addition, we detected no atrial fibrillation or intraoperative arrhythmia due to cardiac compression in the patients treated by the subxiphoid approach. In the literature, we believe the use of multiple instruments in resection procedures increased cardiac compression, which in turn led to intraoperative arrhythmia.
The most significant difference between the subxiphoid technique and the conventional technique is the difficulty in finding suitable angles in the surgical field. There may be jamming and interference when using multiple surgical instruments. Moreover, customized uniportal tools are required to perform the technique. We consider this to be the most important disadvantage of the technique. Gonzalez-Rivas et al. 23 also emphasized that experience with uniportal surgery is particularly necessary for this surgery and that the simultaneous use of endoscopic instruments would make these operations easier.
Limitations
The main limitations of this study are its retrospective nature, the inability to perform multivariate analysis due to the small number of patients, and the inability to evaluate the patient's postoperative pain. Moreover, we did not compare the diagnosis of interstitial lung disease subgroups because of the small sample size. The fact that the subxiphoid approach was applied by only two surgeons in the study was also one of the limitations. In our study, we found that the subxiphoid resection operation times were shorter than those using conventional techniques. In addition, surgeons who performed the subxiphoid surgeries in our study had more experience than the conventional techniques surgeons. This could be a potential reason for the increase in bias of the study. Furthermore, only the subxiphoid approach and right-sided VATS wedge approaches are preferred in our clinic. We did not prefer the left-sided subxiphoid approach because of the cardiac compression on the left side. Therefore, the inclusion of only the patients who underwent right VATS wedge resection in the study could lead to a selection bias.
Conclusion
Our results showed that the subxiphoid VATS approach reduced the procedure time and the length of hospital stay but did not differ from the conventional approach in terms of complications and mortality. For this reason, we think that the subxiphoid approach was a safe and alternative technique for wedge resection for interstitial lung diseases. However, prospective randomized studies are still needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by our institutional review board and conducted according to the Declaration of Helsinki principles (Registration Number 2021-139).
Informed consent
Informed consent is provided in this manuscript.